Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
BODY FLUID COMPARTMENTS
PHYSIOLOGY III, TRI IV
GUYTON & HALL, CHAPTER 25
Dr. Robyn Strader
OBJECTIVES:
1. To learn the major body fluid compartments and their contents.
2. To learn the approximate volume and location of the fluid compartments.
3. To understand the consequences of osmotic balance and imbalance between the fluid
compartments.
4. To discuss some mechanisms for maintaining osmotic equilibrium.
5. To discuss the development of edema.
I. Total body water
A. approx. 42 liters in 70 kg person
B. 60 - 80% of total body weight
C. affected by age, gender, and obesity
II. Intake versus output
A. intake
1. ingestion
a. food and liquids
b. approx. 2100 ml/day
2. oxidation of hydrogen
a. 150 - 250 ml/day
b. approx. 200 ml/day
3. normal intake = 2300 ml/day
B. output
1. insensible water loss
a. approx. 700 ml/day
b. through the skin
1. 300 - 400 ml/day
2. burn victims can increase water loss by 10X,
approx. 3-5 liter/day
c. respiratory
1. 300-400 ml/day
2. air is moisturized to a vapor pressure of 47 mm Hg in the lungs
3. cold air has vapor pressure of approx. 0 mm Hg
10
2. sensible water loss
a. exercise
1. increased respiration
2. increased sweating
a. depends on exercise intensity
b. range of 100 ml/day to 1-2 liters/day
b. excretion
1. feces - approx. 100 ml/day
2. diarrhea
3. urine
a. multiple mechanisms
b. 0.5 to 20 liter/day possible range
(1-1.5 liter/day is normal average)
Total Body Fluids (~40 Liters)
Extracellular
Volume
(15 liters)
Plasma
Volume
(3 liters)
****
** *
***
***
****
***
***
***
****
*****
(2 liters)
Intracellular
Volume
(25 liters)
Red Cell
Volume
Blood Volume
(5 liters)
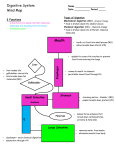
III. Body fluid compartments
A. Intracellular fluid compartment
1. intracellular fluid,
a. approx. 40% of body weight or approx. 25 L
b. approx. 28 L in 70 Kg person
2. similar composition from cell to cell
B. Extracellular fluid (ECF) compartment
1. outside the cells
2. about 15 liters or 20% of body weight
3. divisions:
a. interstitial fluid, approximately 3/4 of ECF
11
b. plasma, almost 1/4 of ECF or 3 liters
c. transcellular fluid, approx. 1- 2 liters
1. cerebrospinal fluid
2. intraocular fluid
3. fluids of the gastrointestinal tract
4. fluids of the potential spaces
C. Blood volume - separate fluid compartment
1. extracellular - plasma
a. approx. 60% of blood volume
b. contains higher concentration of protein than interstitial fluid
c. slightly greater concentration of cations (+)
2. intracellular - fluid in RBC's
3. avg. BV = 5 liters (5 liter = 3 liters plasma + 2 liters of RBC's),
8% of body weight
4. hematocrit = % RBC in blood (packed red cell volume)
a. males = approx. 43 + 5%
b. females = approx. 40 + 5%
c. anemia & polycythemia
D. Measurement of body fluid
1. dilution principle
2. volume in milliliters =
quantity of test substance instilled
concentration per ml of dispersed fluid
12
Known Concentration and Volume
Unknown
Volume
Unknown Volume
Fick's Law
Unknown Volume = Known Volume X Known Concentration
Concentration of Unknown Volume
3. measurement of :
a. total body water
b. extracellular fluid volume
c. calculation of intracellular volume
Intracellular volume = total body water - extracellular volume
d. measurement of plasma volume
e. calculation of interstitial fluid volume
interstitial fluid volume = extracellular fluid volume - plasma volume
f. measurement of blood volume
Total blood volume = Plasma volume
1 - Hematocrit
13
IV. Constituents of extracellular and intracellular fluids
A. major constituents of extracellular fluid
1. large quantities
a. Na
b. Cl
c. bicarbonate ion
d. protein (plasma)
2. small quantities
a. potassium
b. calcium
c. magnesium
d. phosphate
e. sulfate
f. organic acid ions
B. major constituents of intracellular fluid
1. large quantities
a. potassium
b. phosphate
c. magnesium
d. sulfate ions
e. protein; intracellular protein is approx. 4X greater than plasma protein
2. small quantities
a. sodium
b. chloride
c. calcium
V. Osmotic Equilibria and fluid shifts
A. osmosis = movement of solvent toward solutes
B. osmotic pressure = pressure required to oppose osmosis
C. osmotic pressure is proportional to the concentration of the
non-permeant molecules in a solution
D. non-permeant ions cause osmosis and osmotic pressure in the
same manner as does non-permeant molecules
E. osmole = total # of particles in a solution
1. 1 osmole (osm) is equal to 1 mole (mol; 6.02 X 1023)
2. osmole refers to the number of osmotically active particles in a solution
F. osmolality = osmoles / kilogram of water
(This term is most often used by medical labs.)
G. osmolarity = osmoles / liter solution (used most often in clinical data)
H. Osmotic pressure (mmHg) = 19.3 X Osmolality (milliosmole / kg water);
1. amount of pressure required for preventing osmosis
2. indirect measurement of the water and solute concentrations of a solution
3. osmotic pressure is directly proportional to the concentration of osmotically
active particles in solution
14
I. osmolality of body fluids
1. 4/5 of total osmolality of the interstitial fluid and
plasma is caused by sodium and chloride
2. 1/2 of intracellular osmolality is caused by potassium
3. plasma osmolality 1.3 milliosmoles greater than interstitial and
intracellular fluids
VI. Maintenance of osmotic equilibrium
A. isotonicity
B. hypotonicity
C. hypertonicity
Cell
Cell
Isotonic Fluid
Cell
Hypotonic Fluid
Cell
Hypertonic Fluid
VII. Edema
A. edema = presence of excess fluid in the tissues
1. intracellular edema
a. depression of metabolic systems or inadequate nutrition to the cells
b. inflammation
2. extracellular edema
a. abnormal leakage of fluid from the capillaries
1. increased capillary pressure
2. decreased plasma proteins / increased interstitial proteins
3. increased capillary permeability
b. failure of lymphatic system to return fluid
c. renal retention of salt and water
3. proteoglycan meshwork
4. "pitting" vs. "nonpitting" edema
15
B. causes of edema
1. increased capillary pressure
a. excessive kidney retention of salt and water
b. high venous pressure
c. decreased arteriolar resistance
P
Increased Capillary Pressure
2. decreased plasma proteins
a. loss of proteins in urine
b. loss of protein from denuded skin areas
c. failure to produce proteins
pppp
ppppppppp
ppppppppppp
ppppppppp
pppppp
p
p
p
p
p
p
p
p
Decreased Capillary Protein
3. increased capillary permeability
a. immune reactions that cause release of histamine and
other immune products
b. toxins
c. bacterial infections
d. vitamin deficiency, especially vit. C
e. prolong ischemia
f. burns
Increased Capillary Permeability
16
4. blockage of lymph return
a. cancer
b. infections
c. surgery
d. congenital absence or abnormality of lymphatic vessels
Lymph Flow
Blood Flow
Lymph Flow
Blood Flow
Blocked Lymph Flow
VIII. Safety factors that normally prevent edema
A. low compliance of the interstitium when interstitial fluid pressure is in the negative
pressure range
B. ability of lymph flow to increase 10 - 50 fold
C. washdown of interstitial fluid protein concentration
IX. Fluids in the potential spaces
A. fluid exchange
B. lymphatic drainage of protein from the potential spaces potential spaces
C. edema in potential spaces = effusion
17
60
Interstitial
Fluid
Volume
Total Interstitial Fluid
32
28
24
Free Fluid
20
16
12
8
4
Gel Fluid
0
-10 -8 -6 -4 -2 0 2 4 6 8
Interstitial Free Fluid Pressure
18
19
Urine Formation: Renal Blood Flow, Glomerular Filtration, and Their Control
Physiology III, Tri 4
Guyton Chapter 26
Dr. Robyn Strader
OBJECTIVES:
