Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
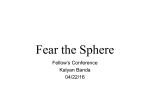
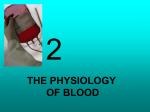
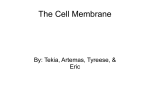
Ned Tijdschr Klin Chem Labgeneesk 2016; 41: 217-228 Proefschriften Erythrocyte aging and disease A tale of membranes and microparticles S. DINKLA This chapter is an introduction to the research on erythrocytes, microparticles and regulatory T cells that is presented in the subsequent chapters. The first part of this chapter briefly discusses the main functions and characteristics of the erythrocyte. The second part focusses on erythrocyte aging and removal, transfusion side effects, and anemia of inflammation. The third part discusses the functions of erythrocyte-derived and platelet-derived microparticles in the context of health, disease and transfusion medicine. In the fourth part, a brief overview of the immune system and its role in tissue homeostasis is given. In the final part, the scope of this thesis is presented. I - The erythrocyte Erythrocytes, commonly known as red blood cells, are the most abundant cells in the circulation, and are the principal means of oxygen delivery to and CO2 removal from the peripheral tissues. The erythrocyte owes its ability to transport oxygen to its high hemoglobin content. In the human lung, the erythrocytes take up oxygen at the alveolar-capillary interface, which they release whilst traversing the capillary network in the peripheral tissues. This oxygen release is stimulated by the CO2 that is produced by metabolically active tissues. Upon entering the erythrocyte, CO2 is converted into HCO3- and H+ by the enzyme carbonic anhydrase. The subsequent decrease in intracellular pH serves as a signal for hemoglobin to release oxygen. Erythrocytes are biconcave disks with an approximate diameter of 7 µm and maximum thickness of 2.5 µm. Unlike almost all the other cells of the body, erythrocytes do not contain intracellular organelles such as a nucleus, endoplasmic reticulum, Golgi apparatus, and mitochondria, which enables a maximal hemoglobin content and plasma membrane deformability. Erythrocytes must be able to undergo large passive deformations in order to pass through the narrow Proefschrift ter verkrijging van de graad van doctor aan de Radboud Universiteit Nijmegen Promotoren: Prof. dr. I. Joosten Prof. dr. R. Brock Copromotoren:Dr. G.J.C.G.M. Bosman Dr. V.M.J. Novotný E-mail: [email protected] Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 capillaries of the microvasculature and the fenestrae in the spleen. The shear stress that erythrocytes experience when traversing the vessels and the deoxygenation of their hemoglobin trigger the release of potent vasodilators in the form of S-nitrosothiol and ATP, which promote the passage of the erythrocyte. ATP promotes the release of NO by the vascular endothelium, which is further enhanced by the shear stress that the passing erythrocytes exert on the endothelium. This physiological activity is exemplary for the complex interactions between the erythrocyte and its environment. II - Erythrocyte aging and removal In the red bone marrow, multipotent hematopoietic stem cells proliferate and differentiate to form erythroblasts (1), which produce large quantities of hemoglobin and ultimately expel their nuclei to form reticulocytes. The reticulocytes mature into erythrocytes in the bone marrow, a process which is completed after their release into the circulation. This maturation process is characterized by loss of intracellular 217 Figure 1. Erythrocyte birth, aging and removal. organelles such as mitochondria and ribosomes (2, 3), and by extensive membrane remodeling (4, 5). In the circulation, the average lifespan of the human erythrocyte is approximately 120 days (6), which means that 200 billion erythrocytes have to be removed and replaced every day. Physiological autoantigens During their stay in the circulation, erythrocyte aging results in an increase in autologous IgG binding, which ultimately leads to the phagocytosis of old erythrocytes by Kupffer cells in the liver (Figure 1) (7). The work of Marguerite Kay has uncovered that the binding of physiological autoantibodies to senescent erythrocytes is associated with changes in band 3. These changes are thought to be triggered by the binding of denatured hemoglobin to the cytoplasmic domain of band 3 (Figure 1) (7). It has been suggested that selective tyrosine phosphorylation of oxidized band 3 by Syk may play a role in the recruitment of hemoglobin-bound band 3 molecules in large membrane aggregates that show a high affinity to physiological autoantibodies (8). Band 3 The Cl-/HCO3- exchange protein band 3, or anion exchanger 1, is the most abundant protein in the erythrocyte membrane, facilitates the transport of CO2 through the body (9), and controls the rate of glycolysis in the erythrocyte by reversible binding of key enzymes such as glyceraldehyde 3-phosphate dehydrogenase (10). Band 3 is present in three distinct protein complexes within the erythrocyte membrane: as an ankyrin-bound, tetrameric band 3 complex, as a dimeric band 3 complex bound to the protein 4.1–GPC junctional complex, and as freely diffusing dimeric band 3 complexes (Figure 2) (11). The cytoplasmic domain of band 3 functions as the main anchorage site of the plasma membrane for the cytoskeleton by Figure 2. Band 3 multiprotein complexes in the human erythrocyte membrane. CA II – carbonic anhydrase II, GAPDH – glyceraldehyde 3-phosphate dehydrogenase, GPA – glycophorin A, GPB – glycophorin B, GPC – glycophorin C, Hb – hemoglobin, LW – Lewis blood group system, PFK – phosphofructokinase, Rh – rhesus blood group system, RhAG – Rh-associated glycoprotein blood group system (van den Akker et al.(11), adapted from Salomao et al.(17)) 218 Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 Figure 3. Phospholipid distribution and its regulation in the erythrocyte membrane. ATP – adenosine triphosphate, PC – phosphatidylcholine, PE – phosphatidylethanolamine, PS – phosphatidylserine, SM – sphingomyelin (© Frans Kuypers 2011) binding ankyrin, protein 4.1, protein 4.2 and adducin (12-14), and thereby plays a crucial role in the mechanical integrity and the deformability of the erythrocyte. Band 3 also interacts with various integral membrane proteins including glycophorin A, RhAG and/or Rh from the rhesus complex (Figure 2) (15, 16). Erythrocyte deformability Another mechanism of removal centers on the reduced deformability of aged erythrocytes (18-20). Erythrocyte deformability is governed by the viscosity of the cytoplasm - largely determined by its hemoglobin concentration -, the surface area-to-volume ratio (S/V), and the mechanical properties of the plasma membrane - primarily determined by its protein and lipid constituent organization - including the interaction between plasma membrane constituents with the cytoskeleton (19, 21, 22). As previously mentioned, the erythrocyte has to undergo large deformations in order to pass through the narrow capillaries of the microvasculature and the fenestrae in the spleen. Poorly deformable erythrocytes tend to get stuck in the spleen, which may trigger phagocytosis (23-25). Indeed, enhanced splenic sequestration of abnormal erythrocytes with reduced deformability is associated with a decreased life span and anemia in several erythrocyte membranopathies (26). During its time in the circulation, the erythrocyte loses membrane surface due to continuous membrane vesiculation (27-29). This vesicle shedding is thought to constitute a mechanism for the removal of damaged/aged membrane patches, postponing the untimely recognition and elimination of functional erythrocytes (29-33). In addition, vesiculation also contributes to the gradual loss in deformability observed during physiological erythrocyte aging (34), as it leads to a reduced S/V ratio and increased mean cellular hemoglobin concentration (34, 35). This might induce their eventual removal by splenic sequestration. Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 Phosphatidylserine exposure The lipid part of the plasma membrane of the erythrocyte is composed of equal proportions of cholesterol and phospholipids (26). While cholesterol is evenly distributed between the outer and inner leaflet of the membrane, the four dominant phospholipids are asymmetrically distributed. Phosphatidylcholine and sphingomyelin (SM) are primarily located in the outer leaflet, while phosphatidylethanolamine and phosphatidylserine (PS) are predominantly found in the inner leaflet (Figure 3) (36, 37). Various phospholipid transport proteins have been implicated in membrane phospholipid asymmetry. “Flippases” transport phospholipids from the extracellular to the cytoplasmic membrane leaflet, while “floppases” do the opposite, both in an energy-dependent manner (Figure 3). In contrast, “scramblases” move phospholipids bidirectionally down their concentration gradients by an energy-independent mechanism that is triggered by a rise in cytoplasmic calcium (Figure 3) (37). A novel calcium-activated cation channel (TMEM16F) required for calcium-induced membrane phospholipid scrambling was recently identified, and was found to be mutated in patients with Scott syndrome, a disease characterized by defective calcium-induced phospholipid scrambling activity (38-40). The plasma membrane lipid composition is involved in erythrocyte homeostasis (41, 42), as exemplified by the altered erythrocyte morphology and survival in patients with hemoglobinopathies and severe liver diseases, due to a disturbed membrane lipid asymmetry and lipid metabolism, respectively (42, 43). The maintenance of phospholipid asymmetry, in particular the exclusive localization of PS in the inner plasma membrane leaflet, has several functional implications. One such implication is the association between an increase in PS exposure and vesiculation (44). Externalization of PS to the outer leaflet of the plasma membrane is a hallmark of apoptotic cell death for 219 many cell types (45-48). Once exposed, PS is recognized by macrophages which in turn phagocytoze the targeted cell, either directly via PS receptors (4951), or through PS-mediated opsonisation of cells with lactadherin (52, 53). This has led to the broadly supported postulate that PS exposure by erythrocytes promotes their removal from the circulation. PS exposure on erythrocytes indeed leads to their phagocytosis by Kupffer cells of the liver and macrophages of the spleen in mice (54). A recent study has shown that stress-induced PS exposure by erythrocytes leads to their recognition by PS receptors TIM-1 and TIM-4, and triggers their removal by TIM-1 and TIM-4-positive phagocytes (49). Another study demonstrated that endothelial cells bind PS-positive erythrocytes via stabillin-1 and 2, greatly enhancing phagocytosis of these erythrocytes (55). These findings suggest that liver, splenic, and/or vascular endothelium cooperate with resident macrophages in the removal of PS-positive erythrocytes. Interestingly, few erythrocytes (<1%) in the human circulation expose PS regardless of their age (56), suggesting that PS exposure either does not occur during physiological erythrocyte aging, or leads to the rapid removal of the PS-exposing erythrocyte. In erythrocyte pathologies such as sickle cell anemia, thalassemia and spherocytosis, erythrocyte survival inversely correlated with phosphatidylserine exposure (57). Another mechanism involved in erythrocyte removal involves the membrane protein CD47. CD47 is generally known as a marker of “self”, as it has been shown to inhibit erythrocyte phagocytosis by macrophages of the reticulo-endothelial system (58-60). A recent study adds another dimension to the CD47 story, by showing that a conformational change in CD47 induced by experimental erythrocyte aging enables thrombospondin binding and subsequent phagocytosis by splenic macrophages in vitro (61). It is reasonable to assume that several of the abovementioned clearance mechanisms act simultaneously in an effort to efficiently remove old and/or damaged erythrocytes in vivo. Side effects of erythrocyte transfusion Erythrocyte transfusions are given to raise the hemoglobin concentration in patients with severe anemia, or after acute blood loss due to surgery and trauma. Erythrocytes as well as platelets and plasma are isolated from whole blood of healthy donors by centrifugation. The collected erythrocytes are stored in specially designed plastic bags containing a preservative solution at 4°C. In the Netherlands, the leukocyte numbers in the product are strongly reduced by centrifugation and subsequent filtration prior to storage in SAG-M preservation solution. Dutch legislation dictates that erythrocyte concentrates can only be used for transfusion within 35 days after their collection, in order to meet the international quality standards of 75% erythrocyte survival at 24 hours after transfusion and 0.8% hemolysis in the concentrate (62, 63). 220 Although the more than 100 million annual voluntary blood donations help save millions of lives worldwide (64), erythrocyte transfusions can also have serious side effects, such as acute lung injury, iron deposition resulting in severe organ damage, vasoconstriction, and formation of alloantibodies and autoantibodies (65). There are a number of changes that occur during erythrocyte storage that may cause the observed side effects after transfusion. These “storage lesions” include vesiculation (30, 66), decreased deformability (67, 68), decreased 2,3-bisphosphoglycerate (69), ATP and glutathione (70) concentrations, potassium leakage (71), and hemolysis (72). Immune-mediated side effects The erythrocyte contains a complex set of regulatory systems that may induce erythrocyte removal after physiological or pathological injury such as osmotic shock, oxidative stress and/or energy depletion (73). Modulation of these pathways is progressively lost during storage (74, 75), and this may result in accelerated aging and the removal of up to 30% of the transfused erythrocytes within 24 hours after transfusion (76). Disruption of these systems likely include a reduction of the threshold for activation of the pathways governing PS exposure (77), and may trigger aberrant expression of pathogenic epitopes on stored erythrocytes and their vesicles (78). Frequent erythrocyte transfusions may induce the formation of alloantibodies. This is especially problematic in the steadily increasing number of transfusion-dependent patients. Almost half of these patients acquire alloantibodies at some point in time, and in approximately 10% of the patients erythrocyte autoantibodies are detected. Some patients that produce these autoantibodies develop autoimmune hemolytic anemia, which can be life-threatening (79, 80). Observations such as these suggest that erythrocyte antigenicity changes during storage, potentially leading to autoantibody production after transfusion against these neoantigens. Murine studies suggest that erythrocyte transfusions can augment inflammation (81, 82), that may enhance the risk of immune responses towards erythrocyte autoantigens. Storage duration versus clinical outcome The wealth of data available on the gradual changes observed in the erythrocyte during storage (83) has long since sparked the discussion that longer storage time increases the risk of transfusion side effects. Multiple studies have reported that increased storage age of transfused erythrocytes is an independent risk factor for a number of adverse endpoints (84-90). In contrast, several other studies did not find any difference between short and long stored erythrocytes on clinical outcome (91-94). The use of either leukocyte-reduced or non-leukocyte-reduced erythrocyte products in these studies may explain the observed discrepancies (95). Thus far, there are no completed prospective randomized controlled studies examining the effect of storage duration of transfused erythrocytes on morbidity and mortality (95-97). To definitively answer this question two large clinical trials are Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 currently underway: The US-based initiative Red Cell Storage Duration Study (RECESS), and the complementary UK and Canadian co-initiative Age of Blood Evaluation (ABLE) (97). Anemia of inflammation Inflammation arising from various etiologies, including autoimmune disorders, infection