Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Aortic stenosis wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Heart failure wikipedia , lookup
Electrocardiography wikipedia , lookup
Myocardial infarction wikipedia , lookup
Rheumatic fever wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Congenital heart defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Atrial septal defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
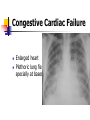
Approach to child with heart disease Pushpa Raj Sharma Professor of Child Health Institute of Medicine Diseases of heart Blood vessels Endocardium Myocardium Pericardium Prevalence Congenital Cyanotic: 22% Acyanotic: 68% VSD ASD PDA TOF PS AS 25% 6% 6% 5% 5% 5% Acquired Kawasaki disease Rheumatic Tubercular Collagen Ceylon Med J 2001 Sep; 46 (3): 96-8; Indian J Pediatr. 2001 Aug;68 (8):757-7 Nelson’s Textbook of pediatrics; 17 ed. Common acyanotic lesions Ventricular septal defects Atrial septal defects Atrio-ventricular septal defects Patent ductus arteriosus Truncus arteriosus Pulmonary stenosis Aortic stenosis Mitral stenosis/incompetence Coarctation of aorta Tricuspid regurgitation Common Cyanotic Lesions Decreased flow 1. Tetralogy of Fallot 2. Tricuspid Atresia 3. Severe Pulmonic Stenosis 4. Ebstein’s anamoly Increased Flow 5. Transposition of great vessles 6. VSD with pulmonary atresia Common Lesions producing cyanosis 7. Truncus Arteriosus 8. Hypoplastic left heart 9. Single ventricle 10. TAPVR with infradiaphragmatic obstruction Presenting complaints/signs Fast breathing Failure to thrive Oedema Exercise intolerence Hepatomegaly, Easy fatigability spleenomegaly Chest indrawing Clubbing Sweating during feeding Cyanosis Bluish spells Focal neurological lesion Fever with rigor Other organ defects Palpitation Chromosomal anomalies Convulsion Cyanosis: is it a cardiac cause or lung cause Hyperoxia test Neonates with cyanotic congenital heart disease usually do not have significantly raised arterial Pao2 during administration of 100% oxygen. Ventricular Defect Small VSD Asymptomatic A loud, harsh, or blowing holosystolic murmur. Large VSD dyspnea, feeding difficulties, poor growth, profuse perspiration, recurrent pulmonary infections, and cardiac failure in early infancy. Syndromes associated with this condition 80% VSD: ECG is normal but may show right ventricular hypertrophy, if present indicates defect is large and presence of pulmonary hypertension or pulmonry stenosis Ventricular Septal Defect (VSD) Small VSDs, the chest radiograph is usually normal Large VSD: The presence of right ventricular hypertrophy, olegeimic lung fields (pulmonary hypertension or an associated pulmonic stenosis), gross cardiomegaly with prominence of both ventricles, the left atrium. Ventricular Septal defects 30–50% of small defects close spontaneously, most frequently during the 1st 2 yr of life. Small muscular VSDs are more likely to close (up to 80%) than membranous VSDs are (up to 35%). infants with large defects have repeated episodes of respiratory infection and heart failure despite optimal medical management. Surgical repair prior to development of an irreversible increase in pulmonary vasculalr resistance (usually prior to the patient's second birthday). Atrial Septal Defects: secundum Most common form of ASD (fossa ovalis) In large defects, a considerable shunt of oxygenated blood flows from the left to the right atrium. Mostly asymptomatic The 2nd heart sound is characteristically widely split and fixed. Secundum Atrial Septal Defects:primum Situated in the lower portion of the atrial septum and overlies the mitral and tricuspid valves. In most instances, a cleft in the anterior leaflet of the mitral valve is also noted. Combination of a left-toright shunt across the atrial defect and mitral insufficiency C/F similar to that of an ostium secundum ASD Atrial Septal Defect Enlargement of the right ventricle Enlargement of atrium Large pulmonary artery increased pulmonary vascularity is. The electrocardiogram in patients with a complete AV septal defect is distinctive. The principal abnormalities are (1) superior orientation of the mean frontal QRS axis with left axis deviation to the left upper or right upper quadrant, (2) counterclockwise inscription of the superiorly oriented QRS vector loop, (3) signs of biventricular hypertrophy or isolated right ventricular hypertrophy, (4) right ventricular conduction delay (RSR′ pattern in leads V3 R and V1 ), (5) normal or tall P waves, and (6) occasional prolongation of the P-R interval Atrial Septal Defects Secundum ASDs are well tolerated during childhood. Antibiotic prophylaxis for isolated secundum ASDs is not recommended. Surgery or transcatheter device closure is advised for all symptomatic patients and also for asymptomatic patients with a Qp:Qs ratio of at least 2:1. Ostium primum defects are approached surgically Patent Ductus Arteriosus Small defect no symptoms. Large defect: Wide pulse pressure Enlarged heart Thrill in L second IS Continuous murmur X-ray: prominent pulmonary artery with increased vascular markings. Primary Pulmonary Hypertension Prominent pulmonary artery. Prominent right ventricle Prominent vascularity in the hilar areas Decreased vascualr marking in the periphery. No treatment Mitral insufficiency: Rheumatic High volume load Enlarged left ventricles Inflammatory process Dilatation of the left atrium Pulmonary congestion Spontaneous improvement Repeated insult Symptoms of left sided failure Chronic mitral insufficiency Symptoms of right heart failure Raised Pulmonary AP Enlarged right ventricle and atrium Mitral insufficiency: Rheumatic Signs of heart failure Heaving apical impulse Apical systolic thrill Accentuated 2nd sound Holosystolic murmur radiating to axilla ECG: bifid P waves and left ventricular hyertrophy X-ray: prominent left atrium and ventricle (straight left border) Prophylaxis against recurrence of rheumatic fever Rheumatic valvular disease: Mitral stenosis Takes 10 years to develop Symptoms proportionate to severity Left ventricular failure right ventricular failure Loud first heart sound with opening snap. Diastolic murmur Absent murmur if heart failure. Surgical intervention if symptomatic Mitral Stenosis Loud 1st sound Diastolic murmur left atrial enlargement prominence of the pulmonary artery enlarged right-sided heart chambers; ECG: prominent notched P wave. Pericardial Effusion Presenting complaint Precordial pain Cough Dyspnoea Abdominal pain Vomiting Fever Other organs involvement Signs: Position: leaning forward. Puffy face Friction rub Absent apical impulse Muffled heart sounds Pulsus paradoxus Distended neck veins Low QRS complex, T inversion Pericardial Effusion A relatively large pericardial effusion must be present to cause an enlarged cardiac shadow with the usual “water bottle” configuration on a chest roentgenogram The test that differentiates The cardiac seize and the vascularity in the chest X-ray Cardiac disease with normal/decreased vasculature Viral myocarditis Tetralogy of Fallot Pulmonary atresia Tricuspid atresia Endocardial fibroelastosis Aberrant left coronary artery Cystic medial necrosis Diabetic mother Tetralogy of Fallot Ventricular septal defect Pulmonic stenosis Overriding aorta Right ventricular hypertrophy Cyanotic Cardiac disease with increased vasculature Atrioventricular septal defects Congestive cardiac failure Transposition of great arteries with VSD Total anomalous pulmonary venous drainage Truncus arteriosus Single ventricle without pulmonary stenosis Hypoplastic left heart syndrome Congestive Cardiac Failure Enlarged heart Plethoric lung fields specially at bases