Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Coronary artery disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Heart failure wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
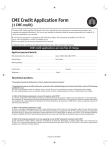
+Model ARTICLE IN PRESS ACVD-880; No. of Pages 11 Archives of Cardiovascular Disease (2016) xxx, xxx—xxx Available online at ScienceDirect www.sciencedirect.com CLINICAL RESEARCH Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors Dysfonction ventriculaire droite chez les patients avec cardiomyopathie dilatée idiopathique : valeur pronostique et facteurs prédictifs Clement Venner a, Christine Selton-Suty a, Olivier Huttin a, Marie-Line Erpelding b, Etienne Aliot a, Yves Juillière a,∗ a Department of Cardiology, institut lorrain du cœur et des vaisseaux, University Hospital of Nancy, Vandœuvre-lès-Nancy, France b Department of Clinical Epidemiology and Evaluation, S2R Centre, ESPRI, University Hospital of Nancy, Nancy, France Received 4 June 2015; received in revised form 3 August 2015; accepted 14 October 2015 KEYWORDS Right ventricular dysfunction; Dilated cardiomyopathy; Propensity analysis; Heart failure Summary Background. — Right ventricular (RV) dysfunction is an important predictor of impaired prognosis in idiopathic dilated cardiomyopathy. Aims. — To determine the prognostic role of RV dysfunction, independent of left ventricular (LV) dysfunction. Methods. — A total of 136 consecutive patients (73% men; mean age 59.0 ± 13.2 years) with idiopathic dilated cardiomyopathy (LV ejection fraction ≤ 45%) were enrolled retrospectively. Thirty-four patients (25%, group 1) presented with RV dysfunction, defined as tricuspid annular plane systolic excursion (TAPSE) ≤ 15 mm; 102 patients (group 2) had preserved RV function. Abbreviations: CI, confidence interval; DCM, dilated cardiomyopathy; DT, deceleration time; FAC, fractional area change; HF, heart failure; HR, hazard ratio; LV, left ventricular; LVEF, left ventricular ejection fraction; LVOT, left ventricular outflow tract; MACE, major adverse cardiac events; MRI, magnetic resonance imaging; OR, odds ratio; RV, right ventricular; RVEF, right ventricular ejection fraction; sPAP, systolic pulmonary artery pressure; TAPSE, tricuspid annular plane systolic excursion; TR, tricuspid regurgitation; TVI, time-velocity integral. ∗ Corresponding author at: Department of Cardiology, institut lorrain du cœur et des vaisseaux, CHU Nancy—Brabois, rue du Morvan, 54511 Vandœuvre-lès-Nancy, France. E-mail address: [email protected] (Y. Juillière). http://dx.doi.org/10.1016/j.acvd.2015.10.006 1875-2136/© 2015 Elsevier Masson SAS. All rights reserved. Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS 2 C. Venner et al. Results. — Mean LV ejection fraction was 27.5 ± 8.7%. Mean TAPSE was 18.6 ± 5.4 mm (15—21.8 mm). Multivariable predictors of RV dysfunction were LV outflow tract time-velocity integral (odds ratio 0.8, 95% confidence interval [CI] 0.7—0.9; P = 0.003) and E-wave deceleration time ≤ 145 ms (odds ratio 4.1, 95% CI 1.3—12.8; P = 0.017). Major adverse cardiac event-free survival rates at 1 and 2 years were 64% and 55%, respectively, in group 1 and 87% and 79%, respectively, in group 2 (P = 0.002). Both by multivariable analysis and after stratification using a propensity score, RV dysfunction emerged as an independent predictor for major adverse cardiac events (hazard ratio 3.2, 95% CI 1.3—7.6; P = 0.009), along with right atrium area and age. Conclusion. — In idiopathic dilated cardiomyopathy, RV dysfunction with TAPSE ≤ 15 mm offers additional prognostic information, independent of the extent of LV dysfunction. © 2015 Elsevier Masson SAS. All rights reserved. MOTS CLÉS Dysfonction ventriculaire droite ; Cardiomyopathie dilatée ; Analyse de propensité ; Insuffisance cardiaque Résumé But. — La dysfonction ventriculaire droite (VD) est un facteur prédictif important de l’altération du pronostic dans la cardiomyopathie dilatée (CMD) idiopathique. Le but était de déterminer le rôle pronostique de la dysfonction VD indépendamment du niveau de dysfonction ventriculaire gauche (VG). Méthodes. — Au total, 136 patients consécutifs (73 % d’hommes, âge moyen : 59,0 ± 13,2 ans) avec CMD idiopathique (FEVG ≤ 45 %) étaient inclus rétrospectivement. Trente-quatre patients (25 %, groupe 1) présentaient une dysfonction VD définie par une excursion systolique du plan de l’anneau tricuspide (TAPSE) ≤ 15 mm et 102 (groupe 2) avaient une fonction VD préservée. Résultats. — La FEVG moyenne était de 27,5 ± 8,7 %. Le TAPSE moyen était de 18,6 ± 5,4 mm (15—21,8 mm). Les facteurs prédictifs de la dysfonction VD en analyse multivariée étaient l’intégrale temps-vélocité (TVI) de la chambre de chasse du VG (OR 0,8 [95 % IC, 0,7—0,9], p = 0,003) et le temps de décélération de l’onde E ≤ 145 ms (OR 4,1 [95 % IC, 1,3—12,8], p = 0,017). La survie sans événements cardiaques majeurs (MACE) à 1 et 2 ans était respectivement de 64 % et 55 % dans le groupe 1 et de 87 % et 79 % dans le groupe 2 (p = 0,002). Après analyse multivariée et stratification en utilisant un score de propensité, la dysfonction VD apparaissait comme un facteur prédictif indépendant des MACE (HR 3,2 [95 % IC, 1,3—7,6], p = 0,009), en plus de la surface de l’oreillette droite et de l’âge. Conclusion. — Dans la CMD idiopathique, la dysfonction VD définie par un TAPSE ≤ 15 mm offre une information pronostique additionnelle indépendante du niveau de dysfonction VG. © 2015 Elsevier Masson SAS. Tous droits