and in particular sepsis, promote anemia (98-100). The preferred treatment is directed at the underlying disease. However, when inflammation persists there are only a few options for treatment of “anemia of inflammation” (98). Approximately 40% of critically ill individuals, including those with severe sepsis, receive at least one erythrocyte concentrate in the intensive care unit, with a mean of five concentrates per patient, equaling half of the total human blood volume. In these patients, erythrocyte transfusions are associated with increased morbidity and mortality (100). Because anemia is a comorbid condition that is associated with poor outcomes in various chronic disease states, understanding its pathogenesis is essential for the development of new remedies (98). Next to changes in systemic iron homeostasis and defective erythropoiesis (98, 99), also a reduced erythrocyte lifespan contributes to anemia of inflammation (101-103). While iron homeostasis and defective erythropoiesis have been extensively studied in these conditions, erythrocyte survival has received little attention so far (98). Phagocytic capacity is enhanced during inflammation (104), providing a possible explanation for enhanced erythrocyte clearance. Alternatively, the wide range of changes occurring in the circulation during systemic inflammation might impact erythrocyte characteristics directly. Indeed, alterations in erythrocyte shape, deformability, and aggregability were observed in patients with severe sepsis (105, 106). To date no mechanistic explanation has been provided for these changes. Erythrocyte membrane lipid remodeling in anemia of inflammation Membrane protein modification could not be causally linked to the altered erythrocyte rheology observed in patients with severe sepsis (107). However, lipid metabolism is markedly altered during inflammation, as exemplified by enhanced lipase activity and by changes in lipid constituents in the plasma (108), and could thus affect erythrocyte membrane lipid composition. This hypothesis is supported by the finding that the incubation of erythrocytes from healthy volunteers with plasma of septic patients resulted in enhanced PS exposure and ceramide content (109). Ceramide is a bioactive lipid involved in many cellular processes including apoptosis, senescence and inflammation (110, 11), possibly associated with the tendency of signaling receptors to cluster in ceramide-enriched platforms. In addition, the formation of these platforms alters membrane curvature and decreases plasma membrane integrity (112, 113). Sphingomyelinases (SMases) are the principal enzymes for the generation of ceramide (114). Since in a variety of diseases, including sepsis, inflammation triggers Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 the secretion of acid SMase in the blood, this SMase is likely responsible for the ceramide formation in erythrocytes (109). III - Microparticles Microparticles (MPs) were first described by Peter Wolf in 1967, when he observed a halo of debris surrounding activated platelets which he termed “platelet dust” (115). They are defined as plasma membrane-derived vesicles with a diameter of 100 to 1000 nm that expose molecules specific to the parental cell (116-118). The majority of the blood-borne MPs are generated by erythrocytes and platelets (118-120). Depending on their origin, MPs may contain an array of signaling molecules, including receptors, cytokines and bioactive lipids, but also mRNA and microRNA. This molecular composition renders MPs vectors of biological information. As such they play an active role in homeostasis and pathogenesis, the latter including atherosclerosis, various malignancies, autoimmune disorders, and infection (117, 121). Erythrocyte-derived microparticles During aging, the erythrocyte produces numerous vesicles, often termed red cell microparticles (RMPs), that expose PS and autoantigens, which are probably responsible for their rapid removal from the circulation (30, 31, 120, 122). Data from in vitro studies suggest that RMPs are likely to be actively involved in pathophysiology as well. For example, RMPs from erythrocyte storage units were found to modulate platelet function (123), and to be highly procoagulant (124, 125). RMPs can transfer biologically active molecules, exemplified by the transfer of CD59 from control erythrocytes to CD59-lacking erythrocytes of patients with paroxysmal nocturnal hemoglobinuria (126). Furthermore, RMPs may contribute to the procoagulant state and vaso-occlusions in sickle cell disease (119, 127). RMPs from malaria-infected erythrocytes were found to be major inducers of systemic inflammation during malaria infection (128, 129). Platelet-derived microparticles In contrast to what the name implies, the majority of the ‘platelet-derived microparticles’ (PMPs) in the circulation are not derived from platelets, but from megakaryocytes (130, 131). PMPs are likely to be important mediators of coagulation, not only by exposing procoagulant factors (118, 125, 132), but also by providing a platform for the binding of additional platelets to the subendothelial matrix (118, 133). PMPs may be involved in various other processes, such as hemostasis, maintenance of vascular health, and immunity (134). Prominent examples are the involvement of PMPs in vasoregeneration (135, 136), and their assistance in leukocyte-leukocyte interaction via P-selectin binding to PSGL-1 (137). A recent study showed that enhanced glycoprotein VI-mediated PMP generation leads to a PMP build-up in the joint fluid of patients suffering from inflammatory arthritis (but not osteoarthritis), inducing an inflammatory response via interleukin-1 signaling (138). 221 Microparticles in transfusion medicine Not only in vivo, but also in vitro during blood bank storage, erythrocytes and platelets shed MPs (30, 139). These MPs may be responsible for some of the side-effects commonly observed after transfusion (140-144). RMPs from storage products are enriched in removal signals such as PS, immunoglobulins, and complement (30, 144). The supernatant of erythrocyte transfusion units, which contains many RMPs that were shed during storage, was found to have the ability to modulate the functions of T cells (141), neutrophils (145), macrophages (140), and monocytes (146) in vitro. Transfusion unit supernatants also caused lung inflammation and coagulopathy in a rat model (147). These findings strengthen the view that a high dose of RMPs may induce or augment the inflammatory and/ or immunological side-effects of transfusion, including autoantibody formation (148). Next to coagulation, platelets also have an important role as immune mediators (149, 150), making PMPs likely candidates for immune regulation as well (143, 151-153). Side-effects of platelet transfusion include fever and acute lung injury (152), and enhanced PMP levels in platelet units correlated with various allergic transfusion reactions (151). The ability of PMPs to interact with leukocytes (137, 151), as well as their potential to induce CD40L-mediated B cell activation (154), underscore their ability to affect the immune system. The plethora of signaling molecules on PMPs makes it even more likely that they contribute to the transfusion burden (134, 155). While most circulating PMPs originate from megakaryocytes (130, 131), P-selectin-positive PMPs from platelet transfusion units constitute an important part of the storage PMP burden, and likely have distinct biological activities (151, 156). IV - The immune system Our immune system has evolved to defend the body against harmful pathogens. Immune responses are strictly regulated to allow rapid initiation of immune activity upon infection, and quick resolution of the response after elimination of the pathogen, in order to prevent tissue damage. In addition, the immune system must be kept in a resting state in normal situations to prevent harmful responses against the body’s own tissues and the commensal microorganisms. Parallel to immune surveillance, immune cells also provide essential support for tissue homeostasis and function (157). The immune response Tissue injury caused by pathogens and/or trauma triggers the local