1. To understand the importance of the role of the kidney in urine formation.
2. To understand the structure and function of the nephron.
3. To learn the direction of fluid flow through the kidney.
4. To learn the importance of blood flow and blood pressure in the formation of urine.
5. To understand glomerular filtration rate and the components that effects it.
6. To discuss the mechanisms that regulate blood flow and glomerular filtration rate.
I.
II.
III.
Kidney
A. Excrete most of the end products of body metabolism
B. Control concentrations of body fluid constituents
Nephron
A. Functional unit
B. Forms urine
C. Composed of:
1.
glomerulus (Bowman's capsule and capillaries)
2.
tubule
Fluid Flow
A. afferent arteriole
B. efferent arteriole
C. Bowman's capsule
D. proximal tubule
E. Loop of Henle
1.
descending limb
2.
thin segment
3.
ascending limb
F. distal tubule
G. cortical collecting duct
H. collecting duct
I.
minor calyx
J.
major calyx
K. renal pelvis
L. ureter
20
IV.
V.
VI.
VII.
Capillary Network
A. peritubular capillary network
1.
supplied by efferent arterioles
2.
in renal cortex
3.
next to proximal and distal tubules, and collecting ducts
B. Vasa recta
1.
extensions of peritubular network
2.
extend to medulla with loops of Henle
Nephron Function ("clears" blood)
A. glomerular filtration
B. reabsorption
C. secretion
Renal Blood Flow
A. renal fraction = 1/5 of cardiac output
B. varies from 12-30%
Renal Blood Pressure
A. glomerulus
1.
resistance
2.
high pressure
B. peritubular bed
1.
low resistance
2.
low pressure
C. vasa recta
1.
only 1-2% of renal flow
2.
"sluggish flow"
D. arcuate arteries = 100 mm Hg
E. veins = 8 mm Hg
F. afferent = 100 mm Hg
G. glomerulus = 60 mm Hg
H. efferent arterioles = 47 mm Hg
I.
peritubular capillary = 13 mm Hg
J.
glomerulus
1. pressure
2. filtration
K. capillary bed
1. pressure
2. absorption
L. intrarenal pressure (due to capsule) = 13 mm Hg
M. Peritubular capillaries
1.
extremely porous
2.
rapid absorption
3.
glomeruli filters = 180 l/day; only 1-1.5 becomes urine
21
VIII.
Glomerular Filtration
A. glomerular membrane (very porous)
1.
capillary endothelial cell
2.
basement membrane
3.
epithelial cell
Capillary Endothelial Cell
Basement Membrane
Epithelial Cell
B.
C.
D.
permeable to molecules <69,000 MW
pore size
negative electrical charge
Cationic
Neutral
Anionic
4
Molecular Weight X 10,000
IX.
6
8
Glomerular Filtrate
A. Similar composition to arterial blood except no RBC's and very little protein
B. Rate
1.
125 ml/min
2.
filtration fraction = 19%
125 ml/min glomerular filtration = 19%
650 ml/min plasma flow
CP
glomerular
capillary
GP
Bowman's Capsule
GCP
22
C.
D.
E.
F.
X.
Dynamics of filtration
1. glomerular capillary pressure, filtration
2. Bowman's capsule pressure, filtration
3. plasma protein colloid osmotic pressure, filtration
4. Bowman's capsule protein, filtration
5.
Glomerular pressure (GP) = 60 Hg
6.
Bowman's capsule pressure (CP) = 18 mm Hg
7.
Colloid osmotic pressure in the glomerular(GCP)
capillaries 28-36 mm Hg, X = 32 mm Hg
Filtration pressure
FP = GP - GCP - CP
Filtration coefficient = Kf
Kf = glomerular filtration rate in both kidneys/mm Hg filtration pressure
GFR = filtration pressure X Kf
125 ml/min = 10 mm Hg X 12.5 ml/min/Hg
Factors that affect the GFR
A. Filtration coefficient
B. Glomerular pressure
C. Plasma colloid osmotic pressure
D. Bowman's capsule pressure
E. Renal blood flow
F. Arteriolar constriction
1.
afferent
2.
efferent
23
24
XI.
Control of GFR and Renal Blood Flow
A. Autoregulation
B. Tubuloglomerular feedback
1.
afferent arteriolar vasodilator feedback mechanism
2.
efferent arteriolar vasoconstrictor feedback
mechanism
C. Juxtaglomerular complex
1.
macula densa
2.
juxtaglomerular cells
3.
pressure diuresis
4.
systemic stimulation
5.
reabsorption of fluid by the peritubular capillaries
Glomerular Capillary Bed
Juxtaglomerular Apparatus
Distal
Tubule
25
26
FORMATION OF URINE BY THE KIDNEY
Physiology III, Tri 4
Guyton & Hall, Chapter 27
Dr. Robyn Strader
OBJECTIVES:
1.
2.
3.
4.
5.
6.
To describe the mechanisms for transport into and out of the renal tubule.
To learn the histology of the cells lining the renal tubule.
To discover the cellular differences along the renal tubule.
To learn where absorption and/or secretion occur for selected substances.
To understand the meaning of tubular load.
To be able to calculate plasma clearance.
I.
Active Transport
A. Primary active
1.
ATPase
2.
Concentration gradient
3.
Intracellular potential
4.
Carrier proteins
5.
Secretory transport
6.
Absorptive transport
Interstitium
Lumen
Tubular Cell
K
K
Na
Na
ACTIVE TRANSPORT
Na
B.
Secondary active absorption
1.
No energy from ATP used
2.
Dependent upon Na movement - co-transport
3.
Brush border protein carriers
Co-Transport
Amino Acids, Glucose
27
C.
