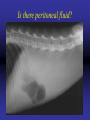
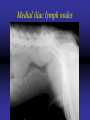
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
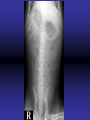
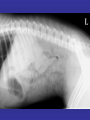
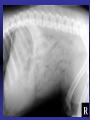
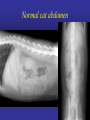
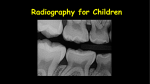
General Abdominal Radiography Tony Pease, DVM, MS Assistant Professor of Radiology North Carolina State University Objectives • • • • • Acquisition of radiographs Abdominal radiographic anatomy Radiographic patterns of abdominal disease Determine normal compared to abnormal How ultrasound is helpful Reading • Chapters 38-40 – Pages 483-539 Abdominal Radiography • Generally being replaced with ultrasound – Ultrasound does not give a global picture • Radiographs are a snapshot of disease – 1/120th of a second picture • Ultrasound is real time Abdominal Anatomy • A lot of organs in a small space • Rely on location Acquiring radiographs • Relatively high kVp (70 kVp) – Moderate image contrast – Some of shades of grey – More than bone less than thorax • Moderate mAs (8-12 mAs) – Minimizes motion artifact – Maximizes contrast • Enemas and fasting are helpful Positioning • Include caudal thorax • Try to include greater trochanter of femur • Center beam just caudal to the last rib Large patients • May need two films per view – Four films per study – Make sure to overlap images Ventrodorsal • • • • • Liver Spleen Left Kidney Right Kidney Stomach and duodenum Left lateral • • • • • • • • Esophagus Pylorus Duodenum Liver Spleen Left kidney Right kidney Urinary bladder Right lateral • • • • • • Fundus Liver Spleen Left kidney Right kidney Urinary bladder Normal cat abdomen Deep circumflex iliac artery Sometimes confused for medial iliac lymph nodes or ureteral calculi Positional radiographs • Remember gas rises • Can manipulate the animal Can you see the gas? Lateral horizontal beam Horizontal beam • Place the animal in left lateral – Puts the fundus of the stomach down – Smaller pylorus is high • Gas accumulates near the diaphragm Now time for the radiographs! • Positioning – done • Exposure – done • Interpretation! – Takes radiologists years to become experts – You have 9 hours! Quick word on abdominal masses • Hard to tell what organ is involved • Best guess based on location – What organs are displaced • May need ultrasound to be more specific Some incidental findings • Lucency on the ventral aspect of L3-4 • Cholesterol granulomas • Spondylosis deformans Lack of ventral aspect of L4 • It is where the diaphragm attaches Cholesterol granuloma • Generally in cats Smooth bridging bone Spaces of the abdomen • Retroperitoneal – Dorsal to the colon – Contains kidneys, adrenal glands, lymph nodes – Continuous with mediastinum • Peritoneal – Surrounds visceral organs – Generally a potential space Can compare spaces Retroperitoneal space Good detail Peritoneal space Poor detail Loss of serosal detail • • • • • • Poor radiographic technique Fat content of a puppy or kitten Peritoneal fluid (many types) Carcinomatosis Lack of fat Peritonitis Peritoneal fluid • Soft tissue and fluid are similar opacity • Ultrasound superior for peritoneal fluid • Emaciation versus fluid – Similar appearance – Lack of fat to provide contrast – Difference is overall size of abdomen Peritoneal fluid • Radiographs very insensitive for detecting • Cannot tell fluid type – Radiographs or ultrasound! • Multiple causes – Increased hydrostatic pressure – Decreased plasma colloid oncotic pressure – Capillary permeability Mild Severe Severe Lack of fat cause loss of detail Is there peritoneal fluid? Retroperitoneal space • Only thing that is dorsal to the colon Don’t forget that other view Abdominal lymph nodes • Many lymph nodes in abdomen • Generally not seen radiographically – Even if large • Medial iliac lymph nodes are the exception • Ultrasound more useful for lymph nodes Medial iliac lymph nodes Don’t forget about goats • Can help diagnose caseous lymphadenitis Pneumoretroperitoneum • Retroperitoneum communicates with the mediastinum • Therefore usually associated with: – Subcutaneous emphysema – Pneumomediastinum Need large volume of gas • Ruptured trachea • Ruptured esophagus – Need aerophagia Pneumoretroperitoneum • Not generally clinically important • Just a sign of another disease Even in the cow! Pneumoperitoneum • Can persist 10-14 days after surgery • Rupture of a hollow viscus – Gastrointestinal perforation – Surgical emergency!! • External puncture wound Several places to look What about large animal? Foals, calves and pigs • Can image abdomen – Usually standing – See fluid layers • Can do barium enemas – Strictures or atresia ani Barium enema Ileus Traumatic reticuloperitonitis Traumatic reticuloperitonitis All about the belly in 1 hour! • Radiographs helpful even if large animal • Hard to tell where mass comes from • Radiographs are a good overview Questions?