Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Adaptive immune system wikipedia , lookup
Globalization and disease wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Pathophysiology of multiple sclerosis wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
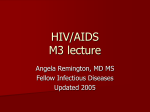
Clinical Infectious Diseases MAJOR ARTICLE HIV/AIDS Recent Thymus Emigrant CD4+ T Cells Predict HIV Disease Progression in Patients With Perinatally Acquired HIV Ramia Zakhour, Dat Q. Tran, Guenet Degaffe, Cynthia S. Bell, Elizabeth Donnachie, Weihe Zhang, Norma Pérez, Laura J. Benjamins, Gabriela Del Bianco, Gilhen Rodriguez, James R. Murphy, and Gloria P. Heresi Department of Pediatrics, University of Texas Health Center, Houston, Texas Background. Robust immune restoration in human immunodeficiency virus (HIV)–positive patients is dependent on thymic function. However, few studies have investigated thymic function and its correlation with disease progression over time in HIVpositive patients. Methods. In this longitudinal prospective study, we followed 69 HIV-positive patients who were perinatally infected. Peripheral blood mononuclear cells were stained with monoclonal anti-CD4 and anti-CD31 and recent thymic emigrants (CD4+recently emigrated from the thymus (RTE), CD4+CD31+) quantified by flow cytometry. Statistical analysis used Wilcoxon rank sum test, Kruskal–Wallis, Spearman correlation, and Kaplan–Meier estimates; Cox regression models were performed for the longitudinal analysis. Results. Median age of HIV positive patients enrolled was 13 years (interquartile range [IQR], 8.6). CD4+RTE% decreased with age and was higher in females. Median CD4+RTE% was 53.5%, IQR, 22.9. CD4+RTE% was closely related to CD4+% and absolute counts but independent of viral load and CD8+CD38+%. Antiretroviral compliance as well as higher nadir CD4+% were associated with higher CD4+RTE%. Low CD4+RTE% predicted poor progression of VL and CD4+% over time. Conclusions. CD4+RTE% predicts disease progression and may reflect history of disease in HIV-positive patients and adolescents. They are easy to measure in the clinical setting and may be helpful markers in guiding treatment decisions. Keywords. HIV; thymus; CD31; patients. Human immunodeficiency virus (HIV) infection can cause marked compromise of immune capacities that are, in part, consequences of diminished thymus production of T cells [1–4]. Central goals of clinical management of HIV patients include maintaining or restoring CD4+ T cells. The clinical success of this arm of management is most often evaluated as fraction of blood lymphocytes that are CD4+. However, this measurement does not discriminate whether the enumerated CD4+ cells are of peripheral or thymic origin; cells of thymic origin are required for more robust immunological capacities, providing a larger T-cell receptor repertoire [5]. To address this, studies have been conducted to directly measure T cells recently emigrated from the thymus (RTE). Results demonstrate that HIV infection can cause notable reductions in RTE and that in some circumstances therapy can restore RTE production. However, few studies have evaluated RTE in patients at sites of primary care delivery, especially in Received 16 October 2015; accepted 18 January 2016; published online 21 February 2016. Correspondence: G. P. Heresi, Department of Pediatrics, University of Texas, 6431 Fannin MSB 3.126, Houston, TX 77030 ([email protected]). Clinical Infectious Diseases® 2016;62(8):1029–35 © The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail [email protected]. DOI: 10.1093/cid/ciw030 patients who acquired HIV perinatally when their immune systems were immature. Although CD4 and viral load (VL) have long been shown to be good markers of disease control in HIV, multiple studies have proven the additive role of other markers as prognostic determinants for HIV disease progression, in particular, markers of immune activation [6]. However, there continues to be a need for easy-to-measure markers of disease progression [7], especially ones that can reflect successful therapeutic interventions. Determining the role of RTE in predicting