release of various soluble proinflammatory mediators, including chemokines and the cytokines IL-1 and TNF-α by specialized cells such as resident macrophages. IL-1 and TNF-α promote the expression of selectins and integrins by the local vascular endothelium, enabling the adhesion, arrest, and extravasation of leukocytes, which subsequently migrate along the chemokine gradient towards the inflamed tissue (158). Platelets adhere to the exposed extracellular matrix and the inflamed 222 endothelial cells, further activating the endothelium and adhering monocytes, and release additional pro-inflammatory factors including IL-1 (159, 160). At the site of tissue injury, neutrophils engulf pathogens and compromised cells, and subsequently release proteolytic enzymes and oxygen metabolites which digest the phagocytozed material (158). Monocytes recruited to the inflamed tissue differentiate into different types of pro-inflammatory macrophages. Next to their function in phagocytozing pathogens, dead cells and cell debris, these macrophages are the primary orchestrators of tissue inflammation (161). Within days, a specific response is mustered due to antigen presentation to T and B cells by antigenpresenting cells like macrophages and dendritic cells. CD4+ helper T (TH) cells support the further activation of other effector cells of the adaptive immune system including B cells and CD8+ cytotoxic T cells, through cell-cell interactions and the release of cytokines. The activated and differentiated B cells secrete antibodies that bind the antigen-exposing pathogen, assisting in their recognition by other effector cells. Activated cytotoxic T cells search for infected cells in the body that expose the antigen they are primed against, and kill these cells by disrupting their membrane and releasing an array of cytotoxins (157, 158). Immune cells regulate tissue homeostasis Initially, inflamed tissue is dominated by M1-polarized macrophages which promote further leukocyte influx and TH1-mediated and TH17-mediated inflammatory responses by producing IL-1, TNF-α, IL-12 and IL-23. Inflammation must be resolved in a timely manner to avoid unnecessary tissue damage. M2-polarized macrophages that do not secrete IL-12 , but instead produce anti-inflammatory factors such as IL-10, TGF-β, IL-1 decoy receptor and IL1-RA, gradually appear in the inflamed tissue to dampen the inflammatory process (161, 162). They further consolidate the resolution of inflammation by inducing regulatory T cell (Treg) differentiation (163), and by actively recruiting Tregs through the release of CCL22 (164). Tregs that express the transcription factor Foxp3 play a critical role in maintaining immune homeostasis and dominant self-tolerance through a combination of cellcell interactions, the release of soluble factors including the anti-inflammatory cytokines IL-10, TGF-β and IL-35, and the scavenging of the T cell survival factor IL-2 (Figure 4). The majority of the Foxp3+ Tregs are produced in the thymus as an antigen-primed and functionally mature T cell subpopulation (naturallyoccurring Tregs), while some Tregs differentiate from naïve conventional T cells in the periphery (induced Tregs) (165, 166). Aside from their ability to suppress effector cell priming in lymphoid tissues (167-170), Tregs are also able to suppress myeloid populations and effector cells in other tissues (171). Tregs have been shown to drive monocyte differentiation towards a M2-like macrophage phenotype, suggesting they consolidate the anti-inflammatory macrophage phenotype (172). Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 Figure 4. Mechanisms potentially used by Tregs to assert tissue homeostasis in the steady state, during 'damage control' in inflamed tissue, and for infectious tolerance after resolution of inflammation. iTreg – induced Treg cell, TGF-βR – TGF-β receptor, nTreg – natural Treg cell, CO – carbon monoxide, IFN-γR – IFN-γ receptor (Tang et al. (173)) During the resolution of inflammation, TGF-β and other growth factors such as VEGF, FGF and PDGF, that are released by macrophages, platelets (174), Tregs (171, 175) and various other cell types (174), promote angiogenesis, tissue regeneration and wound repair. Macrophages further regulate wound healing by phagocytozing debris, apoptotic neutrophils, and extracellular matrix (ECM) components that promote inflammation (176, 177), and by releasing factors that control ECM turnover (178). This macrophagegoverned healing process is tightly regulated in order to restore homeostatic tissue architecture and function, while preventing fibrosis and scarring. In summary, the immune system sustains tissue homeostasis by disposing of invading pathogens and by supporting tissue repair and maintenance. V - Scope of the thesis Physiological erythrocyte aging leads to membrane alterations ultimately responsible for their removal from the circulation. Similar membrane changes occur during erythrocyte blood banking, and could explain the high removal rate of part of the erythrocytes shortly after transfusion and the transfusion side Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 effects. Furthermore, the changes in the erythrocyte membrane that occur during systemic inflammation might explain a reduced erythrocyte lifespan contributing to the development of anemia. In recent years, increased awareness of the importance of microparticles in homeostasis, various diseases and transfusion medicine, has stimulated research on their exact nature and function. The aim of this thesis is to provide more insight into the erythrocyte membrane changes that occur during storage and systemic inflammation, including vesiculation. In addition, we studied the potential impact of platelet-derived microparticles on the immune system. The potential formation of pathological antigens during erythrocyte storage was investigated in Chapter 2. Using patient plasma containing anti-erythrocyte autoantibodies, immunoprecipitations were performed with erythrocytes and MPs from concentrates of increasing storage periods. Antigen recognition by patient plasma autoantibodies was associated with storage time, and several membrane proteins could be identified as candidate antigens. The composition of the immune complexes recognized on the MPs was markedly different from those on the erythrocytes, 223 indicating that their immunization potential differs from that of their parental cells. These data corroborate the theory that deregulation of the mechanisms governing erythrocyte aging contributes to transfusioninduced alloantibody and autoantibody formation. In Chapter 3, we assessed the potential of PS exposure as a parameter for donor-dependent variation in product quality. PS exposure was determined just prior to, and during a 35-day storage period, and was found to correlate with common blood bank quality parameters and some donor characteristics. PS exposure increased with storage time, and correlated with hemolysis and MP concentration in the concentrate, and with the plasma hemoglobin concentration of the donor. Furthermore, the initial level of PS exposure was found to be predictive for PS exposure after osmotic stress. These findings support the use of PS exposure as a donor-dependent, biologically relevant parameter for erythrocyte transfusion unit quality. During systemic inflammation, as occurs in patients with severe sepsis, the lipid metabolism in the circulation is markedly altered, involving an enhanced activity of several lipases such as SMases. The functional consequences of these enzymes on erythrocyte structure and function were studied in detail in Chapter 4. We found erythrocytes to be very sensitive to SMase-induced ceramide formation in the membrane. Ceramide build-up led to the loss of the discoid shape, followed by PS exposure and loss of cell integrity. In this process, markedly enhanced vesiculation and reduced deformability were also observed. Erythrocytes aged in vivo and in vitro were more sensitive to SMase-induced changes than younger erythrocytes. This study indicates that SMase has the potential to alter pathophysiologically relevant erythrocyte parameters, which is especially important in the context of