Secondary active secretion
1.
Counter transport
2.
Brush border carrier protein
Counter Transport
II.
Passive Absorption of Water
A. Concentration difference
B. Tight junctions
III.
Passive Absorption
A. Electrical neutrality
B. Passive diffusion
C. Chloride, ions, urea, creatinine
28
IV. Absorptive Capabilities
A. Proximal Tubular Epithelium
1.
2.
absorbs most (65%) of glomerular filtrate
3.
brush border
4.
extensive interstitial membrane
5.
secondary active transport
a.
absorbed
i.
glucose
ii.
amino acids
b.
secreted - H ions
B.
Thin Segment of the Loop of Henle
1.
thin epithelium
2.
reduced activity
3.
ing portion)
4.
simple diffusion
C.
Thick Segment of the Loop of Henle
1.
thick epithelial cells
2.
ascends back to glomerulus
3.
forms juxtaglomerular complex
4.
rudimentary brush border
5.
few basal channels
6.
tight junctions
7.
active transport of Na & Cl
8.
almost impermeable to H2O and urea
9.
3/4 of all ions transported out
10. important role in urine concentration
D.
Distal Tubule
1.
starts at juxtaglomerular complex
2.
convoluted
3.
functional segments
a.
diluting segment - similar to thick segment
b.
late distal and cortical collecting duct
i.
impermeable to urea
ii.
Na reabsorbed, K secreted
iii.
intercalated cells, H+
iv.
permeability and ADH
E.
Collecting Duct
1.
cuboidal epithelial cells
2.
ADH determines permeability
3.
secretion of H+
29
V.
VI.
Reabsorption of Water
A. osmotic diffusion
B. volume diminishes along tubular path
Reabsorption of Other Substances
A. protein
1.
absorbed through the brush border of proximal tubule
2.
pinocytosis
B. urea - small quantities reabsorbed
C. creatinine - not reabsorbed, only secreted
D. urate ion, sulfates, phosphates, and nitrates - less reabsorption than water
E. inulin and para-aminohippuric acid - used for function studies
VII. Tubular Load = amount of substance that filters through the glomerular membrane into
the tubules each minute.
A.
Tubular transport maximum (Tm) = the maximum rate at which a substance can
be reabsorbed
500
400
Loss of
Glucose
in urine
100
0
*
*
0
B.
*
100 200 300 400
Tubular load of Glucose
500 600
700 800
Gradient - time transport
1.
no transport maximum
2.
dependent on
a.
concentration gradient of substance across the membrane, without
any maximum
b.
the time that the fluid containing the substance remains within the
tubule
VIII. Plasma Clearance
PC ml/min = (Urine Flow ml/min) X (Concentration in Urine)
Concentration in Plasma
30
31
32
33
Renal and Associated Mechanisms for Controlling
Extracellular Fluid Osmolality and Sodium Concentration
Physiology III, Tri 4
Guyton & Hall, Chapter 28
Dr. Robyn Strader
OBJECTIVES:
1. To understand how the body reduces the amount of excess water.
2. To understand how and why the body produces a dilute urine.
3. To understand how the kidney uses the countercurrent mechanism to concentrate urine.
4. To understand the role of ADH in the kidney.
5. To understand the role of aldosterone in maintaining osmolality.
6. To understand the importance of and regulation of sodium concentration.
I.
The Mechanism for Excreting Excess Water: Excretion of a Dilute Urine.
A. Osmolality, Urine body water
B. Osmolality, excretion of solutes
C. with decreased osmolality:
1. increased urine output
2. urine may have osmolarity as low as 50 mosm/liter
3. sodium and potassium concentrations may not be effected
D. Renal mechanism
1.
the kidney has the ability to regulate water excretion independently of
2.
necessary for survival
3.
absorb solutes
4.
distal tubules
II.
The Mechanism for Excreting Excess Solutes: the Countercurrent Mechanism for
Excreting a Concentrated Urine
A. Antidiuretic hormone (ADH) = Vasopressin
1.
posterior pituitary
2.
distal tubule
3.
most powerful feedback system for regulating plasma osmolarity and
B. Counter current mechanism
1.
Juxtamedullary nephrons
2.
Vasa recta
C. Hyperosmolality of the medullary interstitial fluid, and mechanisms for achieving it
1.
osmotic pressure of medullary fluid
a.
active/passive transport of Na+, active transport of Cl- and co-transport
of K, etc. out of the thick portion of the ascending limb
b.
carried downward into inner medulla
c.
active transport of Na from the collecting ducts and passive absorption
of Cl ions with Na ions
34
ADH urea absorbed into the fluid of the inner medulla from
the collecting ducts
e.
medullary interstitial fluid osmolality is due to:
(1)
active transport of the ions into the interstitium by the thick
portion of the ascending limb of loop of Henle
(2)
active transport of ions from the collecting duct into the
interstitium
(3)
passive diffusion of large amounts of urea from the collecting
duct into the interstitium
Water Reabsorption via ADH
1.
ADH acts on basolateral membrane
2.
ADH activates adenyl cyclase in membrane to form cyclic adenosine
monophosphate (cyclic AMP) in the cell membrane
d.
D.
E.
Countercurrent Multiplier = repetitive reabsorption of Na Cl by the thick ascending
segment of the loop of Henle, along with the continual inflow of new NaCl from the
proximal tubule into the loop of Henle
F.
Counter Current Exchange Mechanism in the Vasa Recta - A Mechanism for
Holding Solutes in the Medulla
1.
medullary blood flow maintains high solute concentration in medullary
interstitial fluids
2.
"sluggish" blood flow minimizes solute removal
3.
vasa recta function as a counter current exchanger
G.
Mechanism for Excreting a Concentrated Urine - Role of ADH
1.
increase permeability of cortical collecting duct, collecting duct and distal
tubule
2.
water enters medullary interstitium via osmosis
3.
concentration in collecting duct
H.
Summary of the Osmolal Concentration Changes in the Different Segments of the
Tubules.
1.
proximal tubule - highly permeable to water
2.
Loop of Henle - osmolality rises rapidly due to counter current mechanism
3.
In distal tubule, cortical collecting duct, and collecting duct - osmolality is
dependent on ADH
I.
Osmolar clearance; Free Water Clearance
1.
C osm = Osmoles entering urine per minute
Plasma Osmolar Concentration
2.
Free water = excess water that is excreted
CH2O = Urine volume per minute - C osm
35
III.
Control of Extra Cellular Fluid Osmolality and Sodium Concentration
A. Extracellular fluid osmolality = 300 + 3% mosm/L
Na ion concentration = 142 + 3% mEq/L
B. Relationship between extra cellular fluid osmolality and sodium concentration is
determined almost entirely by the extracellular fluid Na concentration
C. Control systems regulating extracellular osmolality and sodium concentration
1.
osmoreceptor - antidiuretic hormone
2.
thirst mechanism
3.
salt appetite mechanism
IV.