clinical outcome in HIV-positive patients deserves further investigation. This could be especially important for patients who have seemingly well controlled disease while on and compliant with combined antiretroviral therapy (cART), but a fraction of whom will subsequently deteriorate. RTE measurements using T-cell receptor excision circles (TREC) have proven difficult to apply in clinical settings [3, 5]. Several studies have shown CD31 expression on CD4+ cells to decrease with maturation and correlate well with TREC content, making it an acceptable marker of CD4+RTE cells [8–10]. Because CD31 is expressed on the surface of CD4 cells and methodology to measure surface markers on CD4 cells, including CD4, are routine components of clinical management of HIV patients, it is possible that the addition of a single reagent to HIV/AIDS • CID 2016:62 (15 April) • 1029 a routine standard of care assay could provide quantitative information on CD4+RTE cells for pediatric patients in clinical settings [5]. We hypothesized that CD4+RTE% measured by flow cytometry will predict the subsequent clinical course with respect to HIV disease for perinatally HIV-infected patients. To this purpose, we prospectively measured CD4+RTE% in a population of perinatally infected patients and adolescents attending a pediatric HIV specialty clinic. METHODS Patients The study involved 69 HIV-positive patients, perinatally infected, receiving care through the Pediatric HIV Clinic of UTHealth, Houston, Texas. During the study period, the clinic provided services to 96 HIV-positive patients and adolescents (all were offered participation in the study; 1 declined), of whom 84 attended the clinical laboratory that collaborated in providing samples for this study (blood samples either could not be obtained or were of poor quality for 15 of the patients who attended the collaborating clinical laboratory). The Institutional Review Board of UTHealth approved the study. Blood samples were collected at each routinely scheduled clinic visit between January 2010 and September 2012. Clinical and laboratory data were retrieved from medical records. Lymphocyte Phenotyping Peripheral blood mononuclear cells were isolated from EDTA anticoagulated fresh whole blood using a commercial lymphocyte separation media (MP Biomedical, LLC). A total of 50 000 cells were surface stained for 20 minutes at 4°C in the dark with PerCP-Cy5.5–conjugated anti-CD4 (Clone RPA-T4, BioLegend, San Diego, California) and fluorescein isothiocyanate– conjugated anti-CD31 (Clone MBC 78.2 [R-PECAM1.2], Invitrogen, Carlsbad, California), then washed and resuspended in phosphate-buffered solution. A FACSCalibur (BD Biosciences) was used for data acquisition. Analysis was performed using FlowJo software, version 7.6 (Tree Star, Inc.). Supplementary Figure 1 presents the gating strategy. Analyses Patients were classified into groups representing their clinical status with respect to HIV disease at baseline ( point of enrollment and collection of first blood sample). Patients classified into clinically good status (Cgood) had CD4 ≥25% and undetectable HIV RNA in plasma (<50 HIV RNA copies/mL). Patients in clinically poor status (Cpoor) had CD4 <25% and ≥50 HIV RNA copies/mL. Patients in clinically intermediate status (Cint) had CD4 ≥ 25% and ≥50 HIV RNA copies/mL. One patient had CD4 <25% and <50 HIV RNA copies/mL. This individual was excluded from group analysis. Patients were considered to be on treatment if they were receiving cART defined as dual-nucleoside–nucleotide reverse 1030 • CID 2016:62 (15 April) • HIV/AIDS transcriptase inhibitors with either a nonnucleoside reverse transcriptase inhibitor or a protease inhibitor without interruption for at least 3 months prior to baseline CD4+RTE measurement. Duration of overall antiretroviral exposure was expressed as cumulative duration in days of receipt of any 1 or more antiretroviral drugs. Patients were considered ART naive if they had not received any cART in the past. All others were considered as having interrupted treatment. The data were initially analyzed cross-sectionally using historical findings and clinical measures made on baseline