réservés. Background Idiopathic dilated cardiomyopathy (DCM) is the second most frequent cause of heart failure (HF). Despite recent changes in diagnosis and treatment of HF, prediction of prognosis remains uncertain from one patient to another [1—3]. The effect of left ventricular (LV) function on outcome in HF has been well documented [2—5]. Furthermore, the new variables of myocardial deformation obtained by two- and three-dimensional speckle tracking give additional prognostic information [6,7]. Right ventricular (RV) performance is connected to LV dysfunction in multiple ways (shared fibres and septal wall, biventricular cardiomyopathic process, increased LV filling pressures, ventricular interdependence and inextensible pericardial space) [8,9]. Evaluation of RV performance remains challenging in routine practice and, as a result, RV function has long been neglected [8—10]. Progress in echocardiography has helped to redefine the importance of RV evaluation for further risk stratification [11,12]. The prevalence of RV dysfunction in DCM varies from 34 to 65% [13,14]. Several studies have demonstrated the additional prognostic value of RV dysfunction in HF and, most particularly, in idiopathic DCM [15—18]. Propensity analyses are rarely used in clinical studies; they are mostly used in pharmacological and epidemiological studies, to counter the effect of potential confounding bias caused by the indication for treatment. The use of a propensity analysis in this context could provide further information about the prognostic role of RV dysfunction, independent of the level of LV dysfunction, and also about the factors associated with RV function [19,20]. Such an analysis has not been performed in primary DCM. The aim of our study was to establish the prevalence of RV dysfunction in a consecutive series of patients with idiopathic DCM, based on tricuspid annular plane systolic Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS RV dysfunction in idiopathic dilated cardiomyopathy excursion (TAPSE), and to identify its determinants and incremental prognostic effect for a given range of LV dysfunction, using a propensity analysis. Methods Study population Between 1st January 2010 and 1st January 2012, we retrospectively selected 790 patients who had been referred to our institution, and for whom the primary or associated PMSI (Programme Médicalisé des Systèmes d’Information) diagnosis was DCM. In order to isolate idiopathic DCM, this database was crossed with hospitalization records, clinical and echocardiographic data. Exclusion criteria were defined to precisely distinguish idiopathic DCM from all other causes of LV dysfunction or dilatation, and required a systematic review of coronary angiograms. Ischaemic substrate was defined as any stenosis ≥ 50% in either of the main coronary arteries or in one of their main side branches. Data from patients with insufficient echocardiography or examination performed in an unstable clinical state were not retained for analysis (n = 92). When the initial cause of hospitalization was acute HF, the echocardiography assessment at discharge was retained. Data from 136 patients presenting with idiopathic DCM were available for analysis. Follow-up Follow-up was censored on 1st January 2014, and consisted of a telephone interview with the patient’s general physician. For all patients, we recorded data on the presence and date of occurrence of all major adverse cardiac events (MACE), defined as a composite criterion, including death from cardiac cause (sudden cardiac death, ventricular tachycardia, acute HF), heart transplantation and cardiacrelated hospitalizations. The delay from the first hospitalization between January 2010 and January 2012 to the first event was retained for survival analysis. Echocardiographic assessment Transthoracic echocardiograms were recorded on various generations of Vivid systems (GE Vingmed Ultrasound, Horten, Norway), and analyses were performed off-line on an EchoPAC workstation (GE Healthcare, Milwaukee, MI, USA). Measurements were made according to guidelines [21,22]. LV ejection fraction (LVEF) was measured according to Simpson’s method. DCM was defined as LVEF ≤ 45% and left ventricular end-diastolic diameter ≥ 55 mm. Global peak systolic longitudinal strain was assessed by two-dimensional speckle imaging in the apical four-chamber view. Diastolic function analysis was based on mitral-pulsed Doppler inflow and tissue-Doppler imaging at the lateral mitral annulus. A restrictive pattern was defined as E-wave deceleration time (DT) < 145 ms — the median value and in concordance with previous studies [23,24]. Left and right atrial areas were measured from the apical four-chamber view. 3 TAPSE was measured by M-mode, after two-dimensional echocardiography guidance at the lateral tricuspid annulus, as the maximal systolic excursion. Tissue Doppler imaging at the tricuspid annular free wall allowed the assessment of S-wave velocity. Fractional area change (FAC) in the right ventricle was obtained according to image quality. Systolic pulmonary artery pressure was calculated from tricuspid regurgitation (TR) flow added to right atrial pressure estimated from the inferior vena cava. Right and left atrial areas were measured at end-ventricular systole in a four-chamber view. Cardiac magnetic resonance imaging assessment Thirty-seven patients (27.2%) underwent cardiac magnetic resonance imaging (MRI), performed using a 1.5-Tesla MRI scanner (Signa HDxt; GE