Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
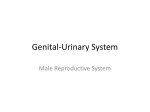
1966 Assessment of 54 Biomarkers for Biopsy-Detectable Prostate Cancer Dipen J. Parekh,1 Donna Pauler Ankerst,1 Jacques Baillargeon,2 Betsy Higgins,1 Elizabeth A. Platz,3 Dean Troyer,5 Javier Hernandez,6 Robin J. Leach,1,4 Anna Lokshin,7 and Ian M. Thompson1 Departments of 1Urology, 2Pathology, and 3Cellular and Structural Biology, University of Texas Health Science Center, and 4Brooke Army Medical Center, San Antonio, Texas; 5Department of Preventive Medicine and Community Health, University of Texas Medical Branch, Galveston, Texas; 6Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; and 7University of Pittsburgh Cancer Center, Pittsburgh, Pennsylvania Abstract Objective: We analyzed the association of 54 biomarkers from seven classes including adipokines, immune response metalloproteinases, adhesion molecules, and growth factors with prostate cancer risk adjusting for the Prostate Cancer Prevention Trial (PCPT) risk score. Methods: A total of 123 incident prostate cancer cases and 127 age-matched controls were selected from subjects in the San Antonio Center for Biomarkers of Risk of Prostate Cancer cohort study. Prediagnostic serum concentrations were measured in the sample collected at baseline using LabMAP technology. The odds ratios (OR) of prostate cancer risk associated with serum concentrations of 54 markers were estimated using univariate conditional logistic regression before and after adjustment for the PCPT risk score. Two-way hierarchical unsupervised clustering techniques were used to evaluate whether the 54-marker panel distinguished cases from controls. Results: Vascular endothelial growth factor, resistin, interleukin 1Ra (IL-1Ra), granulocyte colony-stimulating factor, matrix metalloproteinase-3, plasminogen activator inhibitor, and kallikrein-8 were statistically significantly (P < 0.05) underexpressed in prostate cancer cases, and A-fetoprotein was statistically significantly overexpressed in prostate cancer cases, but all had area underneath the receiver-operating characteristic curve <60%; none were statistically significant adjusting for multiple comparisons (P < 0.0008) or after adjustment for the PCPT risk score. Statistical clustering of patients by the marker panel did not distinguish a separate group of cases from controls. Conclusions: This age-matched case-control study did not support findings of increased diagnostic potential from a 54-marker panel when compared with the conventional risk factors incorporated in the PCPT risk calculator. Future discovery of new biomarkers should always be tested and compared against conventional risk factors before applying them in clinical practice. (Cancer Epidemiol Biomarkers Prev 2007;16(10):1966 – 72) Introduction The pathogenesis of prostate cancer is complex and likely multifactorial. Several etiologic factors have been proposed involving a broad range of molecular systems, pathways, and mechanisms. Adipokines, markers of immune response, metalloproteinases, adhesion molecules, hormones, and several growth factors have been implicated in the process of both cancer initiation and progression in the prostate as well as in other organ systems (1-10). Several from these groups have been proposed as biomarkers for cancer detection as well as for prognosis and follow-up in prostate cancer based on their detection in different biospecimens (10-13). The rapid evaluation of panels of biologically motivated markers for prostate cancer is critical for the development of promising markers for early detection. Prostatespecific antigen (PSA) is currently the most widely used marker for the early detection of prostate cancer. It is Received 4/4/07; revised 6/2/07; accepted 7/11/07. Requests for reprints: Dipen Parekh, Department of Urology, University of Texas Health Sciences Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78284-7802. Phone: 210-567-5640; Fax: 210-567-6868. E-mail: [email protected] Copyright D 2007 American Association for Cancer Research. doi:10.1158/1055-9965.EPI-07-0302 important in the initial phases of