blood samples. Spearman ρ was used to calculate correlations, and Mann–Whitney U, Kruskal–Wallis, and Wilcoxon signed ranks tests were used for comparisons. A linear regression model was used to determine independent predictors of CD4+RTE%. Likelihood ratio tests were used to compare models and determine best fit in a backward stepwise method. To further investigate the capacity of CD4+RTE% to predict clinical course, Kaplan–Meier estimates, univariate log-rank tests, and multivariate Cox proportional hazards regression models were calculated for 2 outcomes: deterioration of clinical status and improvement of clinical status. A deteriorating clinical event was defined among baseline Cgood and Cint patients as any follow-up visit with CD4 <25% and ≥50 HIV RNA copies/mL (Cpoor). An improving clinical event was defined among baseline Cpoor and Cint patients as any follow-up visit with CD4 ≥25% and <50 HIV RNA copies/mL (Cgood). Assumptions of proportional hazards and time-varying covariate effects were graphically assessed. A P value <.05 was considered as statistically significant. RESULTS Demographic, clinical, and laboratory data from baseline are presented in Table 1. As expected, CD4+RTE% correlated negatively with age (ρ = −0.48 [P < .001]). Values of CD4+RTE% were somewhat higher in females compared with males; the difference approached statistical significance (medians 57.8 [interquartile range = 21.0] and 47.8 [interquartile range = 25.4], respectively, P = .055). Associations of Baseline CD4+RTE% With Patient History and Selected Baseline Laboratory Outcomes We used correlation analysis to test for univariate relationships between CD4 + RTE% at baseline, other outcomes measured on the same blood sample, and outcomes selected as indicators of each patient’s HIV disease history. CD4+RTE% Correlates Positively With CD4 and Is Independent of Viral Load The findings demonstrated strongly significant positive correlations between CD4+RTE% and other contemporary measures of CD4+ cells, including CD4+% (r = 0.44; P < .001) and CD4:CD8 ratio (r = 0.37; P = .002). Baseline CD4+RTE% showed equally strong positive correlations with nadir CD4 count (r = 0.41; P < .001); this is a value that, in most instances, occurred many Table 1. Demographic Clinical and Laboratory Data at Baseline HIV Clinical Status Group Outcome N All HIV Positive 69 Cpoor 9 Cint P1 a Cgood 34 P2a P3 a 25 14.1 [11.1] .002 .012 .668 18 (52.9) 12 (48) .461 .336 .708 26 (76.5) 14 (56) .688 .187 .127 13.2b [9.7] .011 Age (y) 13 [8.6] 17.7 [5.3] Female 37 (53.6) 6 (66.7) Black 49 (71) 8 (88.9) 11.7 [7.6] CD4 33 [5.48] 38.6 [15.1] <.001 <.001 CD4+Abs cell/µL 792 [718] 228 [267] 803 [680] 897 [574] <.001 <.001 .382 CD4+RTE% 53.5 [22.9] 46.1 [21.8] 54.4 [19.3] 57.8 [27.6] .066 .188 .933 378.1 [489.6] 100.8 [118.7] 447.9 [453] 394.4 [610.9] <.001 <.001 .771 18 [12] 10 [5] 20 [7] 20 [20] <.001 .011 .920 CD4+% CD4+RTEAbs cell/µL CD4+%Nadir 33 [12] CD4+AbsNadir cell/µL 308 [493.5] 92 [140] 411 [331.25] 333 [599] <.001 .014 .471 CD4/CD8 ratio 0.8 [0.6] 0.2 [0.2] 0.7 [0.5] 1.2 [1.2] <.001 <.001 .003 CD8 CD8+% 40.9 [21.7] 61 [26.7] 43 [19.6] 32.4 [15.3] .002 <.001 .003 CD8+Abs cell/µL 931 [637] 1200 [832] 1042 [686.5] 806 [461] .758 .102 .032 CD8+CD38+% 21 [20] 38 [28] 23.5 [18.3] 15 [17.5] .057 .001 .002 CD8+HLA-DR+% 10 [11.5] 26 [13] 11.5 [10.8] 6 [5.5] .002 <.001 .015 HIV VL Log10VL 2.2 [1.5] 4.5 [2.6] 2.8 [1.1] Undetectable .061 <.001 <.001 Average Daily VLc 3.4 [1.0] 3.8 [0.7] 3.4 [1.1] 2.87 [1.3] .060 .010 .063 0.8 [1.9] 1.9 [5.2] 0.61 [2.0] 0.44 [1.0] .125 .020 .840 .445 .046 .040 Treatment Age at initiation (y) cART Yes 56 (81.2) 7 (77.8) 24 (70.6) 24 (96) No, ART Interrupted 7 (10.1) 2 (22.2) 5 (14.7) 0 (0) No, ART naive 6 (8.7) 0 (0) 5 (14.7) 1 (4) Values are medians (interquartile ranges) or counts (%). Abbreviations: Abs, absolute; ART, antiretroviral therapy; cART, combined antiretroviral therapy; Cgood, clinically good status; Cint, clinically intermediate status; Cpoor, clinically poor status; HIV, human immunodeficiency virus; RTE, recently emigrated from the thymus; VL, viral load. a P1, P value for comparisons between groups Cpoor and