erythrocyte transfusion in patients with prolonged systemic inflammation. Based on the results described in Chapter 4, we investigated sepsis-associated changes in the erythrocyte membrane lipid composition. In Chapter 5, we analyzed the plasma membrane lipid content of freshly isolated erythrocytes from healthy volunteers after incubation with the plasma of patients with septic shock. While ceramide could not be detected, we found markedly increased levels of lysophosphatidylcholine (LPC), which is produced by phospholipase A2. Although secretory phospholipase A2 IIA was greatly enhanced in the septic patient plasmas, its concentration did not correlate with the LPC levels. Enhanced LPC levels were not detected when erythrocytes were incubated with the plasma of healthy volunteers, in whom sepsis was simulated using a low dose of lipopolysaccharide. Interestingly, erythrocyte PS exposure increased in these subjects after lipopolysaccharide infusion. These data provide evidence for active remodeling, during sepsis, of the lipid compartment of the erythrocyte membrane, which is likely to affect erythrocyte survival. During the course of our studies we extensively studied cell-derived MPs from various sources. The isolation, analysis and quantification of these MPs is challenging due to their small and heterogeneous size. Based on 224 our experience, we present our perspective on the do’s and don’ts regarding RMP and PMP isolation and characterization in Chapter 6. A novel regulatory function of PMPs on regulatory T cell stability is presented in Chapter 7. In this chapter we show that PMPs selectively bind to a specialized subset of Foxp3+ regulatory T cells, and that PMPs inhibit their differentiation into potentially pathogenic effector cells in a pro-inflammatory microenvironment. Our data indicate the direct involvement of the adhesion molecule P-selectin and thus suggest a role for PMPs in vascular healing by regulating the regulators at the sites of vascular insult. In Chapter 8, the findings reported in this manuscript are summarized and discussed, and future perspectives are outlined. References 1. Gregory CJ, Eaves AC. Three stages of erythropoietic progenitor cell differentiation distinguished by a number of physical and biologic properties. Blood 51(3), 527-537 (1978). 2. Kundu M, Lindsten T, Yang CY et al. Ulk1 plays a critical role in the autophagic clearance of mitochondria and ribosomes during reticulocyte maturation. Blood 112(4), 1493-1502 (2008). 3. Zhang J, Randall MS, Loyd MR et al. Mitochondrial clearance is regulated by Atg7-dependent and -independent mechanisms during reticulocyte maturation. Blood 114(1), 157-164 (2009). 4. Chasis JA, Prenant M, Leung A, Mohandas N. Membrane assembly and remodeling during reticulocyte maturation. Blood 74(3), 1112-1120 (1989). 5. Waugh RE, Mantalaris A, Bauserman RG, Hwang WC, Wu JH. Membrane instability in late-stage erythropoiesis. Blood 97(6), 1869-1875 (2001). 6. Dornhorst AC. The interpretation of red cell survival curves. Blood 6(12), 1284-1292 (1951). 7. Kay M. Immunoregulation of cellular life span. Ann. N. Y. Acad. Sci. 1057 85-111 (2005). 8. Pantaleo A, Ferru E, Giribaldi G et al. Oxidized and poorly glycosylated band 3 is selectively phosphorylated by Syk kinase to form large membrane clusters in normal and G6PD-deficient red blood cells. Biochem. J. 418(2), 359-367 (2009). 9. Alper SL. Molecular physiology of SLC4 anion exchangers. Exp. Physiol 91(1), 153-161 (2006). 10.Campanella ME, Chu H, Low PS. Assembly and regulation of a glycolytic enzyme complex on the human erythrocyte membrane. Proc. Natl. Acad. Sci. U. S. A 102(7), 2402-2407 (2005). 11. van den Akker E, Satchwell TJ, Williamson RC, Toye AM. Band 3 multiprotein complexes in the red cell membrane; of mice and men. Blood Cells Mol. Dis. 45(1), 1-8 (2010). 12. Anong WA, Franco T, Chu H et al. Adducin forms a bridge between the erythrocyte membrane and its cytoskeleton and regulates membrane cohesion. Blood 114(9), 19041912 (2009). 13.Toye AM, Ghosh S, Young MT et al. Protein-4.2 association with band 3 (AE1, SLCA4) in Xenopus oocytes: effects of three natural protein-4.2 mutations associated with hemolytic anemia. Blood 105(10), 40884095 (2005). 14. Zhang D, Kiyatkin A, Bolin JT, Low PS. Crystallographic structure and functional interpretation of the cytoplasmic domain of erythrocyte membrane band 3. Blood 96(9), 2925-2933 (2000). Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 15.Beckmann R, Smythe JS, Anstee DJ, Tanner MJ. Coexpression of band 3 mutants and Rh polypeptides: differential effects of band 3 on the expression of the Rh complex containing D polypeptide and the Rh complex containing CcEe polypeptide. Blood 97(8), 2496-2505 (2001). 16. Bruce LJ, Beckmann R, Ribeiro ML et al. A band 3-based macrocomplex of integral and peripheral proteins in the RBC membrane. Blood 101(10), 4180-4188 (2003). 17. Salomao M, Zhang X, Yang Y et al. Protein 4.1R-dependent multiprotein complex: new insights into the structural organization of the red blood cell membrane. Proc. Natl. Acad. Sci. U. S. A 105(23), 8026-8031 (2008). 18. Mchedlishvili G. Disturbed blood flow structuring as critical factor of hemorheological disorders in microcirculation. Clin. Hemorheol. Microcirc. 19(4), 315325 (1998). 19. Mohandas N, Chasis JA. Red blood cell deformability, membrane material properties and shape: regulation by transmembrane, skeletal and cytosolic proteins and lipids. Semin. Hematol. 30(3), 171-192 (1993). 20. Parthasarathi K, Lipowsky HH. Capillary recruitment in response to tissue hypoxia and its dependence on red blood cell deformability. Am. J. Physiol 277(6 Pt 2), H2145-H2157 (1999). 21. Mohandas N, Evans E. Mechanical properties of the red cell membrane in relation to molecular structure and genetic defects. Annu. Rev. Biophys. Biomol. Struct. 23 787-818 (1994). 22. Mokken FC, Kedaria M, Henny CP, Hardeman MR, Gelb AW. The clinical importance of erythrocyte deformability, a hemorrheological parameter. Ann. Hematol. 64(3), 113122 (1992). 23. Mebius RE, Kraal G. Structure and function of the spleen. Nat. Rev. Immunol. 5(8), 606-616 (2005). 24. Deplaine G, Safeukui I, Jeddi F et al. The sensing of poorly deformable red blood cells by the human spleen can be mimicked in vitro. Blood 117(8), e88-e95 (2011). 25. Safeukui I, Buffet PA, Deplaine G et al. Quantitative assessment of sensing and sequestration of spherocytic erythrocytes by the human spleen. Blood 120(2), 424-430 (2012). 26. Mohandas N, Gallagher PG. Red cell membrane: past, present, and future. Blood 112(10), 3939-3948 (2008). 27. Willekens FL, Roerdinkholder-Stoelwinder B, GroenenDopp YA et al. Hemoglobin loss from erythrocytes in vivo results from spleen-facilitated vesiculation. Blood 101(2), 747-751 (2003). 28. Willekens FL, Werre JM, Kruijt JK et al. Liver Kupffer cells rapidly remove red blood cell-derived vesicles from the circulation by scavenger receptors. Blood 105(5), 21412145 (2005). 29.Willekens FL, Werre JM, Groenen-Dopp YA, Roerdinkholder-Stoelwinder B, de Pauw B, Bosman GJ. Erythrocyte vesiculation: a self-protective mechanism? Br. J. Haematol. 141(4), 549-556 (2008). 30. Bosman GJ, Lasonder E, Luten M et al. The proteome of red cell membranes and vesicles during storage in blood bank conditions. Transfusion 48(5), 827-835 (2008). 31. Bosman GJ, Lasonder E, Groenen-Dopp YA, Willekens FL, Werre JM. The proteome of erythrocyte-derived microparticles from plasma: new clues for erythrocyte aging and vesiculation. J. Proteomics. (2012). 32.Ferru E, Giger K, Pantaleo A et al. Regulation of membrane-cytoskeletal interactions by tyrosine phosphorylation of erythrocyte band 3. Blood 117(22), 5998-6006 (2011). 33. Bosch FH, Werre JM, Schipper L et al. Determinants of red blood cell deformability in relation to cell age. Eur. J. Haematol. 52(1), 35-41 (1994). 34.Bosch FH, Werre JM, Roerdinkholder-Stoelwinder B, Huls TH, Willekens FL, Halie MR. Characteristics of red Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 blood cell populations fractionated with a combination of counterflow centrifugation and Percoll separation. Blood 79(1), 254-260 (1992). 