Sodium Excretion and its Control by Aldosterone
A. Role of tubular system is to reabsorb Na
1.
Proximal tubule = 65%
2.
Ascending limb of Loop of Henle = 27%
B.
Variable Reabsorption of Sodium in the late distal tubules and Cortical Collecting
Ducts - Role of Aldosterone
1.
Na excretion in the late distal tubules is dependent on aldosterone
2.
Aldosterone activates the DNA molecule to Form (M) RNA to cause
formation of carrier proteins or protein enzymes necessary for Na transport
process
3.
Stimulation of Aldosterone secretion
a.
Angiotensin II
b.
extracellular fluid potassium ion concentration
c.
extracellular fluid Na ion concentration
V. Control of sodium intake
A. Stimuli
1. decreased sodium concentration in the extracellular fluid
2. circulatory insufficiency
B. Thirst - elicited immediately
C. Salt appetite - progressively builds after several hours
36
37
38
Renal Regulation of Blood Volume and Extracellular Fluid Volume;
Excretion and Regulation of Urea, Potassium, and Other Substances
Physiology III, Tri 4
Guyton Chapter 29 & Micturition (31)
Dr. Robyn Strader
OBJECTIVES:
1. To understand the processes of pressure natriuresis and pressure diuresis.
2. To understand mechanisms for blood volume control.
3. To understand nervous and hormonal factors that contribute to the control of blood volume.
4. To understand conditions that cause large increases in blood volume.
5. To understand mechanisms for excretion of selected substances.
6. To understand the process of micturition.
I.
Control of Blood Volume
A. Constancy of Blood Volume
(Fig.29). Almost no change in blood volume occurs despite tremendous changes
in daily intake of water and electrolytes.
Blood
Volume
5
4
3
2
1
0
.5 1
B.
2
3
4
5
6
7
8 L/day water ingested
Pressure Natriuresis and Pressure Diuresis as the Major Basis for Blood Volume
Control
1.
Mechanical mechanism - most important basis for blood volume control
2.
Pressure diuresis
BP Urine volume
3.
Pressure natriuresis
BP Salt output
4.
Fig. 29-2.
2X BP = 8X urine output
50 mm Hg BP = O urine output
8
Urine Output
L/day
4
1
0
50
100
200
BP mm Hg
39
C.
D.
E.
Mechanism for Blood Volume Control
1.
Similar to arterial pressure control
2.
BV CO urinary output
3.
Rate of change of extracellular fluid volume
intake > output = positive change
intake < output = negative change
4.
E.C.F.V. BV
5.
Feed back control for BV has high gain
BV CO
CO AP
AP Urine output
Effect of Nervous and Hormonal Factors on the Control of Blood Volume
1.
Arterial baroreceptor and low-pressure stretch receptor reflexes
(= volume reflex)
Arterial baroreceptors sympathetic stimulation dilation of
renal arterioles urine output
2.
Atrial natriuretic factor
atria stretch ANF Na and volume excretion
3.
Aldosterone
Na reabsorption H2 O reabsorption
"Aldosterone escape"
4.
Angiotensin - has little effect
5.
ADH - no serious long-term volume changes
6.
Natriuresis and pressure diuresis - most important fundamental controller of
BV
Conditions that cause large increases in Blood Volume
1.
Heart Disease
CO AP urine output volume AP urine output
2.
Polycythemia
viscosity PR Venous Return BV AP urinary output
40
3.
II.
III.
Increased Capacity of Circulation
capacity BV
a.
pregnancy
b.
varicose veins
Control of Extracellular Fluid Volume
A. Normal condition - BV and ECFV are controlled at the same time
B.
Abnormal conditions
1.
capillary pressure
2.
tissue colloid osmotic pressure
3.
plasma colloid osmotic pressure
4.
permeability of capillaries
5.
lymph flow
C.
Normal Distribution of Fluid Volume Between the Interstitial Spaces and
Vascular System
1.
When ECFV rises above 30-50% normal, almost all of it goes into the
interstitial spaces
2.
Interstitial space acts as overflow reservoir
Urea Excretion
A.
25-30 gms/day formed
B.
Rate of urea excretion
1.
concentration of urea in the plasma
2.
GFR
GFR plasma urea
3.
GFR urea excretion
4.
tubular system concentrates urea
5.
urea - most abundant waste product
6.
urea concentration helps to conserve water
41
IV.
V.
Potassium Excretion
A.
K excretion must match K intake
B.
Large amounts of K are reabsorbed in the proximal tubules and thick ascending
limbs due to co-transport with Na.
C.
Active transport by proximal tubules reabsorbs 65%
D.
27% is reabsorbed in thick ascending limb
E.
8% enters distal tubules
F.
distal tubules and cortical collecting ducts can reabsorb K
G.
Principal cells can secrete large quantities of K
H.
Principal cells are very permeable to K
I.
Na+-/K+ pump is the driving force for potassium secretion
J.
Na diffusion from lumen, K secretion
K.
Na absorption, K secretion (hypokalemia)
L.
K secretion altered nervous and cardiac function
M.
ECF K K secretion
N.
Aldosterone Na reabsorption & K secretion
O.
ECF K Aldosterone
P.
Primary aldosteronism K, aldosterone
Q.
Addison's disease K, aldosterone
Renal control of the extracellular concentrations of other ions
A.
Ca - parathyroid hormone
42
B.
PTH calcium reabsorption by kidney and GI
C.
Mg - reabsorbed by all portions of renal tubules
D.
Phosphate
a.
overflow mechanism
b.