Cint; P2, Cpoor and Cgood; P3, Cint and Cgood. Significant P values are in bold. b Values in italics are outside of clinical laboratory normal ranges. c To estimate cumulative plasma HIV RNA, a geometric mean daily VL is calculated. The log10 of each reported VL (from each patient’s first VL test until the baseline test) is determined, and the trapezoidal rule is used to estimate daily VL between measurements [11]. The sum of these daily log values is divided by the cumulative number of days between first and most recent VL measurement. years before the reference CD4+RTE% measurement. Associations of CD4+RTE% with contemporary measurements of CD8+ cells were not as strong but reached significance for a negative relationship with CD8+% (r = −0.25; P = .040) and the subset CD8+HLA-DR+% (r = −0.24; P = .046). In contrast with CD8+HLA-DR+%, a second marker of immune system activation, CD8+CD38+%, showed no relationship with CD4+RTE% (r = 0.003; P = .982). Analysis did not reveal any significant correlations between CD4+RTE% and contemporary HIV viremia (r = −0.07; P = .560), cumulative historical VL (r = 0.01; P = .900), or peak historical VL (r = −0.07; P = .594). on average, ART-naive patients had lower CD4+RTE% when compared with patients with interrupted treatment and patients on cART. The differences between ART-naive and cART groups approached statistical significance (P = .064) in spite of the small number of patients in the ART-naive group (Table 2). Table 2. CD4+RTE% and Age by Treatment Group ART History Outcome N CD4+RTE% in HIV Perinatally Infected Children Is Predicted by Treatment Status and, to a Lesser Extent, to Nadir CD4+% Fifty-six (81%) patients were on cART and 13 were not on cART at baseline. Of the 13 not on cART, 6 had never received treatment (ART naive, slow progressors) and 7 had been on cART but had compliance issues (interrupted treatment). Despite being younger Naive 6 Interrupted 7 cART P1 a P2 a P3 a 56 NA NA NA CD4+RTE% 37.6 [11.6] 47.8 [25.8] 54.9 [22.1] .366 .064 .338 Age 11.6 [10.6] 15.4 [6.7] 13.0 [9.0] .534 .719 .327 Values are medians and interquartile ranges. Abbreviations: ART, antiretroviral therapy; cART, combined antiretroviral therapy; NA, not applicable; RTE, recently emigrated from the thymus. a P1 lists P values for comparisons between ART naive and ART interrupted; P2 is for ART naive and cART; and P3 is for ART interrupted and cART. HIV/AIDS • CID 2016:62 (15 April) • 1031 To further resolve the relationship with treatment status, a multivariate linear regression model with CD4+RTE% as a dependent variable was constructed. After controlling for associations between CD4+RTE% by age and gender, the model confirmed the significant reduction in CD4+RTE% among treatment-naive patients and a minor reduction among patients with interrupted treatment compared with those on cART (Table 3). Though only approaching significance, CD4+RTE% remained positively associated with nadir CD4+% as the next most influential variable in predicting CD4+RTE%. Ethnicity, HIV clinical status group, CD8+%, CD8+CD38+%, CD8+HLADR+%, and CD4:CD8 ratio did not show a significant association with CD4+RTE% after adjusting for age, gender, treatment status, and nadir CD4+%. Longitudinal Studies of CD4+RTE Cells CD4+RTE% at Baseline Predicts Change Over Time in HIV Disease Clinical Status Group To identify values of CD4+RTE% that associate with improving or deteriorating HIV disease clinical status, the 33 patients with HIV clinical status Cpoor or Cgood and with at least 1 additional blood sample after baseline were evaluated for clinical change over the duration of observation. Three (38%) of the 8 patients initially classified as Cpoor at baseline improved to Cint or Cgood clinical status at least once during their follow-up. The patients who showed improvement had a median baseline CD4+ RTE% of 49.5%, which is 14.4% higher than for those who remained in the Cpoor classification. Reciprocally, of the 25 patients classified at baseline as Cgood, 11 (44%) showed deteriorating clinical status, with at least 1 subsequent blood sample indicating less than Cgood classification. The patients who showed clinical