35.Verkleij AJ, Zwaal RF, Roelofsen B, Comfurius P, Kastelijn D, van Deenen LL. The asymmetric distribution of phospholipids in the human red cell membrane. A combined study using phospholipases and freeze-etch electron microscopy. Biochim. Biophys. Acta 323(2), 178193 (1973). 36. Zwaal RF, Schroit AJ. Pathophysiologic implications of membrane phospholipid asymmetry in blood cells. Blood 89(4), 1121-1132 (1997). 37. Daleke DL. Regulation of phospholipid asymmetry in the erythrocyte membrane. Curr. Opin. Hematol. 15(3), 191-195 (2008). 38. Castoldi E, Collins PW, Williamson PL, Bevers EM. Compound heterozygosity for 2 novel TMEM16F mutations in a patient with Scott syndrome. Blood 117(16), 4399-4400 (2011). 39.Suzuki J, Umeda M, Sims PJ, Nagata S. Calciumdependent phospholipid scrambling by TMEM16F. Nature 468(7325), 834-838 (2010). 40. Yang H, Kim A, David T et al. TMEM16F forms a Ca2+activated cation channel required for lipid scrambling in platelets during blood coagulation. Cell 151(1), 111-122 (2012). 41. Daleke DL. Regulation of phospholipid asymmetry in the erythrocyte membrane. Curr. Opin. Hematol. 15(3), 191195 (2008). 42. Kuypers FA. Red cell membrane lipids in hemoglobinopathies. Curr. Mol. Med. 8(7), 633-638 (2008). 43. Morse EE. Mechanisms of hemolysis in liver disease. Ann. Clin. Lab Sci. 20(3), 169-174 (1990). 44.Bucki R, Bachelot-Loza C, Zachowski A, Giraud F, Sulpice JC. Calcium induces phospholipid redistribution and microvesicle release in human erythrocyte membranes by independent pathways. Biochemistry 37(44), 1538315391 (1998). 45. Fadok VA, Voelker DR, Campbell PA, Cohen JJ, Bratton DL, Henson PM. Exposure of phosphatidylserine on the surface of apoptotic lymphocytes triggers specific recognition and removal by macrophages. J. Immunol. 148(7), 2207-2216 (1992). 46. Bratton DL, Fadok VA, Richter DA, Kailey JM, Guthrie LA, Henson PM. Appearance of phosphatidylserine on apoptotic cells requires calcium-mediated nonspecific flip-flop and is enhanced by loss of the aminophospholipid translocase. J. Biol. Chem. 272(42), 26159-26165 (1997). 47. Brown SB, Clarke MC, Magowan L, Sanderson H, Savill J. Constitutive death of platelets leading to scavenger receptor-mediated phagocytosis. A caspase-independent cell clearance program. J. Biol. Chem. 275(8), 5987-5996 (2000). 48. Kamp D, Sieberg T, Haest CW. Inhibition and stimulation of phospholipid scrambling activity. Consequences for lipid asymmetry, echinocytosis, and microvesiculation of erythrocytes. Biochemistry 40(31), 9438-9446 (2001). 49. Kobayashi N, Karisola P, Pena-Cruz V et al. TIM-1 and TIM-4 glycoproteins bind phosphatidylserine and mediate uptake of apoptotic cells. Immunity. 27(6), 927-940 (2007). 50. Oka K, Sawamura T, Kikuta K et al. Lectin-like oxidized low-density lipoprotein receptor 1 mediates phagocytosis of aged/apoptotic cells in endothelial cells. Proc. Natl. Acad. Sci. U. S. A 95(16), 9535-9540 (1998). 51. Park SY, Jung MY, Kim HJ et al. Rapid cell corpse clearance by stabilin-2, a membrane phosphatidylserine receptor. Cell Death. Differ. 15(1), 192-201 (2008). 52.Fens MH, Mastrobattista E, de Graaff AM et al. Angiogenic endothelium shows lactadherin-dependent phagocytosis of aged erythrocytes and apoptotic cells. Blood 111(9), 4542-4550 (2008). 225 53. Hanayama R, Tanaka M, Miwa K, Shinohara A, Iwamatsu A, Nagata S. Identification of a factor that links apoptotic cells to phagocytes. Nature 417(6885), 182-187 (2002). 54. Schroit AJ, Madsen JW, Tanaka Y. In vivo recognition and clearance of red blood cells containing phosphatidylserine in their plasma membranes. J. Biol. Chem. 260(8), 5131-5138 (1985). 55. Lee SJ, Park SY, Jung MY, Bae SM, Kim IS. Mechanism for phosphatidylserine-dependent erythrophagocytosis in mouse liver. Blood 117(19), 5215-5223 (2011). 56. Bosman GJ, Willekens FL, Werre JM. Erythrocyte aging: a more than superficial resemblance to apoptosis? Cell Physiol Biochem. 16(1-3), 1-8 (2005). 57. Kuypers FA, de Jong K. The role of phosphatidylserine in recognition and removal of erythrocytes. Cell Mol. Biol. (Noisy. -le-grand) 50(2), 147-158 (2004). 58. Oldenborg PA, Zheleznyak A, Fang YF, Lagenaur CF, Gresham HD, Lindberg FP. Role of CD47 as a marker of self on red blood cells. Science 288(5473), 2051-2054 (2000). 59. Oldenborg PA, Gresham HD, Lindberg FP. CD47-signal regulatory protein alpha (SIRPalpha) regulates Fcgamma and complement receptor-mediated phagocytosis. J. Exp. Med. 193(7), 855-862 (2001). 60.Olsson M, Oldenborg PA. CD47 on experimentally senescent murine RBCs inhibits phagocytosis following Fcgamma receptor-mediated but not scavenger receptormediated recognition by macrophages. Blood 112(10), 4259-4267 (2008). 61. Burger P, Hilarius-Stokman P, de Korte D, van den Berg TK, van Bruggen R. CD47 functions as a molecular switch for erythrocyte phagocytosis. Blood 119(23), 5512-5521 (2012). 62. Dumont LJ, AuBuchon JP. Evaluation of proposed FDA criteria for the evaluation of radiolabeled red cell recovery trials. Transfusion 48(6), 1053-1060 (2008). 63. European Directorate for the Quality of Medicines & HealthCare. Guide to the Preparation, Use, and Quality Assurance of Blood Components. 17 ed. Council of Europe publishing; 2013. 64. World Health Organization. Blood safety and availability - Fact sheet N°279. http://www.who.int/mediacentre/ factsheets/fs279/en/; 2013 Jul. Report No.: Fact sheet N°279. 65. Perrotta PL, Snyder EL. Non-infectious complications of transfusion therapy. Blood Rev. 15(2), 69-83 (2001). 66.Donadee C, Raat NJ, Kanias T et al. Nitric oxide scavenging by red blood cell microparticles and cell-free hemoglobin as a mechanism for the red cell storage lesion. Circulation 124(4), 465-476 (2011). 67. Bahrstein G, Manny N, Yedgar S. Circulatory risk in the transfusion of red blood cells with impaired flow properties induced by storage. Transfus. Med. Rev. 25(1), 24-35 (2011). 68. Berezina TL, Zaets SB, Morgan C et al. Influence of storage on red blood cell rheological properties. J. Surg. Res. 102(1), 6-12 (2002). 69.Bennett-Guerrero E, Veldman TH, Doctor A et al. Evolution of adverse changes in stored RBCs. Proc. Natl. Acad. Sci. U. S. A 104(43), 17063-17068 (2007). 70. Whillier S, Raftos JE, Sparrow RL, Kuchel PW. The effects of long-term storage of human red blood cells on the glutathione synthesis rate and steady-state concentration. Transfusion 51(7), 1450-1459 (2011). 71. de Korte D, Verhoeven AJ. Quality determinants of erythrocyte destined for transfusion. Cell Mol. Biol. (Noisy-le-grand) 50(2), 187-195 (2004). 72. Sowemimo-Coker SO. Red blood cell hemolysis during processing. Transfus. Med. Rev. 16(1), 46-60 (2002). 73. Lang KS, Lang PA, Bauer C et al. Mechanisms of suicidal erythrocyte death. Cell Physiol Biochem. 15(5), 195-202 (2005). 226 74.Antonelou MH, Kriebardis AG, Stamoulis KE, Economou-Petersen E, Margaritis LH, Papassideri IS. Red blood cell aging markers during storage in citratephosphate-dextrose-saline-adenine-glucose-mannitol. Transfusion 50(2), 376-389 (2010). 75. Messana I, Ferroni L, Misiti F et al. Blood bank conditions and RBCs: the progressive loss of metabolic modulation. Transfusion 40(3), 353-360 (2000). 76. Luten M, Roerdinkholder-Stoelwinder B, Schaap NP, de Grip WJ, Bos HJ, Bosman GJ. Survival of red blood cells after transfusion: a comparison between red cells concentrates of different storage periods. Transfusion 48(7), 1478-1485 (2008). 77. Bosman GJ, Cluitmans JC, Groenen YA, Werre JM, Willekens FL, Novotny VM. Susceptibility to hyperosmotic stress-induced phosphatidylserine exposure increases during red blood cell storage. Transfusion 51(5), 10721078 (2011). 78. Fossati-Jimack L, Azeredo da SS, Moll T et al. Selective increase of autoimmune epitope expression on aged erythrocytes in mice: implications in anti-erythrocyte autoimmune responses. J. Autoimmun. 18(1), 17-25 (2002). 79. Garratty G. Immune hemolytic anemia associated with negative routine serology. Semin. Hematol. 42(3), 156-164 (2005). 80. Young PP, Uzieblo A, Trulock E, Lublin DM, Goodnough LT. Autoantibody formation after alloimmunization: are blood transfusions a risk factor for autoimmune hemolytic anemia? Transfusion 44(1), 67-72 (2004). 