PTH promotes phosphate excretion
E. other ions
MICTURITION - Chapter 31
I. Emptying of bladder
A. bladder fills until tension wall increases to threshold
B. micturition reflex - conscious desire to urinate
II. Bladder anatomy
A. body
1. major part
2. where urine collects
B. neck
1. funnel-shaped extension of body
2. passes inferiorly and anteriorly into urogenital triangle
3. connects with urethra
C. detrusor muscle
1. smooth muscle of the bladder
2. muscle fibers extend in all directions
3. empties bladder
D. trigone
1. on posterior wall
2. contains smooth mucosa
E. internal sphincter
1. smooth muscle
2. prevents emptying of bladder
F. urogenital diaphragm
1. skeletal muscle
2. voluntary control
G. innervation of the bladder
1. pelvic nerves via sacral plexus to S-2 and S-3
2. sensory and motor nerves
3. pudendal nerve - external bladder sphincter
4. sympathetic innervation via hypogastric
43
III. Transport of urine through the ureters
A. ureters- innervation from sympathetic and parasympathetic nerves
B. peristaltic contractions
C. ureterorenal reflex - pain in ureter causes constriction of renal
artery thereby reducing urine formation
IV. The micturition reflex
A. result from stretch reflex
B. micturition reflex cycle:
1. progressive and rapid increase in pressure
2. period of sustained pressure
3. return of pressure to basal tonic pressure
C. as bladder fills, micturition reflexes occur more often
D. inhibitory signal to external sphincter must be stronger than
voluntary constrictor signals for urination to occur
E. micturition reflex is completely automatic cord reflex but can
be facilitated by brains centers:
1. facilitatory and inhibitory centers in the brain stem
2. several centers in the cerebral cortex
F. higher brain centers keep micturition inhibited except when desired
G. higher brain centers prevent micturition by tonic contraction of
external sphincter
H. cortical center:
1. facilitate sacral micturition to help initiate a micturition reflex
2. inhibit the external urinary sphincter
I. voluntary urination:
1. contraction of abdominal muscles
2. increased pressure
3. urine enters neck of bladder and posterior urethra
4. stretching of walls
5. stretch receptors excited
6. inhabitation of external urethral sphincter
V. Abnormalities of micturition
A. atonic bladder = destruction of sensory nerve
1. overflow incontinence
2. syphilis - constrictive fibrosis
44
3. crushing injuries to the sacral region
B. automatic bladder
1. if spinal cord is damaged above the sacral segments - reflexes still
occur but without brain control
2. stimulating skin in genital region can sometimes elicit a micturition
reflex
C. uninhibited neurogenic bladder
1. frequent and uncontrollable micturition
2. damage to spinal cord or brain - inhibitory signals interrupted
3. small quantity of urine will elicit an uncontrollable
micturition reflex and urination
D. physiologically stressed bladder
1. increased abdominal pressure
2. examples:
a. coughing
b. laughing
c. sneezing
d. pregnancy
e. obesity
45
46
REGULATION OF ACID-BASE BALANCE
Physiology III, Tri 4
Guyton & Hall, Chapter 30
Dr. Robyn Strader
ABBREVIATIONS:
CO2 = Carbon Dioxide
H+
= hydrogen ion
[H+ ] = hydrogen ion concentration
HCl = Hydrochloric acid (strong acid)
HCO3_ = bicarbonate ion
H2CO3 = bicarbonate base (weak acid)
HPO4 = hydrogen phosphate (base)
H2PO4 = dihydrogen phosphate
H2O = water
NaHCO3= sodium bicarbonate (bicarbonate salt, weak base)
NaOH = sodium hydroxide (strong base)
Na H2PO4 = sodium dihydrogen phosphate
Na2HPO4 = disodium hydrogen phosphate
OH- = hydroxyl ion
mole = that amount of a chemical compound whose mass in grams is equivalent to its
formula mass
equivalent =that weight in grams of a substance which will produce or react with one
mole of hydrogen ion or one mole of electrons
I. Acid-Base Balance
A. overview
1. H+ intake and production must equal net removal
2. H+ critical for homeostasis
B. Systems involved in regulating H+ concentration
47
1. kidney
2. buffering mechanisms
a. blood
b. cells
c. lungs
II. Hydrogen Ion concentration
A. H+ influences most enzymes systems
B. H+ influence almost all cell and body functions
C. H+ in body fluids in relatively low compared to other ions
D. [ H+] averages about .00004 mEq/liter ( =40 nEq/liter, very small amount, normal
range = + 3-5 nEq/liter, range can be as much as 10 - 160 nEq/liter without
causing death)
(equivalent weight = the molecular weight of a substance divided by its valence.
valence is the mass of material that can combine with or replace one mole of
hydrogen ions.)
E. [ H+] is control very precisely
III. Acids and Bases
A. H+ = a single free proton released from a hydrogen atom
B. acids = molecules containing hydrogen atoms that can release hydrogen ions in
solutions
1. HCL + H2O = H+ (hydrogen ions) and Cl- (chloride ions)
2. H2CO3 (carbonic acid) + H2O (water) = H+ + HCO3- (bicarbonate ions)
C. bases = alkali = is an ion or a molecule that can accept a H+
1. HCO3- + H+ = H2CO3 (carbonic acid)
2. HPO4= + H+ = H2PO4-
48
3. alkali = molecule formed by combination of one or more alkaline metals with a
highly basic ion
D. proteins in the body function as bases
1. some of the amino acids in proteins have net negative charges
2. they easily except H+
3. hemoglobin and other proteins are among the most important of the bases of
the body
E. strong acid = rapidly dissociates and releases large amounts of H+ in solutions (HCL)
F. weak acids = do not dissociate easily, release H+ slowly H2CO3
G. strong base = reacts rapidly and strongly with H+,
quickly removes H+ from solution
(ex. OH-, reacts with H+ to form H2O)
H. weak base = binds with H+ much more weakly than does OHI. most acids and bases in extracellular fluid are weak acids and bases
J. [ H+] , because it is so small, is expressed on a logarithm scale
pH = log
1
= - log [H+]
[ H+]
(ex.)
pH = -log [.00000004]
pH = 7.4
K. pH is inversely related to the [ H+]
[ H+] = pH
[ H+] = pH
L. arterial blood
1. normal pH = 7.4
2. acidosis < 7.4
3. alkalosis > 7.4
4. range 6.8 to 8.0
49
M. venous blood and interstitial fluids = pH 7.35, due to extra amounts of
CO2 in the form of H2CO3
N. intracellular pH
1. slightly lower than plasma because of acid production
2. pH range 6.0 - 7.4
O. urine pH range 4.5 - 8.0
P. parietal cells of the stomach mucosa produce HCL with a pH of 0.8
III. Defenses Against Changes In Hydrogen Ion Concentration
A. three primary systems that regulate [H+]
1. chemical acid-base buffer systems of the body fluids
a. react within seconds
b. tie up H+
2. respiratory center
a. acts within a few minutes
b. eliminates CO2 - therefore H2CO3
3. kidneys
a. slower acting
b. eliminates excess acid or base from the body
c. most powerful acid-base regulatory system
B. buffer = any substance that can reversibly bind H+
1. Buffer + H+ H Buffer (=weak acid)
2. 80 mEq/liter of hydrogen is ingested or produced each day (15 to 20 mol)
3. ONLY .00004 mEq/liter of [H+] in body fluid (36 - 44 nmol/L)
a. greater than 44 nmol/L can alter consciousness and lead to coma
b. less than 36 nmol/L can cause neuromuscular irritability, tetany, and
loss of consciousness
C. bicarbonate buffer system
1. most important in the extracellular fluid
50
2. consists of a water solution containing:
a. a weak acid, H2CO3
b. a bicarbonate salt, (ex. NaHCO3)
3. bicarbonate is formed by the body:
carbonic
anhydrase
a. CO2 + H2O H2CO3
b. reaction is slow
c. carbonic anhydrase
1. is necessary to form large amounts of H2CO3
2. is abundant in lung alveoli walls (where CO2 is released)
3. is present in epithelial cells of renal tubules where CO2 reacts
with H2O to form H2CO3
4. ionizes weakly to form small quantities of H+ and HCO3H2CO3 H+ + HCO34. bicarbonate salt
a. occurs predominantly as sodium bicarbonate (NaHCO3)
b. in extracellular fluid
c. NaHCO3 ionizes almost completely to form bicarbonate ions (HCO3)
and sodium ions (Na+)
Na HCO3 Na+ + HCO35. CO2 + H2O H2CO3 H+ + HCO3- + Na+
Lung
Kidney
(Because of the weak dissociation of H2CO3, the H+ concentration is
extremely small.)
