Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
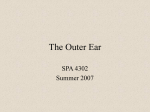
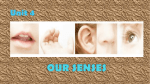
This article originally appeared in The Hearing Profesional July—August 2004 Continuing Education: The Importance of the Keratin Layer to Successful Fitting and Treatment By Max S. Chartrand, BC-HIS IHS offers a diversity of options for obtaining continuing education credit: seminars and classroom training, institutional courses, online studies and distance learning programs. This article represents yet another opportunity. Upon successful completion of the accompanying test you will earn one CEU. The keratin or keratinocyte layer is the outermost portion of the stratum corneum or outer layer of tissues of the external ear canal. Its physiological role is critical in maintaining homeostasis and adapting comfortably to hearing aids and should garner the attention of every member of the hearing healthcare team. Yet, though easily viewed through video otoscopy, its status often goes unnoted during the normal course of dispensing activity. Keratin is comprised of inorganic protein with no circulatory or neurological system. Chemically, its structure is similar to that of human hair and nails. It completely covers the epithelial tissue, starting at a point near the umbo of the tympanic membrane and then traveling the entire length of the canal lumen to the aperture or opening of the ear canal. Keratin protein is the most ignored part of the outer ear, yet it is vital for: maintaining pH flora to prevent fungus, yeast, bacterial infections mixing sebaceous and ceruminous secretions shielding the neuroreflexes from oversensitivity adapting successfully to hearing aid earmolds Figure 1 When the migrating keratin approaches the ear canal opening, it terminates just after contact with tiny hair follicles that grow inward, forming a kind of “ramp” that lifts the desquamated (dead) keratin and its cargo of debris from the epithelium. In turn, minute accumulations of dead skin cells, debris and earwax are steadily deposited into the concha of the ear for easy removal. Through otoscopy, keratin protein presents a “shiny” appearance. As underlying tissue grows steadily and haltingly outward from the tympanic membrane, its migration causes a “bunched up” appearance, forming circular “lines” around the wall of the ear canal. In cases of dehydration or in response to some medications these lines can be so close together as to appear granular. Undisturbed, keratin is what shields the ear canal from bacteria, fungus, yeast, amoeba and potentially septic debris. It also helps the epithelium or outer layer of skin tissue—when coated with ceruminous and sebaceous secretions (that together form “earwax”)—to maintain a slightly acidic pH environment of about 6.5. Hence, keratin is the protective layer over the skin of the ear canal, without which the ear canal would be more susceptible to invasion, injury and/or disease. The absence of keratin in the ear canal may contribute to many common complaints among hearing instrument users, such as: chronic itching hearing aid earmold discomfort non-acoustic occlusion (via the Arnold’s branch of the vagus) predisposition for chronic externa otitis Self-Cleaning Canal The natural desquamation of tissue in the ear canal is such that tissue grows outward from near the umbo (or center point of the eardrum) to the aperture of the ear canal. This natural process generally requires about three months to travel the full length of the canal at the rate of about 1mm per day. So, if one were to place a piece of sand on the tympanic eardrum today, about three months from now that person could remove the same piece of sand from the bowl or concha of the ear with a fingertip. Left undisturbed, then, healthy ear canals are self-cleaning and wax impaction is rare. Abnormally low pH (below 6.5) often leaves the ear canal dry with a host of extant skin problems (psoriasis, eczema, chronic external otitis, contact dermatitis, allergy and abnormal cell growth such as basal and squamous cell carcinomas). After removal via cotton swab trauma or scratching with any foreign object it requires about 10—14 days for a good, strong layer of keratin to reform. Hence, daily use of cotton swabs will effectively negate its formation. In addition, frequent use of ear preparations containing boric acid or hydrogen peroxide solutions not only destroy keratin and layers of epithelium, they also eliminate the water repellent ability of same and leave the external ear canal at risk for chronic otitis externa. Furthermore, these acids can inhibit cerumen formation, as well as interrupt natural desquamation of tissue and the regrowth of the badly needed keratin. Unfortunately, such harsh solutions are the mainstay of today’s over-the-counter otopharmacopia. Figure 2: Keratin coming up off of canal: Latent diabetes II case. As a result of many years of experience working with hearing aid patients, this author believes that only gentle, aseptic botanical solutions should be used in the ears, whether for the purpose of softening hardened earwax or to nurture traumatized ear canal tissues back to normal homeostasis. In so doing, natural tissue growth and its subsequent desquamation will help the canal resume its conveyor belt-like process for self-cleaning and removing potentially harmful debris from the ear canal. Some common and professional practices that remove vital keratin and can set up the external canal for the above problems are: daily use of cotton swabs insertion of foreign objects frequent use of boric acid and hydrogen peroxide solutions aggressive cerumen removal overly tight oto blocks during impression taking forcing one-size-fits-all earmolds into the ear In cases where keratin has been removed due to any of