81. Hod EA, Zhang N, Sokol SA et al. Transfusion of red blood cells after prolonged storage produces harmful effects that are mediated by iron and inflammation. Blood 115(21), 4284-4292 (2010). 82. Mangalmurti NS, Xiong Z, Hulver M et al. Loss of red cell chemokine scavenging promotes transfusion-related lung inflammation. Blood 113(5), 1158-1166 (2009). 83. Bosman GJ, Werre JM, Willekens FL, Novotny VM. Erythrocyte ageing in vivo and in vitro: structural aspects and implications for transfusion. Transfus. Med. 18(6), 335-347 (2008). 84. Baek JH, D'Agnillo F, Vallelian F et al. Hemoglobindriven pathophysiology is an in vivo consequence of the red blood cell storage lesion that can be attenuated in guinea pigs by haptoglobin therapy. J. Clin. Invest 122(4), 1444-1458 (2012). 85. Edgren G, Kamper-Jorgensen M, Eloranta S et al. Duration of red blood cell storage and survival of transfused patients (CME). Transfusion 50(6), 1185-1195 (2010). 86. Eikelboom JW, Cook RJ, Liu Y, Heddle NM. Duration of red cell storage before transfusion and in-hospital mortality. Am. Heart J. 159(5), 737-743 (2010). 87. Gauvin F, Spinella PC, Lacroix J et al. Association between length of storage of transfused red blood cells and multiple organ dysfunction syndrome in pediatric intensive care patients. Transfusion 50(9), 1902-1913 (2010). 88. Koch CG, Li L, Sessler DI et al. Duration of red-cell storage and complications after cardiac surgery. N. Engl. J. Med. 358(12), 1229-1239 (2008). 89. Sanders J, Patel S, Cooper J et al. Red blood cell storage is associated with length of stay and renal complications after cardiac surgery. Transfusion 51(11), 2286-2294 (2011). 90. Zallen G, Offner PJ, Moore EE et al. Age of transfused blood is an independent risk factor for postinjury multiple organ failure. Am. J. Surg. 178(6), 570-572 (1999). 91. Kor DJ, Kashyap R, Weiskopf RB et al. Fresh red blood cell transfusion and short-term pulmonary, immunologic, and coagulation status: a randomized clinical trial. Am. J. Respir. Crit Care Med. 185(8), 842-850 (2012). Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 92.Phelan HA, Eastman AL, Aldy K et al. Prestorage leukoreduction abrogates the detrimental effect of aging on packed red cells transfused after trauma: a prospective cohort study. Am. J. Surg. 203(2), 198-204 (2012). 93. Vamvakas EC, Carven JH. Length of storage of transfused red cells and postoperative morbidity in patients undergoing coronary artery bypass graft surgery. Transfusion 40(1), 101-109 (2000). 94. van de Watering L, Lorinser J, Versteegh M, Westendord R, Brand A. Effects of storage time of red blood cell transfusions on the prognosis of coronary artery bypass graft patients. Transfusion 46(10), 1712-1718 (2006). 95. van de Watering L. Pitfalls in the current published observational literature on the effects of red blood cell storage. Transfusion 51(8), 1847-1854 (2011). 96. Lee JS, Gladwin MT. Bad blood: the risks of red cell storage. Nat. Med. 16(4), 381-382 (2010). 97.Edelstein SB. Blood product storage: does age really matter? Semin. Cardiothorac. Vasc. Anesth. 16(3), 160165 (2012). 98. Roy CN. Anemia of inflammation. Hematology. Am. Soc. Hematol. Educ. Program. 2010 276-280 (2010). 99. Weiss G, Goodnough LT. Anemia of chronic disease. N. Engl. J. Med. 352(10), 1011-1023 (2005). 100.Napolitano LM, Kurek S, Luchette FA et al. Clinical practice guideline: red blood cell transfusion in adult trauma and critical care. Crit Care Med. 37(12), 3124-3157 (2009). 101.Manodori AB, Kuypers FA. Altered red cell turnover in diabetic mice. J. Lab Clin. Med. 140(3), 161-165 (2002). 102.Mitlyng BL, Singh JA, Furne JK, Ruddy J, Levitt MD. Use of breath carbon monoxide measurements to assess erythrocyte survival in subjects with chronic diseases. Am. J. Hematol. 81(6), 432-438 (2006). 103.Moldawer LL, Marano MA, Wei H et al. Cachectin/tumor necrosis factor-alpha alters red blood cell kinetics and induces anemia in vivo. FASEB J. 3(5), 1637-1643 (1989). 104.Brown GC, Neher JJ. Eaten alive! Cell death by primary phagocytosis: 'phagoptosis'. Trends Biochem. Sci. 37(8), 325-332 (2012). 105.Piagnerelli M, Boudjeltia KZ, Brohee D et al. Alterations of red blood cell shape and sialic acid membrane content in septic patients. Crit Care Med. 31(8), 2156-2162 (2003). 106.Reggiori G, Occhipinti G, De Gasperi A, Vincent JL, Piagnerelli M. Early alterations of red blood cell rheology in critically ill patients. Crit Care Med. 37(12), 3041-3046 (2009). 107.Piagnerelli M, Cotton F, van Nuffelen M, Vincent JL, Gulbis B. Modifications in erythrocyte membrane protein content are not responsible for the alterations in rheology seen in sepsis. Shock 37(1), 17-21 (2012). 108.Khovidhunkit W, Kim MS, Memon RA et al. Effects of infection and inflammation on lipid and lipoprotein metabolism: mechanisms and consequences to the host. J. Lipid Res. 45(7), 1169-1196 (2004). 109.Kempe DS, Akel A, Lang PA et al. Suicidal erythrocyte death in sepsis. J. Mol. Med. (Berl) 85(3), 273-281 (2007). 110.Grassme H, Riethmuller J, Gulbins E. Biological aspects of ceramide-enriched membrane domains. Prog. Lipid Res. 46(3-4), 161-170 (2007). 111.Hannun YA, Obeid LM. Principles of bioactive lipid signalling: lessons from sphingolipids. Nat. Rev. Mol. Cell Biol. 9(2), 139-150 (2008). 112.Goni FM, Alonso A. Sphingomyelinases: enzymology and membrane activity. FEBS Lett. 531(1), 38-46 (2002). 113.Lopez-Montero I, Monroy F, Velez M, Devaux PF. Ceramide: from lateral segregation to mechanical stress. Biochim. Biophys. Acta 1798(7), 1348-1356 (2010). 114.Goni FM, Alonso A. Sphingomyelinases: enzymology and membrane activity. FEBS Lett. 531(1), 38-46 (2002). 115.Wolf P. The nature and significance of platelet products in human plasma. Br. J. Haematol. 13(3), 269-288 (1967). Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3 116.Gyorgy B, Szabo TG, Pasztoi M et al. Membrane vesicles, current state-of-the-art: emerging role of extracellular vesicles. Cell Mol. Life Sci. 68(16), 2667-2688 (2011). 117.Thery C, Ostrowski M, Segura E. Membrane vesicles as conveyors of immune responses. Nat. Rev. Immunol. 9(8), 581-593 (2009). 118.Owens AP, III, Mackman N. Microparticles in hemostasis and thrombosis. Circ. Res. 108(10), 1284-1297 (2011). 119. van Beers EJ, Schaap MC, Berckmans RJ et al. Circulating erythrocyte-derived microparticles are associated with coagulation activation in sickle cell disease. Haematologica 94(11), 1513-1519 (2009). 120.Willekens FL, Roerdinkholder-Stoelwinder B, GroenenDopp YA et al. Hemoglobin loss from erythrocytes in vivo results from spleen-facilitated vesiculation. Blood 101(2), 747-751 (2003). 121.Mause SF, Weber C. Microparticles: protagonists of a novel communication network for intercellular information exchange. Circ. Res. 107(9), 1047-1057 (2010). 122.Willekens FL, Werre JM, Kruijt JK et al. Liver Kupffer cells rapidly remove red blood cell-derived vesicles from the circulation by scavenger receptors. Blood 105(5), 21412145 (2005). 123.Xiong Z, Cavaretta J, Qu L, Stolz DB, Triulzi D, Lee JS. Red blood cell microparticles show altered inflammatory chemokine binding and release ligand upon interaction with platelets. Transfusion 51(3), 610-621 (2011). 124.Gao Y, Lv L, Liu S, Ma G, Su Y. Elevated levels of thrombin-generating microparticles in stored red blood cells. Vox Sang. (2013). 125.van der Meijden PE, van Schilfgaarde M, van Oerle R, Renne T, ten Cate H, Spronk HM. Platelet- and erythrocyte-derived microparticles trigger thrombin generation via factor XIIa. J. Thromb. Haemost. 10(7), 1355-1362 (2012). 126.Sloand EM, Mainwaring L, Keyvanfar K et al. Transfer of glycosylphosphatidylinositol-anchored proteins to deficient cells after erythrocyte transfusion in paroxysmal nocturnal hemoglobinuria. Blood 104(12), 3782-3788 (2004). 127.Camus SM, Gausseres B, Bonnin P et al. Erythrocyte microparticles can induce kidney vaso-occlusions in a murine model of sickle cell disease. Blood 120(25), 50505058 (2012). 128.Couper KN, Barnes T, Hafalla JC et al. Parasite-derived plasma microparticles contribute significantly to malaria infection-induced inflammation through potent macrophage stimulation. PLoS. Pathog. 6(1), e1000744 (2010). 