deterioration had a median CD4+RTE% Table 3. Summary of Linear Regression Analysis Predicting CD4+RTE% SE β P Value Variable B Female 9.057 2.970 0.312 .003 Age (y) −1.057 0.326 −0.405 .002 Treatment group Interrupted Naive Nadir CD4+% Constant −4.366 4.695 −0.091 .356 −12.300 5.354 −0.241 .025 0.309 0.174 0.221 55.490 6.367 NA .080 <.001 Initial independent variables included were age, gender, ethnicity, human immunodeficiency virus clinical status group, CD8+%, CD8+CD38+%, CD8+HLA-DR+%, CD4:CD8 ratio, treatment status, and nadir CD4+%. Variables that were found to be nonsignificant were removed from the model in a stepwise fashion and log likelihood ratios were calculated to compare models before and after removal of each variable to ensure that no significant change to the model was occurring (P value <.05 for likelihood ratio test). We retained all variables with a P value <.1 in the model. Statistically significant (P < .05) associations with CD4+RTE% are bolded. Treatment groups were coded as categorical variables with baseline category being combined antiretroviral therapy. Baseline category for gender was male. Nadir CD4+% and age were used as continuous variables. Abbreviations: β, standardized regression coefficients; B, unstandardized regression coefficient; NA, not applicable; RTE, recently emigrated from the thymus; SE, standard errors of unstandardized coefficients. 1032 • CID 2016:62 (15 April) • HIV/AIDS of 45.8% at baseline, which is 18.1% lower than for those who remained in Cgood classification. These findings suggest that patients with CD4+RTE% greater or equal to approximately 50% in a blood sample are more likely to show subsequent clinical improvement, while those with less than approximately 50% CD4+RTE% are more likely to clinically deteriorate. CD4+RTE <50% Independently Predicts Deterioration of HIV Clinical Status Baseline clinical variables predictive of longitudinal disease outcomes were identified using multivariate Cox regression models comprising 59 baseline Cgood and Cint patients (to evaluate for deterioration) and 42 baseline Cpoor and Cint patients (to evaluate for improvement). Low CD4+RTE% <50% and high CD8+ HLA-DR+ >10% significantly predicted deteriorating clinical course in Cgood and Cint patients at baseline (Figure 1A and 1B). Alternatively, treatment status completely predicted improving clinical course (Figure 1C) such that, of 17 (40%) baseline Cpoor and Cint patients who improved to Cgood status during follow-up, all were actively receiving cART. Within these Cpoor and Cint patients receiving cART at baseline, CD8+ HLA-DR+ <10% significantly predicted improvement of clinical status (Figure 1D). High CD4+RTE% (≥50%) and low CD8+% (<36%) at baseline showed univariate association to improvement in clinical status during follow-up but did not remain significant in the multivariate model. DISCUSSION In this study, CD4+RTE% measured as CD31 expressed on CD4+ T cells predicted HIV disease progression (mainly deterioration) in perinatally HIV-infected patients and adolescents. CD4+RTE% in our population decreased with age and was somewhat higher in females, as previously described [12, 13]. We did not find correlations between CD4+RTE% and VL or between CD4+RTE% and average daily VL, which reflects overall exposure to virus. Similar to our findings, De Rossi et al showed that increases in RTE measured as TREC do not correlate with changes in VL and that there are no differences over time in TRECs between patients with or without virologic response to cART [14]. Nikolic-Djokic et al showed that TREC levels correlate with immunologic response but not with virologic response to treatment [15]. These findings may be due to the dissociation between virologic and immune responses frequently described in patients and/or to the fact that resistant viruses are less virulent and less likely to cause immune suppression despite persistent viremia [16]. Thymocytes have been described to be resistant to entry of protease inhibitor–resistant HIV virus [17]. It has also been previously described that TREC do not correlate with VL in patients on treatment for a prolonged period of time [18]. This