the above described methods or has not formed normally, especially in cases of abnormal pH (diabetes mellitus II, gout or thrush), a host of irritating, potentially dangerous organisms such as fungi (aspergillus favus, etc.), yeasts (candida parapsilosis), pseudomonas aeruginosa (gram positive) and streptococcus areus has been found. Once the offending practices cease, periodic video otoscopic inspection should reveal ear canal homeostasis returning to normal. Simultaneously, if there is not underlying pathology, patient complaints usually subside. If not, medical referral may be indicated. There is so much more to the discussion on keratin. It is often mistaken for earwax and, in cases of chronically low pH, appears to peel off like snake skin as it separates early from underlying epithelium. This is especially observed in cases of undisclosed or latent diabetes mellitus II and hyper/hypoglycemia, a common pre-diabetic mellitus II condition. In our practice, we have also noted the association with long-term semi-dehydration (often accompanied with hypernatremia or hypokalemia) and loss or granulation of the keratin layer. Additionally, a narrowly recognized yet potentially dangerous phenomenon arises when desquamated skin cells mix with accumulated cerumen and peeled off keratin to form bacterial sepsis. Long-term impacted earwax with offending bacteria and/or parasites can dry out and harden the wax. In these cases, gentle softeners are indicated before removal. External Canal Neuroreflexes That May Complicate HA Fittings Neuroreflex Arnold’s branch of the vagus (Cranial X) Lymphatic reflex (Cranial V and VII) Red reflex (tympanic plexus of Cranial VII) Indications During Dispensing Tasks Cough, non-acoustic occlusion, own-voice complaints Increased tightness earmold over time, soreness Induces need for more gain/output in amplification over time Essential for Hearing Instrument Success When it comes to wearing hearing aids, keratin status can be most crucial to success. Very few patients can comfortably adapt to new hearing aids if the ear canal is in an unhealthy state. The essential layer of keratin also shields the wearing of hearing aids and earmolds from the sensitive neural reflexes that arise from compression of myelinated and unmyelinated nerve fibers of Cranials V, VII, IX and X that innervate and traverse the external canal. Unshielded, these sensitive reflexes can cause complications in hearing aid and earmold fittings. Some natural neuroreflexes of the external ear canal, which can become particularly sensitive in the absence of keratin are shown in Figure 3. Such complications are usually resolved by restoring the keratin layer, following instructions for an appropriate wearing schedule, tapering the end of the offending earmold and/or making impressions utilizing the (mid) open-mouth technique. This author thinks that external ear physiology training should always include the importance of keratin protein. It should be noted in all its normal and abnormal forms via video otoscopy and then discussed by all members of the hearing healthcare team. In doing so, we may more effectively reduce unnecessary shell and earmold remakes, returns for credit and failed hearing aid trials. Additionally, we will further enlighten ideas about and approaches to ear care, otoprosthetics and auditory rehabilitation. Best of all, hearing impaired individuals will be more apt to enjoy the benefits of modern hearing technology for improved quality of life, thus inducing a positive attitude about the care and services available from their hearing professional and creating a win-win for all. THP Max Chartrand serves as director of research at DigiCare Hearing Research & Rehabilitation in Rye, Colorado, and has been actively involved in professional training in the hearing healthcare field for more than two and a half decades. Correspondence: www.digicare.org. Bibliography Becker, W., Naumann, H. H., and Pfaltz, C. R., Ear, Nose and Throat Diseases, ed. Buckingham, R. A., New York: Theime Medical Publishers, Inc., pp. 134—136 (1989). Chartrand, M. S., “Basic Course in External Ear Care,” Hearing Library, DigiCare Hearing Research & Rehabilitation: www.digicare.org (2002). Chartrand, M. S., “Video Otoscopy Observation and Referral: The FDA Red Flags,” The Hearing Professional, Jan—Feb, 2003, pp. 9—14 (2003). Chartrand, M. S., “But What’s Wrong with Q-tips®?” Archives, Audiology Online Newsletter: www.audiologyonline.com, January (2003). Davis, W. E., “The external and middle ear,” in Otolaryngology—Head and Neck Surgery: Principles and Concepts, Templar, J., and Dais, W. E., ed., St. Louis: Ishiyaku EuroAmerica, Inc., pp. 34—36 (1987). Habif, T. P., Clinical Dermatology, 2nd edition, St. Louis: C. V. Moy Company, pp. 28—31 (1990). Hawke, M., “Atlas of Clinical Otoscopy,” Modern Medicine of Canada, Vol. 36, No. 3, pp. 303—310, March (1981). Johnson A., and Hawke, M., “The nonauditory physiology of the external ear,” from Physiology of the Ear, eds. A. F., and Santos-Sacchi, J., Raven Press: New York, pp. 41—58 (1988). Kemp, R. J., and Bankaitis, A. E., “Infection control for audiologists,” in Hosford-Dunn H., Roeser, R., and Valente, M., eds. Audiology Diagnosis, Treatment, and Practice Management, Vol. III, New York: Theime Publishing Group (2000). McSpaden, J. B., and McSpaden-Hickock, D. K., and Hickock, R. L., “More than everything you wanted to know about non-acoustic occlusion and venting,” Audecibel, Jan—Mar (1993). Roland, P. S., “Chronic External Otitis,” Ear, Nose & Throat Journal, June Supplement (2001). Sundstrom, J., and Mulligan, K., Neuroanatomy Interactive Syllabus; Ch. 7: Auditory System, University of Washington (2002). Slattery, W. H. III, and Saadat, P., “Postinflammatory medial canal fibrosis,” Am J Otol, 18:294—297 (1997).