6. When a strong acid (ex. HCl) is added to the bicarbonate buffer solution, the
increased hydrogen ions released from the acid are buffered by HCO3..
HCl H+ + ClH+ + HCO3- H2CO3 - CO2 + H2O
therefore, more CO2 and H2O are formed
51
7. CO2 stimulates respiration and CO2 is eliminated from the extracellular fluid
8. When a strong base (ex. NaOH) is added to the bicarbonate buffer solution the
hydroxyl ion (OH-) from the NaOH combines with H2CO3 to form HCO3-.
The weak base NaHCO3 replaces the strong base NaOH. H2CO3 decreases
causing more CO2 to combine with H2O to replace H2CO3:
NaOH + H2CO3 NaHCO3 + H2O
CO2 + H2O H2CO3 HCO3- + H+
+
+
NaOH
Na
therefore, CO2 levels in the blood and respiration is inhibited. The
increase in HCO3- is compensated for by renal excretion of HCO3-.
IV. Quantitative Dynamics Of The Bicarbonate Buffer System
A. a buffer's capacity to minimize changes in pH is related to the dissociation
characteristics of the weak acid or base in the presence of its respective salt.
B. a strong acid or base will dissociate almost completely
C. a weak acid or base tends to dissociate very little
weak acid base/salt + [H+]
[HA] [A-] + [H+]
[CH3COOH] [CH3COO-] + [H+]
acetic acid
acetate
the concentrations of hydrogen ions and bicarbonate ions are proportional to the
concentration of H2CO3
H2CO3 H+ + HCO3-
D. for any acid, the concentration of the acid relative to its dissociated ions is defined by
the dissociation constant K':
H+ HCO3K' = H2CO3
52
H+ = K' CO2
HCO3
Clinically, CO2 tension (Pco2) is measured instead of CO2. Under physiological
conditions, the solubility coefficient for CO2 is 0.03 mmol/mm Hg at body temperature
H+ = K (0.03 Pco2)
HCO3-
calculation for a weak acid dissociation constant (Ka)
[A-][H+]
Ka = [HA]
A = proton acceptor (Base/Salt)
HA = proton donor (Weak Acid)
[HA]
[H ] = Ka [A-]
+
taking the log of each quantity and then multiplying by -1, the equation can be rewritten as:
[HA]
-log [H+] = -log Ka -log [A-]
p = minus log of
-log = p
53
[HA]
pH = pK - log [A-]
Eliminating the minus sign in front of the log results in an equation known as the
Henderson-Hasselbalch equation. It describes the dissociation characteristics of weak
acids and bases and the effect on pH.
[A]
pH = pK + log [HA]
pH =pK + log
HCO3(0.03 Pco2)
the pK of bicarbonate buffer system is 6.1
pH =6.1 + log
HCO3(0.03 Pco2)
E. when the ratio of [A- ] to [HA] is 1, the pH is equal to pK and the buffer has its
greatest buffering capability.
F. the dissociation constant Ka and therefore pKa remain the same for a given substance
G. any changes in pH are due to the ratio of base/salt [A-] concentration to weak acid
[HA] concentration
H. metabolic acidosis = acidosis caused by a primary decrease in bicarbonate
concentration
I. metabolic alkalosis = alkalosis caused by a primary increase in bicarbonate
concentration
J. respiratory acidosis = acidosis caused by an increase in Pco2
K. respiratory alkalosis = alkalosis caused by a decrease in Pco2
L. the bicarbonate buffer system is the most important extracellular buffer
M. there is 20 times more HCO3- than dissolved CO2 in the bicarbonate buffer system
V. The Phosphate Buffer System
A. not a major extracellular fluid buffer
B. plays major role in buffering renal tubular fluid and intracellular fluids
54
1. phosphate usually becomes greatly concentrated in the tubules - increasing the
buffering power of the phosphate system
2. the tubular fluid usually has a considerably lower pH than extracellular fluid operating range closer to buffer pK of 6.8
3. phosphate concentration inside the cell is many times more than outside of the
cell
4. intracellular pH is lower than that of extracellular fluid
C. has a pK of 6.8
D. low concentration in extracellular fluid = 8%
E. main elements of the phosphate buffer system are:
1. H2PO4- (weak acid)
2. HPO4= (base)
when a strong acid is added:
HCL + Na2HPO4 NaH2PO4 + NaCl
strong acid is converted to weak acid
when a strong base is added:
NaOH + NaH2PO4 Na2HPO4 + H2O
strong base becomes weak base
VI. Protein Buffers
A. most plentiful buffers
B. hemoglobin
H+ + Hb HHB
C. 60 to 70% of total chemical buffering of the body fluids inside of the cell - mostly
due to protein
D. H+ and bicarbonate ions move through the cell membrane very slowly - therefore it
takes hours for the intracellular proteins to buffer the extracellular fluid.