might explain the finding in our population since most had been on cART for years at study entry. Klein et al found no preferential loss of CD31+ cells among naive CD4 cells after planned treatment interruptions that Figure 1. A and B, Significant predictors of deterioration: patients transitioning from better than clinically poor status (Cpoor) at baseline to Cpoor during follow-up. (C and D), Significant predictors of improvement: patients transitioning from less than clinically good status (Cgood) at baseline to Cgood during follow-up. Abbreviations: ART, antiretroviral therapy; cART, combined antiretroviral therapy; RTE, recently emigrated from the thymus. resulted in a decrease in CD4 counts in HIV-positive patients, concluding that immune activation must contribute to this decrease in addition to possibly decreased thymic function [19]. In our study, thymic function measured as CD4+RTE% was independent of immune activation measured as CD8+CD38+% but not as measured by CD8+HLA-DR+%. CD38 measured on CD8+ cells has been suggested to independently predict response to therapy and disease progression in patients and adults [20–22]. Interestingly, CD4+RTE% did not follow the same pattern of change as CD8+CD38+% when the clinical groups changed over time and did not correlate with CD8+CD38+% overall in our study. Discrepancy between CD38 expression and HLA-DR expression on CD8+ T cells has been described, with the existence of CD8+CD38−HLA-DR+, CD8+CD38+ HLA-DR−, and CD8+CD38+HLA-DR+ cells [23]. CD38 and HLA-DR seem to be expressed on CD8+ T cells at different but partially overlapping stages of their development and maturation [24]. CD38 is expressed on both immature naive CD8 cells as well as activated memory cells [25], whereas HLA-DR is solely expressed on stimulated and activated CD8+ T cells [26]. HLA-DR expression has been shown to correlate negatively with TREC content of CD8+ T cells [26]. This could explain the negative correlation that we found between CD8+HLA- DR+% and CD4+RTE%. CD8+HLA-DR+% was recently described to be significantly higher than CD8+CD38+% in HIV controller patients and to have higher expression on mildly stimulated CD8+ T cells, whereas there was more coexpression of HLA-DR and CD38 on highly activated CD8+ T cells (higher antigen exposure) [23]. These findings combined with ours suggest that HLA-DR has some particularity/superiority over CD38 in predicting disease progression, which might be related to HIV disease pathogenesis and its influence on the generation of cells expressing 1 or both of these markers. In this study, CD8+HLA-DR+% and CD4+RTE% both predicted deterioration of HIV disease as determined by change in CD4 and VL. However, CD4+RTE% was the single most potent prognostic marker to predict such deterioration (P = .0004). CD4+RTE% in HIV-positive patients in our study was mainly dependent on treatment status and nadir CD4+%. This highlights the importance of treatment in thymic function maintenance and recovery as even patients not on treatment at time of study entry but with a history of treatment had higher CD4+RTE% than ART-naive patients despite preserving relatively good CD4 counts and VL. This may be an additional reason to support the start of therapy in patients in whom no other obvious indication for treatment is present. Another finding that supports HIV/AIDS • CID 2016:62 (15 April) • 1033 early initiation of treatment is that patients in the Cgood group were significantly younger at initiation of cART compared with those in the Cpoor group. Similar to Blanche et al, we found nadir CD4+% to correlate with CD4+RTE% and to have a close to significant role in predicting its value [27]. The importance of nadir CD4+% and treatment history in predicting CD4+RTE% highlights that RTE reflect disease history. The remainder of our results, particularly what pertains to differences in RTE between viremic and aviremic patients and changes with age, do not concur with findings by Blanche et al [27]. This discordance is partially due to differences in the populations. However, an important difference is that our study and most previously published literature expressed