biomarker development to compare against this current gold standard. It has been recently shown that other risk factors contribute to PSA for early detection of prostate cancer of high-grade disease, including digital rectal exam (DRE), family history (positive if brother, father, or son had prostate cancer), race (African Americans versus other), age, and history of a prior negative prostate biopsy. These variables are integrated in the form of a risk score that acts as a weighted average of the most prominent risk factors and is more efficient than adding several risk factors (14). For early evaluation of biomarkers, it is also worthwhile to ensure adjustment for these effects in the analysis and as well as to compare the effect of the new markers against these as a benchmark comparison. Case-control studies provide the most efficient mechanism for evaluating large panels of markers as they ensure representative numbers of cases. The purpose of this investigation was to examine the association of a panel of 54 markers with prostate cancer risk in a nested age-matched case control study of 123 cases and 127 controls in the San Antonio Center for Biomarkers of Risk of Prostate Cancer (SABOR) study cohort. The panel includes adipokine markers of immune Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention response, metalloproteinases, adhesion molecules, hormones, growth factors, tumor markers, and other independent molecules not classified as yet under any specific group. This cohort has the advantage that measures of PSA (measured within 1 year of the serum draw for this analysis), family history, age, race, DRE finding, and history of a prior biopsy are available on these men for diagnostic comparison of the new markers. Materials and Methods Study Population. We identified incident prostate cancer cases and controls from members of the SABOR study cohort. SABOR is a prospective screening cohort of f3,500 men from San Antonio and South Texas. This cohort is an effort of the San Antonio Clinical and Epidemiologic Center of the Early Detection Research Network and is supported by the National Cancer Institute. Recruitment of a multiethnic population-based sample was achieved using outreach clinics throughout South Texas. Healthy men, without a history of prostate cancer, were eligible for participation. Participant enrollment began in March 2001 with annual follow-up examinations. A concerted effort was made to oversample ethnic minorities and medically underserved populations. After informed consent, men completed an extensive series of instruments (demographics, diet, quality of life, family history, ethnicity/race, American Urological Association symptom score), provided biological samples, and underwent a directed physical examination including DRE, height, weight, and anthropometric measures. Serum was collected and stored at the University of Texas Health Sciences Center at San Antonio on all SABOR participants at baseline. Blood sample tubes for serum micronutrient and lipid analyses were collected. Clotted blood was processed in a refrigerated centrifuge, and serum was stored at 70jC. At each annual visit, a brief survey is taken of medical problems, and whether prostate cancer had been diagnosed since the time of the last visit. Thereafter, participants underwent phlebotomy and a DRE. If DRE was abnormal or PSA exceeded 2.5 ng/mL, a prostate biopsy was recommended. After 2004, subjects were provided with information related to prostate cancer risk by level of PSA (15) All prostate cancer cases were reviewed by a central pathologist. A total of 123 prostate cancer cases were diagnosed subsequent to enrollment in the cohort. For each case, one control was sampled from the cohort using incidence density sampling (16) to ensure that age-matched controls had accrued at least the same amount of follow-up time as the matched cases at their time of diagnosis. Marker Assessment. All serum samples were assessed using the LabMAP technology (Luminex), which combines the principal of sandwich immunoassay with the fluorescent-bead – based technology allowing individual and multiplex