129.Mantel PY, Hoang AN, Goldowitz I et al. Malaria-infected erythrocyte-derived microvesicles mediate cellular communication within the parasite population and with the host immune system. Cell Host. Microbe 13(5), 521534 (2013). 130.Rank A, Nieuwland R, Delker R et al. Cellular origin of platelet-derived microparticles in vivo. Thromb. Res. 126(4), e255-e259 (2010). 131. Flaumenhaft R, Dilks JR, Richardson J et al. Megakaryocyte-derived microparticles: direct visualization and distinction from platelet-derived microparticles. Blood 113(5), 1112-1121 (2009). 132.Sinauridze EI, Kireev DA, Popenko NY et al. Platelet microparticle membranes have 50- to 100-fold higher specific procoagulant activity than activated platelets. Thromb. Haemost. 97(3), 425-434 (2007). 133.Merten M, Pakala R, Thiagarajan P, Benedict CR. Platelet microparticles promote platelet interaction with subendothelial matrix in a glycoprotein IIb/IIIa-dependent mechanism. Circulation 99(19), 2577-2582 (1999). 134.Aatonen M, Gronholm M, Siljander PR. Platelet-derived microvesicles: multitalented participants in intercellular communication. Semin. Thromb. Hemost. 38(1), 102-113 (2012). 227 135.Mause SF, Ritzel E, Liehn EA et al. Platelet microparticles enhance the vasoregenerative potential of angiogenic early outgrowth cells after vascular injury. Circulation 122(5), 495-506 (2010). 136.Prokopi M, Pula G, Mayr U et al. Proteomic analysis reveals presence of platelet microparticles in endothelial progenitor cell cultures. Blood 114(3), 723-732 (2009). 137.Forlow SB, McEver RP, Nollert MU. Leukocyte-leukocyte interactions mediated by platelet microparticles under flow. Blood 95(4), 1317-1323 (2000). 138.Boilard E, Nigrovic PA, Larabee K et al. Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science 327(5965), 580-583 (2010). 139.Cauwenberghs S, Feijge MA, Harper AG, Sage SO, Curvers J, Heemskerk JW. Shedding of procoagulant microparticles from unstimulated platelets by integrinmediated destabilization of actin cytoskeleton. FEBS Lett. 580(22), 5313-5320 (2006). 140.Sadallah S, Eken C, Schifferli JA. Erythrocyte-derived ectosomes have immunosuppressive properties. J. Leukoc. Biol. 84(5), 1316-1325 (2008). 141.Baumgartner JM, Silliman CC, Moore EE, Banerjee A, McCarter MD. Stored red blood cell transfusion induces regulatory T cells. J. Am. Coll. Surg. 208(1), 110-119 (2009). 142.Donadee C, Raat NJ, Kanias T et al. Nitric oxide scavenging by red blood cell microparticles and cell-free hemoglobin as a mechanism for the red cell storage lesion. Circulation 124(4), 465-476 (2011). 143.Morrell CN. Immunomodulatory mediators in platelet transfusion reactions. Hematology. Am. Soc. Hematol. Educ. Program. 2011 470-474 (2011). 144.Dinkla S, Novotny VM, Joosten I, Bosman GJ. Storageinduced changes in erythrocyte membrane proteins promote recognition by autoantibodies. PLoS. One. 7(8), e42250 (2012). 145.Belizaire RM, Prakash PS, Richter JR et al. Microparticles from stored red blood cells activate neutrophils and cause lung injury after hemorrhage and resuscitation. J. Am. Coll. Surg. 214(4), 648-655 (2012). 146.Muszynski J, Nateri J, Nicol K, Greathouse K, Hanson L, Hall M. Immunosuppressive effects of red blood cells on monocytes are related to both storage time and storage solution. Transfusion 52(4), 794-802 (2012). 147.Vlaar AP, Hofstra JJ, Levi M et al. Supernatant of aged erythrocytes causes lung inflammation and coagulopathy in a "two-hit" in vivo syngeneic transfusion model. Anesthesiology 113(1), 92-103 (2010). 148.Young PP, Uzieblo A, Trulock E, Lublin DM, Goodnough LT. Autoantibody formation after alloimmunization: are blood transfusions a risk factor for autoimmune hemolytic anemia? Transfusion 44(1), 67-72 (2004). 149. Flad HD, Brandt E. Platelet-derived chemokines: pathophysiology and therapeutic aspects. Cell Mol. Life Sci. 67(14), 2363-2386 (2010). 150.Li N. Platelet-lymphocyte cross-talk. J. Leukoc. Biol. 83(5), 1069-1078 (2008). 151.Nomura S, Okamae F, Abe M et al. Platelets expressing P-selectin and platelet-derived microparticles in stored platelet concentrates bind to PSGL-1 on filtrated leukocytes. Clin. Appl. Thromb. Hemost. 6(4), 213-221 (2000). 152.Refaai MA, Phipps RP, Spinelli SL, Blumberg N. Platelet transfusions: impact on hemostasis, thrombosis, inflammation and clinical outcomes. Thromb. Res. 127(4), 287-291 (2011). 153.Vlaar AP, Hofstra JJ, Kulik W et al. Supernatant of stored platelets causes lung inflammation and coagulopathy in a novel in vivo transfusion model. Blood 116(8), 1360-1368 (2010). 154.Sprague DL, Elzey BD, Crist SA, Waldschmidt TJ, Jensen RJ, Ratliff TL. Platelet-mediated modulation of adaptive immunity: unique delivery of CD154 signal by platelet-derived membrane vesicles. Blood 111(10), 5028-5036 (2008). 155.Garcia BA, Smalley DM, Cho H, Shabanowitz J, Ley K, Hunt DF. The platelet microparticle proteome. J. Proteome. Res. 4(5), 1516-1521 (2005). 228 156.Rank A, Nieuwland R, Liebhardt S et al. Apheresis platelet concentrates contain platelet-derived and endothelial cellderived microparticles. Vox Sang. 100(2), 179-186 (2011). 157.Parham P. The Immune System. 3rd ed. Garland Science; 2009. 158.Kumar V, Abbas AK, Aster J. Inflammation and Repair. In: Robbins Basic Pathology (Volume 9th). Elsevier, (2013). 159.Gawaz M, Langer H, May AE. Platelets in inflammation and atherogenesis. J. Clin. Invest 115(12), 3378-3384 (2005). 160.Semple JW, Italiano JE, Jr., Freedman J. Platelets and the immune continuum. Nat. Rev. Immunol. 11(4), 264-274 (2011). 161. Murray PJ, Wynn TA. Protective and pathogenic functions of macrophage subsets. Nat. Rev. Immunol. 11(11), 723737 (2011). 162.Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat. Immunol. 11(10), 889-896 (2010). 163.Savage ND, de Boer T, Walburg KV et al. Human antiinflammatory macrophages induce Foxp3+ GITR+ CD25+ regulatory T cells, which suppress via membranebound TGFbeta-1. J. Immunol. 181(3), 2220-2226 (2008). 164.Curiel TJ, Coukos G, Zou L et al. Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nat. Med. 10(9), 942-949 (2004). 165.Sakaguchi S, Miyara M, Costantino CM, Hafler DA. FOXP3+ regulatory T cells in the human immune system. Nat. Rev. Immunol. 10(7), 490-500 (2010). 166.Josefowicz SZ, Lu LF, Rudensky AY. Regulatory T cells: mechanisms of differentiation and function. Annu. Rev. Immunol. 30 531-564 (2012). 167.Chaudhry A, Rudra D, Treuting P et al. CD4+ regulatory T cells control TH17 responses in a Stat3-dependent manner. Science 326(5955), 986-991 (2009). 168.Chung Y, Tanaka S, Chu F et al. Follicular regulatory T cells expressing Foxp3 and Bcl-6 suppress germinal center reactions. Nat. Med. 17(8), 983-988 (2011). 169.Koch MA, Tucker-Heard G, Perdue NR, Killebrew JR, Urdahl KB, Campbell DJ. The transcription factor T-bet controls regulatory T cell homeostasis and function during type 1 inflammation. Nat. Immunol. 10(6), 595-602 (2009). 170.Linterman MA, Pierson W, Lee SK et al. Foxp3+ follicular regulatory T cells control the germinal center response. Nat. Med. 17(8), 975-982 (2011). 171.Burzyn D, Benoist C, Mathis D. Regulatory T cells in nonlymphoid tissues. Nat. Immunol. 14(10), 1007-1013 (2013). 172.Tiemessen MM, Jagger AL, Evans HG, van Herwijnen MJ, John S, Taams LS. CD4+CD25+Foxp3+ regulatory T cells induce alternative activation of human monocytes/ macrophages. Proc. Natl. Acad. Sci. U. S. A 104(49), 19446-19451 (2007). 173.Tang Q, Bluestone JA. The Foxp3+ regulatory T cell: a jack of all trades, master of regulation. Nat. Immunol. 9(3), 239-244 (2008). 174.Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound. Repair Regen. 16(5), 585-601 (2008). 175.Burzyn D, Kuswanto W, Kolodin D et al. A special population of regulatory T cells potentiates muscle repair. Cell 155(6), 1282-1295 (2013). 176.Barron L, Wynn TA. Fibrosis is regulated by Th2 and Th17 responses and by dynamic interactions between fibroblasts and macrophages. Am. J. Physiol Gastrointest. Liver Physiol 300(5), G723-G728 (2011). 177.Atabai K, Jame S, Azhar N et al. Mfge8 diminishes the severity of tissue fibrosis in mice by binding and targeting collagen for uptake by macrophages. J. Clin. Invest 119(12), 3713-3722 (2009). 178.Wynn TA. Cellular and molecular mechanisms of fibrosis. J. Pathol. 214(2), 199-210 (2008). Ned Tijdschr Klin Chem Labgeneesk 2016, vol. 41, no. 3