RTE as a subpopulation of CD4+ cells, whereas Blanche et al expressed RTE as a percentage of naive CD4 cells, making their data difficult to compare with ours and those of others [28, 29]. We found CD4+RTE% to predict the evolution of virologic and immunologic status of patients. This is based, in part, on the results of the survival analysis but also shown by trends of CD4+RTE% when broken down by clinical groups and stability of those groups over time. Small group size may have accounted for the nonstatistical significance of some of these observations. In a study of adults, RTEs were deemed unsuitable as a marker of CD4 recovery [30]. On the other hand, Li et al recently showed CD31 expressed on naive CD4 cells at initiation of treatment to predict rate of CD4 recovery in HIV-positive adults [28]. Our finding that CD4+RTE% at any point in time can predict deterioration in clinical grouping in HIV-positive patients is new. The dynamics and lack of homogeneity in our population may have limited the significance of some of our observations. Our results were not always significant due to small sample size in some of our groups. CONCLUSION In our study, CD4+RTE% reflected HIV history including cART exposure history and nadir CD4+%. Baseline CD4+ RTE% independently predicted CD4 and VL failure. This easily measurable subset of CD4+ T cells may thus guide the clinician in treatment related decision making, including introduction of an adjuvant therapy to increase thymic output and in determining patient prognosis. The information provided by CD4+RTE% measurements seems to be independent/incremental to that provided by other routinely measured laboratory values. Supplementary Data Supplementary materials are available at http://cid.oxfordjournals.org. Consisting of data provided by the author to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the author, so questions or comments should be addressed to the author. Notes Acknowledgments. We thank our patients, without whom this work would not have been possible. We also thank the clinical and laboratory staff who made the blood collection possible. 1034 • CID 2016:62 (15 April) • HIV/AIDS Financial support. This work was supported by the Texas HIV Initiative. Potential conflicts of interest. All authors: No reported conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. References 1. Stebbing J, Gazzard B, Douek DC. Where does HIV live? N Engl J Med 2004; 350:1872–80. 2. Fernandez S, Nolan RC, Price P, et al. Thymic function in severely immunodeficient HIV type 1-infected patients receiving stable and effective antiretroviral therapy. AIDS Res Hum Retroviruses 2006; 22:163–70. 3. Sandgaard KS, Lewis J, Adams S, Klein N, Callard R. Antiretroviral therapy increases thymic output in children with HIV. AIDS 2014; 28:209–14. 4. Cotugno N, Douagi I, Rossi P, Palma P. Suboptimal immune reconstitution in vertically HIV infected children: a view on how HIV replication and timing of HAART initiation can impact on T and B-cell compartment. Clin Dev Immunol 2012; doi:10.1155/2012/805151. 5. Kohler S, Thiel A. Life after the thymus: CD31+ and CD31- human naive CD4+ T-cell subsets. Blood 2009; 113:769–74. 6. Hazenberg MD, Otto SA, van Benthem BH, et al. Persistent immune activation in HIV-1 infection is associated with progression to AIDS. AIDS 2003; 17:1881–8. 7. Langford SE, Ananworanich J, Cooper DA. Predictors of disease progression in HIV infection: a review. AIDS Res Ther 2007; 4:11. 8. Junge S, Kloeckener-Gruissem B, Zufferey R, et al. Correlation between recent thymic emigrants and CD31+ (PECAM-1) CD4+ T cells in normal individuals during aging and in lymphopenic children. Eur J Immunol 2007; 37:3270–80. 9. Demeure CE, Byun DG, Yang LP, Vezzio N, Delespesse G. CD31 (PECAM-1) is a differentiation antigen lost during human CD4 T-cell maturation into Th1 or Th2 effector cells. Immunology 1996; 88:110–5. 10. Tanaskovic S, Fernandez S, Price P, Lee S, French MA. CD31 (PECAM-1) is a marker of recent thymic emigrants among CD4+ T-cells, but not CD8+ T-cells or gammadelta T-cells, in HIV patients responding to ART. Immunol Cell Biol 2010; 88:321–7. 