analysis of up to 100 different analytes in a single microtiter well as reported previously (17). Statistical Methods. Conditional logistic regression was used to estimate the odds ratio (OR) of prostate cancer risk by 2-fold change of each biomarker (biomarker on log2 scale), as well as for the conventional risk factors PSA (log2 scale), DRE (abnormal versus normal), family history of prostate cancer (positive versus negative), effect of a prior biopsy (ever versus never), race (African American versus not), and the Prostate Cancer Prevention Trial (PCPT) risk score (log2 scale; ref. 14). Areas underneath the receiver-operating characteristic curve (AUCs) of individual markers, SDs, and tests of the null hypothesis of no diagnostic potential (H0/AUC = 50%) were calculated using U statistics (18). Individual markers were evaluated for independent diagnostic information after adjustment for the PCPT risk score by multivariable logistic regression including the marker and PCPT risk score and similarly adjusting for PSA. In multivariable models where the individual marker retained statistical significance at the 0.05 level after adjusting for PSA or the PCPT risk score, the expected cross-validation predictive capability of the multivariable model was compared with the model containing only PSA or the PCPT risk score using the Bayesian information criterion (BIC). The BIC equals 2 log likelihood + the number of parameters in the model logarithm of the sample size, and models with smaller BIC have better expected predictive performance than models with larger BIC. Two-way unsupervised hierarchical clustering of patients and markers was done to assess whether Table 1. Participant characteristics Controls (n = 127) Mean age (SD) Race/ethnicity Caucasian African American Hispanic Other Median PSA (range) Mean PSA (95% CI) Family history of PCA No Yes Digital rectal exam Normal Abnormal Not done Prior biopsy done Never One or more 61.4 (7.4) 88 13 25 1 1.1 1.1 (69.3%) (10.2%) (19.7%) (0.8%) (0.2, 8.3) (0.2, 5.7) P Cases (n = 123) 63.0 (7.4) 71 21 31 0 3.1 3.0 (57.7%) (17.1%) (25.2%) (0.0%) (0.2, 766.0) (0.5, 19.6) 0.10 0.15 <0.0001 0.66 94 (74.0%) 33 (26.0%) 87 (70.7%) 36 (29.3%) 120 (94.5%) 6 (4.7%) 1 (0.0%) 100 (81.3%) 21 (17.1%) 2 (1.6%) 98 (77.2%) 29 (22.8%) 106 (86.2%) 17 (13.8%) 0.003 0.09 Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. 1967 1968 Evaluation of Markers for Prostate Cancer subgroups of patients had similar marker profiles as well as whether subgroups of markers expressed similar expression levels (19). Clustering was done using agglomerative complete linkage after rank transformation using 50 markers that were expressed above the detection limit in 75% or more of participants. Clusters of patients were matched against case/control status to determine whether cancer cases clustered together, and clusters of markers were matched against predefined biological subgroups to determine whether observed statistical correlations among markers corresponded to biologically hypothesized ones. Correlations between pairs of individual markers and tests of whether the correlations were significantly different from 0 (no correlation) were based on the Spearman rank test statistic. All statistical analyses were done in the R freeware statistical package [R 2.2.1 A Language and Environment, Copyright 2005]. For the AUC and univariate logistic regression tests done on each of the 54 biomarkers and six established risk factors, Bonferroniadjusted two-sided a levels = 0.0008 (0.05/60) were used to account for multiple comparisons. Statistical comparisons of patient characteristics were done using twosample t tests (age, logarithm of PSA) and by m2 tests (race/ethnicity, family history, DRE, prior biopsy) and were done at the two-sided 0.05 level. Results Characteristics of the 123 prostate cancer cases and 127 age-matched controls are shown in Table 1. As to be expected, cases had a statistically significantly higher PSA value on average [mean = 3.0 ng/mL; 95% confidence interval (95% CI)= 0.5 to 19.6 ng/mL] than controls (mean = 1.1 ng/mL; 95% CI = 0.2 to 5.7 ng/mL) and were more likely