Healthcare, Milwaukee, WI, USA) connected to an eight-element cardiac phased-array surface coil. Cine images were obtained with a steady-state free precession sequence in base-to-apex contiguous short-axis slices for volume and mass quantification. Statistical analysis All continuous variables are described as means ± standard deviations; all categorical variables are described with absolute and relative frequencies. Intra- and interobserver variabilities of measure were assessed using a Bland-Altman diagram for TAPSE. A receiver operating characteristic curve was built to define an appropriate threshold for TAPSE, based on gold-standard cardiac MRI-derived RV ejection fraction (RVEF). The area under the curve of the model was 0.63, and the most pertinent value was 15.4 mm (Se 0.86; 1—Sp 0.44). RV dysfunction was defined by TAPSE ≤ 15 mm, and patients were divided into two groups according to the presence (group 1) or absence (group 2) of RV dysfunction. Comparisons according to the presence or absence of RV dysfunction and the occurrence of MACE were realized with Student’s t test for continuous variables and the Chi2 test for discrete variables. Bivariate and multivariable logistic regressions were used to identify determinants of RV dysfunction. In the multivariable model, LVEF, LV end-diastolic diameter and age were forced, and a stepwise variable selection method, with a P value < 0.1 to enter the stepwise selection and a P value < 0.05 to remain in the final model, was applied. Results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs). To assess the prognostic effect of RV dysfunction on the occurrence of MACE, several analyses were used. Survival curves according to the presence or absence of RV dysfunction were generated by the Kaplan-Meier method, and were compared using log-rank tests. Next, bivariate and multivariable Cox regression analyses were used to assess predictors of MACE, particularly including RV dysfunction as a dependent variable. Finally, to take into account the likely imbalance in the baseline characteristics of patients with or without RV dysfunction and, more specifically, to address the effect of the extent of LV dysfunction on RV dysfunction, we used Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS 4 C. Venner et al. a propensity analysis [20]. Propensity scores of RV dysfunction were calculated for each patient, including variables predictive of RV dysfunction obtained by multivariable logistic regression and variables supposed to influence both the presence of RV dysfunction and patient outcome (LVEF, LV end-diastolic diameter and age). A Cox multivariable regression stratified by quintiles of propensity scores was performed to predict the occurrence of MACE. Results are expressed as hazard ratios (HRs) with 95% CIs. For all tests, P < 0.05 was considered significant. All statistical analyses were performed using SAS software, version 9.3 (SAS Institute, Cary, NC, USA). Variables with more than half non-missing values and with correlation with other co-variables < 0.6 were selected for all bivariate analyses. Significant variables in the bivariate analyses were candidates for all multivariable analyses. Results Baseline characteristics Patient characteristics are listed in Table 1. The cause of initial hospitalization was acute HF for 39 patients (28.7%); the others (71.3%) were considered to be in a stable haemodynamic state at inclusion, and most were hospitalized for device implantation, coronary angiography or cardiac rehabilitation. The median duration of disease at inclusion was 2.1 years, with no significant intergroup difference (1.5 years vs 2.6 years for groups 1 and 2, respectively; U test P = 0.66). Mean TAPSE was 18.6 ± 5.4 mm, and the reproducibility of measures was as follows: mean bias −0.15 mm, limit of concordance (−2.2; 1.8) for intraobserver variability; and mean bias −0.19 mm, limit of concordance (−2.8; 2.4) for interobserver variability. Five patients (3.7%) had TAPSE > 30 mm. The mean disease duration for these patients was 8.0 ± 7.8 years; mean B-type natriuretic peptide concentration was 185.8 ± 81.6 pg/mL; mean systolic pulmonary artery pressure (sPAP) was 26.0 ± 17.0 mmHg; and only one had grade 2 TR. None of these patients had been enrolled at the time of an acute HF hospitalization, and all received an angiotensin-converting enzyme inhibitor > 50% maximal dose. These high values of TAPSE were not responsible for an outlier effect, according to Tukey’s method for the detection of outlier values. Patient characteristics according to RV dysfunction and its predictors Differences between groups of patients are listed in Table 1. All echocardiographic and cardiac MRI variables of RV function (S-wave, FAC, right atrial size and RVEF) and LV function (LVEF, four-chamber longitudinal peak systolic strain, LV outflow tract [LVOT] time-velocity integral [TVI] and E-wave DT) were statistically more significantly altered in group 1 than in group 2. By multivariable analysis, E-wave DT ≤ 145 ms (OR 4.1, 95% CI 1.3—12.8; P = 0.017) and LVOT TVI (OR 0.8, 95% CI 0.7—0.9; P = 0.003) were the only factors associated with RV dysfunction (Table 2). Figure 1. Kaplan-Meier survival curves of major adverse cardiac events according to tricuspid annular plane systolic excursion (TAPSE) ≤ or > 15 mm. Association between RV dysfunction and MACE None of the patients were lost to follow-up over a mean of 2.7 ± 1.1 years (371 patient-years). Twenty-four patients (17.6%) died in our cohort: 10 in group 