E. pK of many proteins is near 7.4
VII. Respiratory Regulation of Acid-Base Balance
A. second line of defense - CO2 concentrations controlled by the lungs
B. Pco2 pH, Pco2 pH
C. rate of alveolar ventilation Pco2
D. [H+] stimulates alveolar ventilation
55
56
RENAL CONTROL OF ACID-BASE BALANCE
Physiology III, Tri IV
Guyton & Hall, Chapter 30, page 392
Dr. Robyn Strader
I. Kidneys
A. secrete acidic or basic urine
B. large amounts of bicarbonate ions are filtered by tubules
C. large amounts of H+ are filtered by tubules
D. body produces 80 mEq of nonvolatile acids/day from protein metabolism
nonvolatile acids = are not H2CO3, not excreted by the lungs
E. the primary method for removal of body acid is renal excretion
F. kidney prevent loss of bicarbonate (more important than excretion of acids)
G. body filters 4320 mEq of bicarbonate/day (180 24 mEq/liter)
H. almost all bicarbonate is reabsorbed from the tubules
I. 4320 mEq of H+ must be secreted each day to reabsorb the filtered bicarbonate
J. an additional 80 milliequivalents must be secreted to rid the body of nonvolatile acids
(4320 + 80 = 4400 mEq of H+ secreted into the tubular fluid each day)
K. H+ reabsorption of bicarb bicarbonate excretion
alkalosis bicarb excretion [H+] in extracellular
L. in acidoses, the kidney reabsorb all the filtered bicarbonate and produce new
bicarbonate
M. Kidneys regulate extracellular fluid hydrogen ion concentration by:
1. secretion of hydrogen ions
2. reabsorption of filtered bicarbonate ions
3. production of new bicarbonate ions
57
100
80
[H+]
60
(nEq/L)
40
20
0
7.0
7.2
7.4
7.6
7.8
8.0
pH
II. Secretion of H+ and reabsorption of bicarbonate ions by the renal tubule
A. H+ secretion & HCO3 reabsorption occur in almost all parts of the tubules except the
descending and ascending thin limbs of the loop of Henle (see figure 30-4)
B. for a HCO3 to be absorbed, there must be a H+ secreted
C. 80 - 90% of H+ secretion and HCO3 reabsorption occurs in the proximal tubule
D. 10% in thick ascending limb
E. remaining amount is reabsorbed in distal tubule and collecting duct
F. in the Proximal tubule, H+ is counter transported with Na+ (see figure 30-5)
** G. for every H+ secreted into the tubular lumen, a bicarbonate ion enters the blood
H. HCO3 does not diffuse into renal tubular cells very well
1. it must first bind with H+ to form H2CO3
2. it then becomes CO2 and H2O
3. CO2 diffuses into cell and binds with H2O under the influence of carbonic
anhydrase to form H2CO3
4. H2CO3 dissociates to form HCO3 and H+
I. each time a H+ is formed in the tubular epithelial cells, a HCO3 is also formed and
released back into the blood
J. in the distal tubule and collecting duct, (5%) H+ are actively secreted by the
intercalated cells
1. the dissolved CO2 in the cell combines with H2O to form H2CO3
2. the H2CO3 then dissociated into HCO3 (goes to blood) and H+ (secreted into
tubule via ATP-ase pump)
58
3. H+ moves via ATPase pump in distal tubule and collecting duct and countertransport in proximal tubule
K. in the proximal tubule [H+] can be increased 3-4 fold, even though large amounts of
H+ are present
L. in the distal tubule, [H+] can be increased as much as 900-fold
M. this lowers urine pH to about 4.5
Interstitium
Lumen
Na + HCO3
Na
Na
ATP
K
H
HCO3 + H
H2CO3
H2CO3
carbonic
anhydrase
CO2
H2O
+
CO2
CO2 + H2O
III. Excess H+, phosphate and ammonia buffers
A. only a small amount of excess hydrogen ions can be excreted in the urine in the
form of H+
B. minimal urine pH is 4.5 = [H+] of 10-45 mEq/L or 0.03 mEq/Liter
C. for each liter of urine formed, a maximum of 0.03 mEq of free H+ can be excreted
D. therefore, to excrete the 80 mEq of nonvolatile acid formed each day would require
2667 liters of urine
E. ammonia and phosphate buffers are used to remove the excess H+
59
Interstitium
Lumen
Cl
Cl
ATP
H
HCO3 + H
H2CO3
carbonic
anhydrase
H2O
+
CO2
CO2
Interstitium
Lumen
Na + NaHPO4
Na
Na
ATP
K
H
HCO3 + H
H2CO3
H + NaHPO4
H2O
+
CO2
NaH2PO4
carbonic
anhydrase
CO2
Interstitium
Glutamine
Lumen
Glutamine
Glutamine
Cl
2HCO3
2NH4
NH4
Na
NH4 + Cl
Na
60
IV. Phosphate Buffer system
A. composed of HPO4= and H2PO41. both become concentrated in the tubular fluid
2. both are poorly reabsorbed
B. pK of phosphate system is 6.8
C. in the urine, phosphate buffer system normally functions near its most effective range
D. after H+ binds with HPO4= to form H2PO4-, it can be excreted as a sodium salt
(NaH2PO4)
E. under normal conditions, much of the phosphate is reabsorbed and is not available for
buffering H+
F. much of the H+ buffering system is due to ammonia
Interstitium
Lumen
NH3
Na
NH3
Na
ATP
K
H
Cl
HCO3 + H
H2CO3
NH4 + Cl
carbonic
anhydrase
H2O
+
CO2
CO2
V. Ammonia Buffering System
A. composed of NH3 (ammonium) and NH4+ (ammonia ion)
B. NH4+ is synthesized from glutamine
C. glutamine:
1. transported into the epithelial cells of proximal tubule, thick ascending limb
of the loop of Henle and distal tubules
2. is metabolized to form two NH4+ and HCO3
61
D. NH4+ is secreted into the tubular lumen by the counter-transport mechanism in
exchange for sodium, which is reabsorbed
E. HCO3- moves with Na+ into interstitial fluid and into capillaries
F. for each molecule of glutamine metabolized in the proximal tubules,
two NH4+ ions are secreted into the urine and two HCO3- ions are reabsorbed
into the blood
G. the HCO3- formed constitutes new bicarbonate
H. in the collecting duct:
1. H+ is secreted by the tubular membrane into the lumen
2. combines with NH3 to form NH4+ which is then excreted
3. the collecting ducts are permeable to NH3 , it can easily diffuse into
tubular lumen
4. luminal membrane in collecting ducts is less permeable to NH4+
5. Once H+ has reacted with NH3 to form NH4, it is trapped in the tubular
lumen and eliminated in the urine
6. for each NH4+ excreted, a new HCO3- is generated and added
to the blood
I. increase ECF H+ concentration stimulates renal glutamine metabolism and
increases the formation of NH4+ and new bicarbonate to the be used in H+
buffering
J. a decrease in [H+] has the opposite effect
K. Under normal conditions, the amount of H+ eliminated by the ammonia buffer
system accounts for about 50% of the acid excreted and 50% of the new
bicarbonate generated by the kidneys
L. during chronic acidosis, the dominant mechanism by which acid is eliminated
and bicarbonate is generated is excretion of NH4+
62
VI. Quantifying Renal Acid-Base Excretion
A. bicarbonate excretion = urine flow rate X urinary bicarbonate concentration
B. indicates how rapidly the kidneys are removing bicarbonate ions from the
blood ( = adding H+ to the blood)
C. bicarbonate added to the blood = H+ secreted with non-bicarbonate urinary
buffers (urine flow rate X urinary NH4+ concentration)
VII. Regulation of Renal Tubular Hydrogen Ion Secretion
A. H+ secretion by the tubular epithelium is necessary for:
1. bicarbonate reabsorption
2. generation of new bicarbonate associated with titratable acid formation
B. H+ secretion must be carefully regulated if the kidney are to regulated acidbase homeostasis
C. under normal conditions:
1. the kidney tubules must secrete at least enough H+ to reabsorb almost