to have an abnormal DRE. Fewer cases (13.8%) than controls (22.8%) reported having a prior prostate biopsy, although the result was not statistically significant. Results from the logistic regressions and AUCs for the 54 markers in comparison to the standard risk factors are shown in Table 2. Vascular endothelial growth factor (VEGF), resistin, granulocyte colony-stimulating factor (G-CSF), interleukin 1Ra (IL-1Ra), matrix metalloproteinase-3 (MMP-3), plasminogen activator inhibitor-1 (PAI-1), and kallikrein-8 were underexpressed in prostate cancer cases (P < 0.05), and a-fetoprotein (AFP) was overexpressed in prostate cancer cases (P < 0.05). However, none of these markers had a significant effect on prostate cancer in terms of the ORs or AUCs adjusted for the high number of multiple comparisons (all P values >0.0008). None of the AUCs exceeded 60%. In contrast, the conventional risk factors PSA and DRE, and the composite PCPT risk score were highly statistically significant (P < 0.0001), and PSA (AUC = 80.4%) and the PCPT risk score (AUC = 84.9%) had AUCs 20% higher than any of the markers. None of the individual markers were statistically significant (all P values >0.05) after adjusting for the PCPT risk score in a multivariable logistic regression, whereas the PCPT risk score retained its statistical significance (P > 0.0001), and the magnitude of its OR for a doubling of risk in each of the adjusted models (all ORs >6.30 per doubling of risk except for one at 5.58 when adjusting for G-CSF). Similar results were obtained when performing multivariable logistic regression of individual markers adjusting for PSA. PSA remained highly statistically significant in each of these models (all P values <0.0001). Only adiponectin was statistically significant (P = 0.04) at the 0.05 level after adjusting for PSA, a marker that had not been statistically significant at the 0.05 level alone. However, the BIC measure of predictive performance for the combined model of adiponectin and PSA (BIC = 112.04) indicated worse predictive performance (higher BIC) than the model containing PSA alone (BIC = 110.94). An exploratory analysis comprising unsupervised clustering of patients and markers (Fig. 1) revealed that the 54-marker panel could not distinguish cases from controls. Cases and controls did not cluster together as seen on the left side of the graph, where each hierarchical cluster of patients comprised both cases and controls. There was a hotspot of primarily controls with overexpression of a subgroup of markers on the far right, but these markers fell across a range of the classes. Finally there was no to only weak evidence that unsupervised clustering separated markers of different classes. A group of the tumor markers seemed to cluster together (middle of row of marker classes at top). The combined evidence shows that this panel of 54 markers provides only weak diagnostic information for prostate cancer that is highly outweighed by the conventional prognostic factors of PSA and DRE and the PCPT risk score. With this in mind, we sought to characterize the correlations between markers of the same biological class collapsed over cases and controls, along with their correlations with PSA. Adipokines. As indicated by the unsupervised clustering, this group of biomarkers did not correlate well with each other. Of all pairs of the seven markers in this group, only correlations between tumor necrosis factor-RI (TNF-RI) and TNF-RII (correlation r = 0.43) and TNFa and VEGF (r = 0.39) were statistically significant (both P < 0.0001). All other correlations were <0.23, and only five other pairs were statistically significant at the 0.05 level. None of these markers showed strong correlation with PSA (median r = 0.03; range, 1.00 to 0.09). Immune Response. The 12 markers in the immune response group clustered in groups of two or three (Fig. 1), and several pairs exhibited correlations >30% (all P values < 0.0001). IL-1Ra correlated with IL-6 (r = 0.47), IL-2R (0.37), G-CSF (0.52), and macrophage inflammatory protein-1 (MIP-1; 0.47). In addition to IL-1Ra, IL-6 correlated with IL-2R (0.42), G-CSF (0.58), and MIP-1 (0.59). In addition to IL-1Ra and IL-6, IL-2R correlated with MIF (0.42), MPO (0.55), and MIP-1 (0.60). In addition to IL-1Ra and IL6, G-CSF correlated with MIP-1 (0.45) and IP-10 (0.32). Finally, in addition, MIF and MPO correlated (0.36). None of these markers showed strong correlation with PSA (median r = 0.005; range, 0.16 to 0.12). Metalloproteinases. The five markers in the metalloproteinases group all fell within a larger subcluster (right-hand side of dendogram in Fig. 1), but only two pairs exhibited statistically significant correlation (P < 0.0001): MMP and MMP-1 (0.33) and tPAI 1 and PAI-1 (0.68). All other pairs of markers in this group had Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 2. Marker associations with prostate cancer in comparison to the standard risk factors, including the composite PCPT risk score Marker OR (P) (1) Adipokines TNF-RI TNF-RII Leptin TNFa VEGF Adiponectin Resistin (2) Immune response IL-2R sIL-6R MIF IL IL-6 G-CSF IL-1Ra MPO MIP-1 MCP-1a sE-Selectin IP-10 (3) Metalloproteinases MMP-2 MMP-3 MMP-9 PAI-1 (active) tPAI-1 (4) Adhesion SVCAM-1 SICAM-1 (5) Hormones, growth factors FSH LH Prolactin TSH Adrenocorticorticotropic hormone GH IGFBP-1 (6) Tumor markers HCG AFP aKallikrein_10 Carcinoembryonic antigen CA-125 CA 15-3 CA 19-9 CA 72_4 Kallikrein_8 Mesothelin (7) Growth and tumor markers EGFR EGF TGFa HGF NGF ErbB2 Other FAS_L Fractalkine EOTAXIN Cytokeratin_19 Fas Standard risk factors PSA Abnormal DRE Positive family history Previous biopsy African American PCPT risk AUC, % (P) 0.84 0.81 0.88 1.02 0.89 0.76 0.82 (0.56) (0.36) (0.16) (0.83) (0.15) (0.12) (0.10) 55.0 52.6 55.5 50.2 57.9 52.5 56.3 (0.09) (0.24) (0.07) (0.48) (0.01) (0.25) (0.04) 0.95 0.92 1.03 1.12 0.94 0.94 0.91 0.95 0.95 0.86 1.12 0.90 (0.26) (0.63) (0.78) (0.34) (0.03) (0.02) (0.16) (0.58) (0.34) (0.40) (0.53) (0.49) 53.3 53.4 52.3 52.3 55.7 59.4 56.9 53.9 54.6 50.1 53.0 52.5 (0.18) (0.17) (0.26) (0.26) (0.06) (0.005) (0.03) (0.15) (0.10) (0.49) (0.21) (0.25) 0.93 0.68 1.21 0.81 0.60 (0.65) (0.37) (0.37) (0.03) (0.09) 53.9 58.3 51.0 58.1 54.5 (0.15) (0.01) (0.39) (0.01) (0.11) 0.59 (0.16) 1.19 (0.50) 54.9 (0.09) 53.6 (0.16) 1.17 1.02 1.08 0.81 0.99 1.05 1.04 53.6 51.4 54.6 55.5 51.7 54.2 52.1 (0.31) (0.89) (0.55) (0.18) (0.67) (0.30) (0.59) (0.16) (0.35) (0.10) (0.07) (0.32) (0.12) (0.28) NA 1.55 (0.04) 1.08 (0.35) 0.90 (0.12) 0.95 (0.21) 1.00 (1.00) 1.07 (0.71) NA 0.57 (0.02) 0.98 (0.81) NA 57.5 (0.02) 52.5 (0.25) 54.9 (0.09) 51.6 (0.33) 53.2 (0.19) 54.6 (0.10) NA 57.3 (0.02) 51.8 (0.31) 0.65 1.00 0.98 0.94 1.00 0.97 54.9 52.5 53.3 52.1 50.5 52.8 (0.34) (0.97) (0.36) (0.60) (0.86) (0.92) (0.09) (0.25) (0.18) (0.28) (0.45) (0.22) +/ + + + + + + + + + + + NA + + + NA + NA 0.98 (0.40) 0.88 (0.22) NA 1.14 (0.41) NA 52.7 (0.19) 54.3 (0.12) NA 50.4 (0.46) 2.74 5.0 1.24 0.55 1.58 6.51 80.4 (<0.0001) + 84.9 (<0.0001) + (<0.0001) (0.003) (0.48) (0.07) (0.21) (<0.0001) NA + NA + NOTE: OR is odds ratio for cancer for marker greater than the median value of controls versus not; + means marker overexpressed in cancer cases, and means underexpressed according to the AUC; P value for AUC is for a test of the null hypothesis AUC = 50% (random) versus AUC > 50%. Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. 1969 1970 Evaluation of Markers for Prostate Cancer correlations <0.14. None of these markers showed strong correlation with PSA (median r = 0.09; range, 0.12 to 0.04). Adhesion. There were only two adhesion markers, and they clustered together on the heat map (Fig. 1) with correlation 0.39 (P < 0.0001). None of these markers showed strong correlation with PSA (median r = 0.03; range, 0.07 to 0.01). Hormones and Growth Factors. Although a group of four of the seven markers in the hormones and growth factors group clustered together (Fig. 1), only folliclestimulating hormone (FSH) and luteinizing hormone correlated substantially (r = 0.59, P < 0.0001). None of the correlations for any of the other pairs exceeded 0.18. None of these markers showed strong correlation with PSA (median r, 0.00; range, 0.11 to 0.12). Tumor Markers. Of the 10 tumor markers, 5 clustered