1 (30%) and 14 in group 2 (14%). The cause of death was cardiac-related for 20 patients (eight in group 1; 12 in group 2); the four other deaths were the result of cancer or septic shock. Fortynine patients (36%) presented MACE, consisting of 20 cardiac deaths (14.7%), 16 episodes of acute HF (11.8%), two heart transplantations (1.5%) and 24 cardiac-related hospitalizations (17.6%). Overall, MACE were recorded in 18/34 (53%) patients in group 1 and 31/102 (30%) in group (P = 0.02). The mean time of occurrence of MACE after initial hospitalization was 1.3 ± 1.0 years. MACE-free survival rates at 1, 2 and 3 years were 64%, 55% and 42% in group 1 compared with 87%, 79% and 68% in group 2, respectively (P = 0.002), as shown in Fig. 1. In a bivariate Cox regression, MACE were associated with age, systolic blood pressure, RV dysfunction, left and right atrial area ≥ 20 cm2 , sPAP and haemoglobin value. By multivariable analysis, only RV dysfunction (HR 2.4, 95% CI 1.3—4.3; P = 0.006), right atrial area ≥ 20 cm2 (HR 2.2, 95% CI 1.1—4.1; P = 0.019) and age (HR 1.03, 95% CI 1.0—1.1; P = 0.041) were associated with an increased risk of MACE (Table 3). After stratification by quintiles of propensity scores, RV dysfunction (HR 3.2, 95% CI 1.3—7.6; P = 0.009), age and right atrial area ≥ 20 cm2 remained the only factors associated with the occurrence of MACE (Table 3). Outcome regarding RV dysfunction and sPAP A higher rate of MACE was observed in patients with RV dysfunction and sPAP > 40 mmHg (Fig. 2). Patients with RV dysfunction had a worse outcome than patients with preserved RV function. Patients with sPAP > 40 mmHg had a worse outcome than patients with sPAP < 40 mmHg. Patients with RV dysfunction and sPAP < 40 mmHg had an intermediate outcome. sPAP was associated with MACE only in the bivariate Cox regression (HR 1.03, 95% CI 1—1.05; P = 0.019), but not in the multivariable model (Table 3). Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS RV dysfunction in idiopathic dilated cardiomyopathy Table 1 5 Patient characteristics according to right ventricular dysfunction. All patients Group 1 (TAPSE ≤ 15 mm) Group 2 (TAPSE > 15 mm) P 59.01 ± 13.24 100 (73.5) 82 (60.2) 58.50 ± 14.40 29 (85.3) 28 (82.4) 59.18 ± 12.89 71 (69.6) 54 (54.5) 0.80 0.07 0.0004a 0.20 Baseline features Age (years) Men Prior acute HF NYHA functional status I—II III IV Systolic blood pressure (mmHg) Sinus rhythm BNP (pg/mL) Peak VO2 (L/min/m2 ) VE/VCO2 (%) Therapy ACEi > 50% maximal dose Beta-blockers > 50% maximal dose Aldosterone antagonists Diuretics > 80 mg/day furosemide ICD CRT 78 (57.3) 48 (35.3) 10 (7.4) 118.81 ± 21.55 115 (84.6) 751.18 ± 912.60 21.38 ± 6.49 35.52 ± 7.01 7 (47.1) 13 (38.2) 5 (14.7) 111.83 ± 16.80 24 (70.6) 1020.93 ± 999.55 23.34 ± 6.20 34.72 ± 5.45 33 (60.8) 35 (34.3) 5 (4.9) 121.53 ± 22.66 91 (89.2) 627.36 ± 849.92 20.69 ± 6.5 35.84 ± 7.57 0.036a 0.009a 0.06 0.14 0.57 120 (88.2) 101 (74.3) 123 (90.4) 68 (50.0) 50 (36.8) 108 (79.4) 46 (33.8) 58 (42.6) 42 (30.9) 29 (85.3) 21 (72.4) 32 (94.1) 12 (38.7) 16 (47.1) 31 (91.2) 17 (54.8) 11 (32.4) 8 (23.5) 91 80 91 56 34 77 29 47 34 0.54 0.046a 0.40 0.016a 0.15 0.05a 0.11 0.16 0.28 Echocardiography: LV LVEDD (mm) LVEF (%) Four-chamber LVEF (%) Four-chamber LPS (%) LVOT TVI (cm/s) E-wave DT (ms) LA surface (cm2 ) MR > grade 2 65.83 ± 9.21 27.51 ± 8.71 26.42 ± 9.29 —8.00 ± 3.98 16.02 ± 5.64 154.94 ± 59.70 25.32 ± 6.95 45 (33.0) 64.68 ± 8.46 24.24 ± 7.93 22.96 ± 8.43 —5.62 ± 2.54 12.28 ± 4.30 119.89 ± 34.42 28.60 ± 7.82 15 (44.1) 66.22 ± 9.46 28.60 ± 8.73 27.58 ± 9.31 —8.73 ± 4.07 17.31 ± 5.48 166.15 ± 61.81 24.24 ± 6.32 30 (29.4) 0.40 0.014a 0.012a < 0.001a < 0.001a < 0.001a 0.002a 0.12 Echocardiography: RV TAPSE (mm) RA surface (cm2 ) TR > grade 2 sPAP (mmHg) S-wave (cm/s) FAC 18.6 ± 5.4 20.84 ± 9.71 17 (12.5) 36.94 ± 12.21 9.71 ± 2.87 0.40 ± 0.14 11.9 ± 2.1 26.85 ± 13.64 8 (23.5) 38.83 ± 10.64 7.76 ± 1.73 0.30 ± 0.12 20.8 ± 4.2 18.82 ± 6.98 9 (8.9) 36.29 ± 12.70 10.39 ± 2.89 0.43 ± 0.13 < 0.001a 0.13 0.34 < 0.001a 0.001a Cardiac MRI LVEF (%) RVEF (%) 28.34 ± 11.20 42.99 ± 17.52 24.82 ± 13.24 32.55 ± 17.67 29.59 ± 10.34 47.41 ± 15.77 0.23 0.016 (89.2) (87.9) (89.2) (63.6) (33.3) (75.5) (38.2) (46.1) (33.3) a Data are expressed as mean ± standard deviation or number (%). ACEi: angiotensin-converting enzyme inhibitor; BMI: body mass index; BNP: brain natriuretic peptide; CRT: cardiac resynchronization therapy; DT: deceleration time; FAC: fractional area change; HF: heart failure; ICD: internal cardiac defibrillator; LA: left atrial; LPS: longitudinal peak systolic strain; LV: left ventricle; LVEDD: left ventricular end-diastolic diameter; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; LVOT: left ventricular outflow tract; MR: mitral regurgitation; MRI: magnetic resonance imaging; NYHA: New York Heart Association; RA: right atrial; RV: right ventricle; RVEDV: right ventricular end-diastolic volume; RVEF: right ventricular ejection fraction; sPAP: systolic pulmonary artery pressure; TAPSE: tricuspid annular plane systolic excursion; TR: tricuspid regurgitation; TVI: time-velocity integral; VCO2 : carbon dioxide consumption; VE: pulmonary ventilation; VO2 : oxygen consumption. a P ≤ 0.05. Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ARTICLE IN PRESS ACVD-880; No. of Pages 11 6 C. Venner et al. Table 2 Factors associated with tricuspid annular plane systolic excursion ≤ 15 mm. N TAPSE ≤ 15 mm Bivariate regression n % OR 95% CI P OR 95% CI P Multivariable regression Age 136 34 25 1 0.97—1.03 0.80 1.02 0.99—1.06 0.23 LVEDD 134 34 25.4 0.98 0.94—1.03 0.40 0.95 0.90—1.01 0.11 Four-chamber LVEF 136 34 25 0.95 0.90—0.99 0.0112 0.98 0.91—1.04 0.49 Heart rate 136 34 25 1.04 1.01—1.07 0.0015 0.84 0.74—0.94 0.0031 Systolic blood pressure < 100 mmHg 100—120 mmHg 120—140 mmHg ≥ 140 mmHg Missing 14 40 27 26 29 5 15 5 5 4 35.7 37.5 18.5 19.2 13.8 1 1.08 0.41 0.43 0.29 CRP > 5 mg/L No Yes Missing 58 53 25 10 18 6 17.2 34 24 1 2.47 1.52 GOT > 30 IU/L No Yes Missing 61 32 43 14 13 7 23 40.6 16.3 1 2.3 0.65 Four-chamber peak systolic longitudinal strain < 10% ≥ 10% Missing Aortic TVI 0.13 0.13 1.02—6.00 0.48—4.75 0.06 0.91—5.79 0.24—1.78 0.0003 75 35 26 25 1 8 33.3 2.86 30.8 1 0.06 0.89 0.01—0.45 0.34—2.32 133 34 25.6 0.81 0.73—0.89 < 0.0001 < 0.0001 E-wave deceleration time ≤ 145 ms > 145 ms 65 67 26 6 40 8.96 6.78 1 E/A <1 1—2 >2 Missing 57 24 28 27 6 4 11 13 10.5 16.7 39.3 48.1 1 1.7 5.5 7.89 LA area < 20 cm2 ≥ 20 cm2 Missing 31 94 11 4 27 3 12.9 28.7 27.3 1 2.72 2.53 RA area < 20 cm2 ≥ 20 cm2 Missing 72 51 13 11 20 3 15.3 39.2 23.1 1 3.58 1.66 ECG sinus rhythm 0.30—3.83 0.09—1.77 0.10—1.85 0.06—1.32 2.56—17.96 0.0165 4.06 1 1.29—12.79 0.0004 0.43—6.67 1.77—17.13 2.54—24.52 0.18 0.87—8.51 0.47—13.75 0.0109 1.52—8.40 0.39—7.03 0.0214 CI: confidence interval; CRP: C-reactive protein; ECG: electrocardiogram; GOT: glutamic oxaloacetic transaminase: LA: left atrial; LVEDD: left ventricular end-diastolic diameter; LVEF: left ventricular ejection fraction; OR: odds ratio; RA: right atrial; TAPSE: tricuspid annular plane systolic excursion; TVI: time-velocity integral. Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 49/136 39/136 48/136 45/136 123/136 49/136 39/136 63.20 111.56 13.34 27.12 20.84 17.29 40.41 ± ± ± ± ± ± ± 13.44 17.41 1.44 7.68 9.71 5.38 14.32 Bivariate Cox analysis Multivariable Cox analysis Multivariable regression stratified on propensity scores OR 95% CI P OR 95% CI P OR 95% CI P 1.04 0.97 0.80 1.05 2.59 0.93 1.03 1.01—1.06 0.96—0.99 0.67—0.97 1.01—1.10 1.41—4.77 0.88—0.99 1.00—1.05 0.0053 0.0025 0.0194 0.0098 0.0022 0.0146 0.0190 1.027 1.001—1.053 0.0406 1.028 1.001—1.056 0.0402 0.851 0.700—1.036 0.11 0.826 0.670—1.071 0.07 2.153 2.350 1.133—4.089 1.273—4.339 0.0191 0.0063 2.241 3.170 1.103—4.553 1.327—7.570 0.0256 0.0094 ARTICLE IN PRESS Age Systolic BP Haemoglobin LA area ≥ 20 cm2 RA area ≥ 20 cm2 RV dysfunction sPAP Mean ± SD +Model n ACVD-880; No. of Pages 11 Factors associated with the occurrence of a major adverse cardiac event. RV dysfunction in idiopathic dilated cardiomyopathy Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 Table 3 7 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS 8 C. Venner et al. Figure 2. Kaplan-Meier survival curves of major adverse cardiac events according to the level of right ventricular function and systolic pulmonary artery pressure (sPAP). TAPSE: tricuspid annular plane systolic excursion. Discussion By defining RV function based on a threshold of TAPSE of 15 mm in DCM patients, our study showed that among various clinical, biological and echocardiographic variables, only E-wave DT and LVOT TVI were significant predictors of RV dysfunction. Furthermore, for the same extent of LV dysfunction by both standard and propensity analyses, RV dysfunction was confirmed to be a factor associated with the occurrence of MACE in patients with DCM, along with right atrial area ≥ 20 cm2 and age. TAPSE and determinants of RV dysfunction TAPSE is probably the most described variable in the echocardiographic evaluation of RV systolic function. Although it may appear reductive to assess RV global function through the displacement of the tricuspid annulus, it is not complete nonsense, as longitudinal shortening of the RV is the main component of RV ejection — the inward motion of RV free wall and the traction by the septum being less contributive [10]. TAPSE was used in our study to define RV dysfunction, as it is the most described variable, but is also the most routinely and easily performed measurement available in practice. In the guidelines, cardiac MRI is recommended as a gold-standard technique to assess biventricular function, but lack of availability remains a limitation [25]. To identify an optimal cut-off value for TAPSE, we used a receiver operating characteristic curve analysis based on an MRI-derived RVEF < 45%. The value we obtained is in concordance with previously published studies analysing adverse outcomes in HF and, particularly, in primary DCM [26,27]. We selected a large panel of clinical, biological, functional and echocardiographic variables suspected to be associated with RV function. In the multivariable analysis, only E-wave DT and aortic TVI remained significantly associated. A decrease in E-wave DT to < 140 ms reflects an increase in left atrial pressure, with a tendency towards a restrictive filling pattern; previous studies have already emphasized this threshold and the importance of diastolic dysfunction on RV function in HF patients [23,24]. Ghio et al. reported the importance of raised filling pressure, with a four-fold increased risk of an event when associated with reduced TAPSE values < 14 mm compared with patients with preserved TAPSE and a non-restrictive filling pattern [23]. The intrinsic evaluation of RV performance remains a challenge with echocardiography. Most of the variables are load dependent and actually depict ventricular function in light of the ventriculoarterial interaction at the time of examination, for a given