11. Cole SR, Napravnik S, Mugavero MJ, Lau B, Eron JJ Jr, Saag MS. Copy-years viremia as a measure of cumulative human immunodeficiency virus viral burden. Am J Epidemiol 2010; 171:198–205. 12. Pido-Lopez J, Imami N, Aspinall R. Both age and gender affect thymic output: more recent thymic migrants in females than males as they age. Clin Exp Immunol 2001; 125:409–13. 13. Kilpatrick RD, Rickabaugh T, Hultin LE, et al. Homeostasis of the naive CD4+ T cell compartment during aging. J Immunol 2008; 180:1499–507. 14. De Rossi A, Walker AS, Klein N, De Forni D, King D, Gibb DM. Increased thymic output after initiation of antiretroviral therapy in human immunodeficiency virus type 1-infected children in the Paediatric European Network for Treatment of AIDS (PENTA) 5 Trial. J Infect Dis 2002; 186:312–20. 15. Nikolic-Djokic D, Essajee S, Rigaud M, et al. Immunoreconstitution in children receiving highly active antiretroviral therapy depends on the CD4 cell percentage at baseline. J Infect Dis 2002; 185:290–8. 16. Ometto L, De Forni D, Patiri F, et al. Immune reconstitution in HIV-1-infected children on antiretroviral therapy: role of thymic output and viral fitness. AIDS 2002; 16:839–49. 17. Haynes BF, Sempowski GD. Can the thymus win the battle against drug-resistant HIV? Nat Med 2001; 7:661–2. 18. Saitoh A, Singh KK, Sandall S, et al. Association of CD4+ T-lymphocyte counts and new thymic emigrants in HIV-infected children during successful highly active antiretroviral therapy. J Allergy Clin Immunol 2006; 117:909–15. 19. Klein N, Sefe D, Mosconi I, et al. The immunological and virological consequences of planned treatment interruptions in children with HIV infection. PLoS One 2013; 8:e76582. 20. Rosso R, Fenoglio D, Terranova MP, et al. Relevance of CD38 expression on CD8T cells to evaluate antiretroviral therapy response in HIV-1-infected youths. Scand J Immunol 2010; 71:45–51. 21. Ruel T, Ssewanyana I, Achan J, et al. Dynamics of T cell activation accompanying CD4 recovery in antiretroviral treated HIV-infected Ugandan children. Clin Immunol 2009; 131:410–4. 22. Karim R, Mack WJ, Stiller T, et al. Association of HIV clinical disease progression with profiles of early immune activation: results from a cluster analysis approach. AIDS 2013; 27:1473–81. 23. Hua S, Lecuroux C, Saez-Cirion A, et al. Potential role for HIV-specific CD38-/ HLA-DR+ CD8+ T cells in viral suppression and cytotoxicity in HIV controllers. PLoS One 2014; 9:e101920. 24. Ramzaoui S, Jouen-Beades F, Gilbert D, et al. During HIV infection, CD4+ CD38+ T-cells are the predominant circulating CD4+ subset whose HLA-DR positivity increases with disease progression and whose V beta repertoire is similar to that of CD4+ CD38- T-cells. Clin Immunol Immunopathol 1995; 77:33–41. 25. Benito JM, Lopez M, Lozano S, et al. Differential upregulation of CD38 on different T-cell subsets may influence the ability to reconstitute CD4+ T cells under successful highly active antiretroviral therapy. J Acquir Immune Defic Syndr 2005; 38:373–81. 26. Imamichi H, Lempicki RA, Adelsberger JW, et al. The CD8+ HLA-DR+ T cells expanded in HIV-1 infection are qualitatively identical to those from healthy controls. Eur J Immunol 2012; 42:2608–20. 27. Blanche S, Scott-Algara D, Le Chenadec J, et al. Naive T lymphocytes and recent thymic emigrants are associated with HIV-1 disease history in French adolescents and young adults infected in the perinatal period: the ANRS-EP38-IMMIP study. Clin Infect Dis 2014; 58:573–87. 28. Li T, Wu N, Dai Y, et al. Reduced thymic output is a major mechanism of immune reconstitution failure in HIV-infected patients after long-term antiretroviral therapy. Clin Infect Dis 2011; 53:944–51. 29. Lewis J, Walker AS, Klein N, Callard R. CD31+ cell percentage correlation with speed of CD4+ T-cell count recovery in HIV-infected adults is reversed in children: higher thymic output may be responsible. Clin Infect Dis 2012; 55:304–7; author reply 7. 30. Bofill M, Martinez-Picado J, Ruiz-Hernandez R, et al. Naive CD4(+) T cells and recent thymic emigrant levels in treated individuals with HIV: clinical relevance. AIDS Res Hum Retroviruses 2006; 22:893–6. HIV/AIDS • CID 2016:62 (15 April) • 1035