tightly together, and 2 others close to these (Fig. 1). The correlation matrix for this group of markers is shown in Table 3. Human chorionic gonadotropin (HCG) and CA125 correlated with several other markers in the group, and CA15-3 did not correlate with any other markers. None of these markers showed strong correlation with PSA (median r = 0.06; range, 0.19 to 0.01). Growth and Tumor Markers. The six markers in the growth and tumor markers group did not cluster together (Fig. 1). However, ErbB2 statistically significantly correlated with hepatocyte growth factor (HGF; r = 0.37) and epidermal growth factor receptor (EGFR; r = 0.46), as did transforming growth factor (TGF) with nerve growth factor (NGF; r = 0.43) and EGF (r = 0.32; all P values <0.0001). None of these markers showed strong correlation with PSA (median r = 0.04; range, 0.07 to 0.00). Discussion The use of PSA as a biomarker has significantly impacted the detection and management of prostate cancer during the past decade. Despite its widespread use, PSA testing is associated with several limitations as a screening tool that are well recognized. Several individual biomarkers have been tested in different biospecimens such as serum, plasma, prostate tissue, seminal fluid, and urine to either replace or augment the existing use of PSA in cancer detection and prognosis. Previous studies have evaluated either individual biomarkers or a group of biomarkers belonging to a single family based on structure or function in the diagnosis of prostate cancer as well as for risk stratification and prognosis. The current study is the first, to our knowledge, to evaluate a large number (54) of biomarkers covering a broad spectrum of biological activity in a case control fashion using a uniform, standardized technology for prostate cancer. VEGF underexpression was associated with a higher risk of prostate cancer in our study. This is in contrast to earlier reports that reported a direct association between VEGF overexpression and risk of developing biochemical recurrence, lymph node metastases and distant metastases in patients with prostate cancer (8, 20). This variability can be explained by the significant difference in the patient populations in the two studies. Cases of prostate cancer in the current study were from within a screening cohort with a preoperative median PSA levels of 3.1, whereas previously reported VEGF overexpression was found in unscreened patient population with median PSA levels of 7.3 and more advanced disease (8). It is conceivable that a range of expression (both under and overexpression) of VEGF may be involved as the disease progresses from the precancerous to the locally confined to the more advanced stages. Human Figure 1. Heat map clustering of several classes of biomarkers between cases and controls. Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. Cancer Epidemiology, Biomarkers & Prevention Table 3. Correlation between each pair of markers in the tumor markers group (group 6 of Table 1) HCG aCa_72 aAFP aKallikrein_10 aMesothelin CEA CA_19-9 Kallikrein_8 CA125 CA15-3 HCG aCa_72 aAFP Kall10 Mes CEA CA199 Kall8 CA125 CA15-3 1 0.08 1 0.06 0.06 1 0.38 0.12 0.15 1 0.11 0.05 0.04 0.11 1 0.37 0.16 0.07 0.24 0.09 1 0.25 0.16 0.01 0.18 0.16 0.35 1 0.38 0.18 0.04 0.44 0.13 0.42 0.18 1 0.25 0.16 0.06 0.34 0.02 0.36 0.27 0.31 1 0.02 0.10 0.01 0.00 0.02 0.01 0.01 0.03 0.02 1 NOTE: Correlations in bold are statistically significant at the 0.05 level, and of these, all correlations z0.25 were also significant at 0.0001. kallikrein-8 underexpression was also associated with increased risk of prostate cancer in the present study. The role of other members of the kallikrein family such as PSA and human kallikrein-2 have been extensively studied in different stages of prostate cancer in the past (21). Although kallikrein-8 has recently been advocated as a promising biomarker in ovarian cancer, it has not been evaluated, to our knowledge, in prostate cancer (22). Further studies need to be done evaluating kallikrein-8 expression in biospecimens in patients with different stages of prostate cancer to validate the