haemodynamic state. The same limitations apply to tissue Doppler imaging S-wave and FAC, despite their superior value in RV performance assessment compared with TAPSE [12,28]. A recent study emphasized RV free-wall two-dimensional strain and a value < —17% to predict reduced RVEF with high diagnostic accuracy in a comparative assessment along with TAPSE, Swave and FAC [29]. Nevertheless, the performance of this technique in the specific context of idiopathic DCM may raise measurement difficulties (subendocardial definition, RV spherical remodelling), and further studies need to be specifically considered. Ventricular elastance, measured as the ratio of endsystolic arterial pressure (simplified as mean PAP) over end-systolic RV volume, could provide load-independent information about RV intrinsic performance, but requires invasive haemodynamic assessment, as direct evaluation of end-systolic volume remains unachievable with conventional echocardiography. TAPSE values should therefore be interpreted taking into consideration the estimated sPAP value. In the case of normal or moderately elevated values of sPAP (< 40 mmHg), alteration of TAPSE (< 15 mm) probably reflects intrinsic RV dysfunction. In the case of elevated sPAP (≥ 40 mmHg), it seems tendentious to speculate whether the reduction in TAPSE is caused by intrinsic RV dysfunction or is merely the consequence of chronic afterload elevation. In our population, patients with RV dysfunction and elevated sPAP had the poorer prognosis, and patients with preserved RV function had a better outcome regardless of sPAP. These results support those published by Ghio et al., where patients with RV dysfunction and elevated sPAP had a worse survival rate than patients with normal RV function and normal sPAP, and there was an intermediate prognosis for patients with isolated RV dysfunction or elevated sPAP [23]. Determinants of adverse outcome and the role of propensity analysis Our population consisted of consecutive patients enrolled retrospectively, which may in fact have been responsible for a certain degree of heterogeneity, most specifically regarding patients recruited after an acute HF event. Despite this consideration, 71.3% of patients were recruited in a stable haemodynamic state. At the time of inclusion, 88% of patients received an angiotensin-converting enzyme inhibitor (74% had an optimal dose > 50% maximal dose), 90% received a beta-blocker (50% had an optimal dose > 50% maximal dose) and 37% received an aldosterone Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS RV dysfunction in idiopathic dilated cardiomyopathy antagonist. Overall, 34% of patients had a daily dose of furosemide > 80 mg/day. These results are concordant with larger HF registries, such as the French ODIN cohort [30]. We identified age, right atrial area ≥ 20 cm2 and the presence of RV dysfunction as factors associated with an adverse outcome, defined by an increased occurrence of MACE. Sallach et al. had already emphasized the role of right atrial volume index as an independent predictive factor for mortality in HF patients after adjustment for age, LV systolic and diastolic functions, and RV systolic function [31]. The measurement of right atrial volume index is not recommended in recent guidelines, because of the limited data available and the lack of normal values [21]; it may confer more robust and accurate determination of right atrial size over right atrial area, but it is not validated for daily practice. The additional prognostic role of RV function in reducedEF HF has been known since the initial works on thermodilution and isotopic RVEF [15,32,33]. Nevertheless, analysis of the right ventricle often remains neglected compared with that of the left ventricle, because it is difficult to analyse with routine imaging techniques, and probably also because of its retrosternal position and the relative load dependency of standard variables of RV function, as already discussed. However, many variables of RV function and morphology have been shown to be predictors of adverse outcome in patients with HF [13,32,34—36]. In the presence of reduced-EF HF, RV involvement is a distinctive feature of idiopathic DCM, as opposed to other aetiologies of HF, independent of PAP values and LV dysfunction [14,25]. Distinguishing primary DCM from other aetiologies of DCM (predominantly ischaemic cardiomyopathy) was necessary when attempting to directly assess the prognostic effect of RV dysfunction, and more specifically TAPSE. The substrate of RV dysfunction differs between ischaemic and idiopathic DCM; in idiopathic DCM, it mostly reflects a biventricular involvement or the upstream consequence of raised LV filling pressures or raised pulmonary pressures. The pathogenesis of RV dysfunction is more likely heterogeneous in the case of ischaemic cardiomyopathy, depending on the infarct size and the location and duration of the disease. The effect of the ischaemic substrate on TAPSE in previously published studies was reported as either neutral or responsible for a slight drop in values [14,23,37,38]. To avoid further bias we chose to exclude all patients with signs of evolutive or previous myocardial ischaemia. Furthermore, the importance of RV dysfunction in idiopathic DCM had been less specifically addressed. Propensity analyses are generally used in observational studies to assess the effect of one therapy on outcome, in order to eliminate bias caused by confounding factors linked to the indication for this therapy