results of our study. Although a limitation of our study compared with others could be the small sample size, the strong statistical significance maintained for the established risk factors, PSA and DRE, lends evidence that a small sample size was not the underlying reason for the low or lack of statistical significance of this panel of 54 markers on univariate or multivariate analyses adjusting for the PCPT risk score. Several studies have evaluated different classes of biomarkers individually in prostate cancer (2, 6, 8). The current study is unique in that multiple classes of biomarkers were tested using a uniform, standardized technique, facilitating comparisons among different classes of biomarkers, thus reducing technical or temporal errors. One of the major limitations in accepting new prostate cancer biomarkers is the lack of direct comparison to the conventional risk factors for prostate cancer. Although some studies have compared newly tested biomarkers only to PSA for prostate cancer detection, there have been no head-to-head comparison between new biomarkers and a panel of conventional risk factors, which, besides PSA, include other variables such as DRE, family history of prostate cancer, prior negative prostate biopsy, age, and race/ethnicity. The PCPT risk calculator, which incorporates the above risk factors, was originally developed from subjects in the PCPT and has since been validated in the SABOR cohort, which forms the cohort for the current study (23). When compared with the PCPT risk calculator as well as PSA, all biomarkers found to be marginally significant on univariate analysis underperformed. The findings of this study suggest that future endeavors in the discovery of new biomarkers for prostate cancer should involve a rigorous comparison to the wellknown conventional risk factors for cancer detection. The finding that none of the individual biomarkers within the same family or group significantly clustered with each other between cases and controls reinforces the fact that the conventional risk factors continue to be the most accurate way of predicting risk of prostate cancer today. References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. Baillargeon J, Rose DP. Obesity, adipokines, and prostate cancer [review]. Int J Oncol 2006;28:737 – 45. Stattin P, Soderberg S, Hallmans G, et al. Leptin is associated with increased prostate cancer risk: a nested case-referent study. J Clin Endocrinol Metab 2001;86:1341 – 5. Shariat SF, Andrews B, Kattan MW, Kim J, Wheeler TM, Slawin KM. Plasma levels of interleukin-6 and its soluble receptor are associated with prostate cancer progression and metastasis. Urology 2001;58: 1008 – 15. Uehara H, Troncoso P, Johnston D, et al. Expression of interleukin-8 gene in radical prostatectomy specimens is associated with advanced pathologic stage. Prostate 2005;64:409. Cardillo MR, Di Silverio F, Gentile V. Quantitative immunohistochemical and in situ hybridization analysis of metalloproteinases in prostate cancer. Anticancer Res 2006;26:973 – 82. Morgia G, Falsaperla M, Malaponte G, et al. Matrix metalloproteinases as diagnostic (MMP-13) and prognostic (MMP-2, MMP-9) markers of prostate cancer. Urol Res 2005;33:44 – 50. Wilson MJ, Sellers RG, Wiehr C, Melamud O, Pei D, Peehl DM. Expression of matrix metalloproteinase-2 and -9 and their inhibitors, tissue inhibitor of metalloproteinase-1 and -2, in primary cultures of human prostatic stromal and epithelial cells. J Cell Physiol 2002;191: 208 – 16. Shariat SF, Anwuri VA, Lamb DJ, Shah NV, Wheeler TM, Slawin KM. Association of preoperative plasma levels of vascular endothelial growth factor and soluble vascular cell adhesion molecule-1 with lymph node status and biochemical progression after radical prostatectomy. J Clin Oncol 2004;22:1655 – 63. Shariat SF, Lamb DJ, Kattan MW, et al. Association of preoperative plasma levels of insulin-like growth factor I and insulin-like growth factor binding proteins-2 and -3 with prostate cancer invasion, progression, and metastasis. J Clin Oncol 2002;20: 833 – 41. Lekas A, Lazaris AC, Deliveliotis C, et al. The expression of hypoxia-inducible