or when the number of confounding variables is high [20]. Propensity analysis is worthy of interest in this context, as it is validated when studying rare outcomes in patients with multiple risk factors. Furthermore, statistical results obtained are less biased, more robust and more precise than a regression approach based on logistic regression [19]. In our case, propensity analysis allowed us to discern the direct effect of RV dysfunction on outcome, independent of factors associated with RV dysfunction (E-wave DT, LVOT TVI) and the extent of LV dysfunction (based on LVEF and LV end-diastolic diameter). Hence we were able to obtain a better estimation 9 of the direct RV dysfunction effect. The use of propensity analysis with Cox regression stratified by quintiles of propensity scores showed that RV dysfunction, along with age and right atrial area, was a significant prognostic factor for MACE among patients with DCM, independent of the level of LV systolic and diastolic function. Stratification on quintiles of propensity score is a technique that is particularly validated when the effect of the therapy may reasonably vary according to the strength of the indication for its use or, in our case, when the effect of RV dysfunction on outcome is believed to vary according to the range of level of LV dysfunction. Another statistical method could have been used, which involves matching patients according to their age, LVEF and LV end-diastolic diameter, and according to factors influencing the level of RV dysfunction (LVOT TVI and E-wave DT), but this would have limited the data sample and hampered the statistical analysis. Study limitations This was a small, retrospective study; the patients included depict the population of a tertiary centre specializing in the diagnosis and therapeutic management of patients with HF. Notwithstanding this consideration, and the fact that most of our patients were in a stable haemodynamic state at inclusion, it may have resulted in an inclusion bias, and may not provide a clear representation of French patients with HF overall, but our inclusion criteria matched those of previously published studies in HF. A standardized echocardiography protocol for the evaluation of DCM was not available for all patients, and some RV function variables could not be included in the multivariable analysis because of missing data (S-wave, RV free wall strain and FAC), which will have lowered the power of the statistical analysis, despite their prognostic influence in other studies. Choice of and justification for TAPSE in the assessment of RV function has been addressed specifically in the Discussion section. Conclusion The simple measurement of TAPSE should probably be performed systematically in an echocardiographic examination, as it conveys important prognostic information in the case of idiopathic DCM. RV dysfunction, defined by TAPSE ≤ 15 mm, was mostly related to restrictive LV diastolic filling pattern (E-wave DT ≤ 145 ms). Through a propensity analysis, the presence of RV dysfunction provided incremental prognostic information, independent of the level of LV dysfunction. Disclosure of interest The authors declare that they have no competing interest. References [1] Elliott P, Andersson B, Arbustini E, et al. Classification of the cardiomyopathies: a position statement from the European Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS 10 [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] C. Venner et al. Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J 2008;29:270—6. Grzybowski J, Bilinska ZT, Ruzyllo W, et al. Determinants of prognosis in nonischemic dilated cardiomyopathy. J Card Fail 1996;2:77—85. Juilliere Y, Danchin N, Briancon S, et al. Dilated cardiomyopathy: long-term follow-up and predictors of survival. Int J Cardiol 1988;21:269—77. Rihal CS, Nishimura RA, Hatle LK, Bailey KR, Tajik AJ. Systolic and diastolic dysfunction in patients with clinical diagnosis of dilated cardiomyopathy. Relation to symptoms and prognosis. Circulation 1994;90:2772—9. Solomon SD, Anavekar N, Skali H, et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation 2005;112:3738—44. Mignot A, Donal E, Zaroui A, et al. Global longitudinal strain as a major predictor of cardiac events in patients with depressed left ventricular function: a multicenter study. J Am Soc Echocardiogr 2010;23:1019—24. Nahum J, Bensaid A, Dussault C, et al. Impact of longitudinal myocardial deformation on the prognosis of chronic heart failure patients. Circ Cardiovasc Imaging 2010;3:249—56. Champion HC, Michelakis ED, Hassoun PM. Comprehensive invasive and noninvasive approach to the right ventricle-pulmonary circulation unit: state of the art and clinical and research implications. Circulation 2009;120:992—1007. Voelkel NF, Quaife RA, Leinwand LA, et al. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation 2006;114: 1883—91. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation 2008;117:1717—31. Wahl A, Praz F, Schwerzmann M, et al. Assessment of right ventricular systolic function: comparison between cardiac magnetic resonance derived ejection fraction and pulsed-wave tissue Doppler imaging of the tricuspid annulus. Int J Cardiol 2011;151:58—62. Wang J, Prakasa K, Bomma C, et al. Comparison of novel echocardiographic parameters of right ventricular function with ejection fraction by cardiac magnetic resonance. J Am Soc Echocardiogr 2007;20:1058—64. Gulati A, Ismail TF, Jabbour A, et al. The prevalence and prognostic significance of right ventricular systolic dysfunction in nonischemic dilated cardiomyopathy. Circulation 2013;128:1623—33. La Vecchia L, Zanolla L, Varotto L, et al. Reduced right ventricular ejection fraction as a marker for idiopathic dilated cardiomyopathy compared with ischemic left ventricular dysfunction. Am Heart J 2001;142:181—9. Juilliere Y, Barbier G, Feldmann L, Grentzinger A, Danchin N, Cherrier F. Additional predictive value of both left and right ventricular ejection fractions on long-term survival in idiopathic dilated cardiomyopathy. Eur Heart J 1997;18: 276—80. Meluzin J, Spinarova L, Hude P, et al. Combined right ventricular systolic and diastolic dysfunction represents a strong determinant of poor prognosis in patients with symptomatic heart failure. Int J Cardiol 2005;105:164—73. Meyer P, Filippatos GS, Ahmed MI, et al. Effects of right ventricular ejection fraction on outcomes in chronic systolic heart failure. Circulation 2010;121:252—8. Sun JP, James KB, Yang XS, et al. Comparison of mortality rates and progression of left ventricular dysfunction in patients with idiopathic dilated cardiomyopathy and dilated versus nondilated right ventricular cavities. Am J Cardiol 1997;80:1583—7. [19] Glynn RJ, Schneeweiss S, Sturmer T. Indications for propensity scores and review of their use in pharmacoepidemiology. Basic Clin Pharmacol Toxicol 2006;98:253—9. [20] Heinze G, Juni P. An overview of the objectives and the approaches to propensity score analyses. Eur Heart J 2011;32:1704—8. [21] Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440—63. [22] Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr 2010;23:685—713 [quiz 86—8]. [23] Ghio S, Temporelli PL, Klersy C, et al. Prognostic relevance of a non-invasive evaluation of right ventricular function and pulmonary artery pressure in patients with chronic heart failure. Eur J Heart Fail 2013;15:408—14. [24] Meta-analysis Research Group in Echocardiography Heart Failure Collaborators, Doughty RN, Klein AL, et al. Independence of restrictive filling pattern and LV ejection fraction with mortality in heart failure: an individual patient meta-analysis. Eur J Heart Fail 2008;10:786—92. [25] McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012;14: 803—69. [26] Damy T, Kallvikbacka-Bennett A, Goode K, et al. Prevalence of, associations with, and prognostic value of tricuspid annular plane systolic excursion (TAPSE) among out-patients referred for the evaluation of heart failure. J Card Fail 2012;18: 216—25. [27] Ghio S, Recusani F, Klersy C, et al. Prognostic usefulness of the tricuspid annular plane systolic excursion in patients with congestive heart failure secondary to idiopathic or ischemic dilated cardiomyopathy. Am J Cardiol 2000;85: 837—42. [28] Pavlicek M, Wahl A, Rutz T, et al. Right ventricular systolic function assessment: rank of echocardiographic methods vs. cardiac magnetic resonance imaging. Eur J Echocardiogr 2011;12:871—80. [29] Focardi M, Cameli M, Carbone SF, et al. Traditional and innovative echocardiographic parameters for the analysis of right ventricular performance in comparison with cardiac magnetic resonance. Eur Heart J Cardiovasc Imaging 2015;16: 47—52. [30] Juilliere Y, Suty-Selton C, Riant E, et al. Prescription of cardiovascular drugs in the French ODIN cohort of heart failure patients according to age and type of chronic heart failure. Arch Cardiovasc Dis 2014;107:21—32. [31] Sallach JA, Tang WH, Borowski AG, et al. Right atrial volume index in chronic systolic heart failure and prognosis. JACC Cardiovasc Imaging 2009;2:527—34. [32] de Groote P, Millaire A, Foucher-Hossein C, et al. Right ventricular ejection fraction is an independent predictor of survival in patients with moderate heart failure. J Am Coll Cardiol 1998;32:948—54. [33] Gavazzi A, Berzuini C, Campana C, et al. Value of right ventricular ejection fraction in predicting short-term prognosis of Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006 +Model ACVD-880; No. of Pages 11 ARTICLE IN PRESS RV dysfunction in idiopathic dilated cardiomyopathy patients with severe chronic heart failure. J Heart Lung Transplant 1997;16:774—85. [34] Bursi F, McNallan SM, Redfield MM, et al. Pulmonary pressures and death in heart failure: a community study. J Am Coll Cardiol 2012;59:222—31. [35] Damy T, Viallet C, Lairez O, et al. Comparison of four right ventricular systolic echocardiographic parameters to predict adverse outcomes in chronic heart failure. Eur J Heart Fail 2009;11:818—24. [36] de Groote P, Fertin M, Goeminne C, et al. Right ventricular systolic function for risk stratification in patients with stable left ventricular systolic dysfunction: comparison of 11 radionuclide angiography to echoDoppler parameters. Eur Heart J 2012;33:2672—9. [37] Juilliere Y, Buffet P, Marie PY, Berder V, Danchin N, Cherrier F. Comparison of right ventricular systolic function in idiopathic dilated cardiomyopathy and healed anterior wall myocardial infarction associated with atherosclerotic coronary artery disease. Am J Cardiol 1994;73:588—90. [38] Kjaergaard J, Iversen KK, Akkan D, et al. Predictors of right ventricular function as measured by tricuspid annular plane systolic excursion in heart failure. Cardiovasc Ultrasound 2009;7:51. Please cite this article in press as: Venner C, et al. Right ventricular dysfunction in patients with idiopathic dilated cardiomyopathy: Prognostic value and predictive factors. Arch Cardiovasc Dis (2016), http://dx.doi.org/10.1016/j.acvd.2015.10.006