factor-1a (HIF-1a) and angiogenesis markers in hyperplastic and malignant prostate tissue. Anticancer Res 2006;26: 2989 – 93. Gann PH, Klein KG, Chatterton RT, et al. Growth factors in expressed prostatic fluid from men with prostate cancer, BPH, clinically normal prostates. Prostate 1999;40:248 – 55. Gho YS, Kim PN, Li HC, Elkin M, Kleinman HK. Stimulation of tumor growth by human soluble intercellular adhesion molecule-1. Cancer Res 2001;61:42537. Soulitzis N, Karyotis I, Delakas D, Spandidos DA. Expression analysis of peptide growth factors VEGF, FGF2, TGFB1, EGF and IGF1 in prostate cancer and benign prostatic hyperplasia. Int J Oncol 2006;29:305 – 14. Thompson IM, Ankerst DP, Chi C, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst 2006;98:529 – 34. Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level < or = 4.0 ng per milliliter. N Engl J Med 2004;350:2239 – 46. Szklo M, Nieto J, Miller M. Epidemiology: beyond the basics. Gaithersburg (MD): Aspen Publishers, Inc.; 2000. Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. 1971 1972 Evaluation of Markers for Prostate Cancer 17. Gorelik E, Landsittel D, Marrangoni A, et al. Multiplexed immunobeadbased cytokine profiling for early detection of ovarian cancer. Cancer Epidemiol Biomarkers Prev 2005;14:981 – 7. 18. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988;44: 837 – 45. 19. Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysis and display of genome-wide expression patterns. Proc Natl Acad Sci U S A 1998;95:14863 – 8. 20. Duque JL, Loughlin KR, Adam RM, Kantoff P, Mazzucchi E, Freeman MR. Measurement of plasma levels of vascular endothelial growth factor in prostate cancer patients: relationship with clinical stage, Gleason score, prostate volume, and serum prostate-specific antigen. Clinics 2006;61:401 – 8. 21. Haese A, Graefen M, Huland H, Lilja H. Prostate-specific antigen and related isoforms in the diagnosis and management of prostate cancer. Curr Urol Rep 2004;5:231 – 40. 22. Borgono CA, Kishi T, Scorilas A, et al. Human kallikrein 8 protein is a favorable prognostic marker in ovarian cancer. Clin Cancer Res 2006; 12:1487 – 93. 23. Parekh DJ, Ankerst DP, Higgins BA, et al. External validation of the Prostate Cancer Prevention Trial risk calculator in a screened population. Urology 2006;68:1152 – 5. Cancer Epidemiol Biomarkers Prev 2007;16(10). October 2007 Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research. 2519 Correction In an article (1) in the October 2007 issue, an author’s affiliation was incorrect and grant information was omitted. The following corrects the error and the omission. Elizabeth Platz6 Department of Epidemiology, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. The authors gratefully acknowledge the Clinical and Epidemiologic and Validation Center of the Early Detection Research Network (NIH grant number U01CA086402) and the San Antonio Cancer Institute, whose generous funding made this work possible. Dipen J. Parekh is supported by UTHSCSA Institute for Integration of Medicine and Science (IIMS) Mentored Career Development Award. Reference 1. Parekh DJ, et al. Assessment of 54 biomarkers for biopsy-detectable prostate cancer. Cancer Epidemiol Biomarkers Prev 2007;16:1966 – 72. Copyright D 2007 American Association for Cancer Research. doi:10.1158/1055-9965.EPI-16-11-COR1 Cancer Epidemiol Biomarkers Prev 2007;16(11). November 2007 Assessment of 54 Biomarkers for Biopsy-Detectable Prostate Cancer Dipen J. Parekh, Donna Pauler Ankerst, Jacques Baillargeon, et al. Cancer Epidemiol Biomarkers Prev 2007;16:1966-1972. Updated version Cited articles Citing articles E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: http://cebp.aacrjournals.org/content/16/10/1966 This article cites 22 articles, 8 of which you can access for free at: http://cebp.aacrjournals.org/content/16/10/1966.full.html#ref-list-1 This article has been cited by 4 HighWire-hosted articles. Access the articles at: /content/16/10/1966.full.html#related-urls Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from cebp.aacrjournals.org on April 20, 2017. © 2007 American Association for Cancer Research.