all the bicarbonate that is filtered
2. there must be enough H+ left over to be excreted as titratable acid or
NH4+ to rid the body of the nonvolatile acids produced each day from
metabolism
D. in alkalosis:
1. tubular secretion of H+ must be reduced to a level that is too low to
achieve complete bicarbonate reabsorption - enabling the kidneys to
increase bicarbonate excretion
2. titratable acid and ammonia are not excreted because there are no
excess H+
available to combine with non-bicarbonate buffers
3. there is no new bicarbonate added to the urine in alkalosis
E. in acidosis:
1. tubular H+ secretion must be increased sufficiently to reabsorb all the
filtered bicarbonate and-
63
2. have enough H+ left over to excrete large amounts of NH4 and
titratable acid
3. large amounts of new bicarbonate ions are added to the blood
F. the most important stimuli for H+ secretion by the tubules in acidosis are:
1. an increase in Pco2 of the extracellular fluid
2. an increase in H+ of the extracellular fluid (pH)
G. aldosterone stimulates the secretion of H+ by the intercalated cells of the
collecting duct (Conn's syndrome) excessive secretion of H+ and
increased bicarbonate added back to the blood alkalosis
H. in alkalosis:
1. H+ secretion
2. can occur as a result of a decreased extracellular Pco2
3. can occur as a result of a H+ concentration
pH
H+nEq/L Pco2 mm Hg
7.4
40
Respiratory Acidosis
Respiratory Alkalosis
Metabolic Acidosis
Metabolic Alkalosis
Normal
HCO3 mEq/L
40
24
VIII. Renal Correction of Acidosis
A. acidosis occurs when ratio of HCO3- to CO2 in the extracellular fluid
decreases pH
B. if the ratio decreases due to fall in HCO3- = metabolic acidosis
C. if pH falls due to Pco2 = respiratory acidosis
D. in acidosis:
1. kidneys reabsorb all the filtered bicarbonate
2. kidneys contribute new bicarbonate through the formation of NH4+ and
titratable acid
64
E. metabolic acidosis = H+/HCO3- in tubule fluid due to filtration of HCO3
F. respiratory acidosis = H+ in tubular fluid due to rise in extracellular fluid
Pco2, which stimulates H+ secretion
G. with chronic acidosis there is NH4+ production
IX. Renal Correction of Alkalosis
A. alkalosis = ratio of HCO3- to CO2 in the extracellular fluid , causing
a rise in pH
B. excess bicarbonate ions in tubules are excreted in the urine
X. Clinical Causes of Acid-Base Disorders
RESPIRATORY ACIDOSIS
A. pulmonary ventilation Pco2 H2CO3 & H+ respiratory acidosis
B. causes of respiratory acidosis:
1. damaged respiratory center
2. decreased ability of lungs to eliminate CO2
3. obstruction of respiratory tract passageways
4. pneumonia
5. pulmonary membrane surface area
6. interference with gas exchange
C. respiratory acidosis compensatory responses:
1. buffers of the body fluids
2. kidneys
RESPIRATORY ALKALOSIS
A. caused by overventilation by the lungs
B. generally not caused by physical pathological conditions - but psychoneurosis
C. high altitude - low O2 stimulates respiration CO2 and mild respiratory
alkalosis
65
METABOLIC ACIDOSIS
A. caused by extracellular fluid bicarbonate concentration
B. metabolic acidosis = all other types of acidosis besides those caused by excess
CO2 in the body fluid
C. causes of metabolic acidosis
1. failure of the kidneys to excrete metabolic acids normally formed in
the body
2. formation of excess quantities of metabolic acids in the body
3. addition of metabolic acids to the body by ingestion of infusion
of acids
4. loss of base from the body fluids, which has the same effect as adding
an acid to the body fluids
5. other causes:
a. renal tubular acidosis
b. diarrhea
c. vomiting
d. diabetes mellitus
e. ingestion of acids
f. chronic renal failure
METABOLIC ALKALOSIS
A. caused by increased extracellular fluid bicarbonate concentrations
B. retention of bicarbonate of loss of H+
C. not as common as acidosis
D. causes:
1. administration of diuretics
2. excess aldosterone
3. vomiting of gastric contents
4. ingestion of alkaline drugs
(FIG. 30-10)
66
Arterial Blood Sample
pH
Acidosis
Alkalosis
Metabolic
Respiratory
Metabolic
Respiratory
Respiratory
Compensation
Renal
Compensation
Respiratory
Compensation
Renal
Compensation
67
68
General Principles of Gastrointestinal Function Motility, Nervous Control, and Blood Circulation
Physiology III, Tri 4
Guyton & Hall, Chapt. 62
Dr. Robyn Strader
I. Alimentary tract
A. tube like structure
1. approximately 6' long
2. length increases with relaxation of longitudinal muscle
B. provides the body with:
1. water
2. electrolytes
3. nutrients
C. functions:
1. movement of food
2. storage of food
3. secretion of digestive juices
4. digestion of food
5. absorption of digestive products
II. Gastrointestinal motility
A. layers of intestinal wall: (internal to external)
1. mucus layer (mucosa)
a. epithelium
b. lamina propria
1. collagen
2. elastin
3. glands
4. lymph nodes
5. vascular supply
6. mucosa - contains muscularis mucosae
69
2. submucosa
a. submucosal plexus
b. (aka) Meissner's plexus
3. muscularis externa
a. longitudinal muscle layer
b. circular muscle layer
c. myenteric plexus (Auerbach's plexus)
4. serosa
B. smooth muscle
1. 200-500 m in length
2. 2-10 m in diameter
3. arranged in bundles (up to 1000 parallel fibers)
4. extend down the intestinal tract (longitudinal muscle layer)
and around the gut (circular muscular layer)
5. connected by gap junctions - allowing for movement of ions
from one cell to the next
6. electrical signals travel readily, longitudinally from one fiber
to the next within a bundle 7. muscle functions as syncytium - bundles are separated by
connective tissue but are fused at points
8. excitation can travel through muscle layers
9. cell structure
a. caveolae - may function similar to T-tubules
b. no T-tubule system in smooth muscle
c. dense bodies
1. act as Z bands
2. contain actin
3. held in place by intermediate bodies
d. contains mitochondria
e. limited Golgi apparatus
f. Ca++-Calmodulin pathway
70
1. phosphorylatoin of myosin
2. activated myosin binds with actin to form contraction
3. slow & steady
III. Electrical activity
A. GI smooth muscle exhibits almost continual slow electrical
activity, usually in rhythm
B. types of electrical waves:
1. slow waves
a. determine rhythm of GI contractions
b. undulating changes in resting membrane
potential - are not action potentials
c. resting membrane potential -50 to -60 mV
d. intensity = 5 - 15 mV
e. frequency = 3- 12 / min. (3 in stomach, 12 in duodenum,
8 - 9 in terminal ileum)
f. cause of slow waves is unknown - maybe slow undulation
of Na+/K+ pump
g. usually cause contraction only in the stomach
h. in the stomach - slow waves initiate contractions
i. control appearance of intermittent spike potentials
2. spike potentials
a. cause most of the muscle contraction
b. true action potentials
c. occur when resting membrane exceeds -40 mV (becomes more
positive)
d. last 10 - 40 times longer (slower) than action potential in
large nerves
e. generated by calcium-sodium channels (slower than sodium
channels) slow to open & slow to shut
71
f. movement of calcium into muscle fiber during the action
potential enhances smooth muscle contraction
g. produce about 1-10/sec
h. caused by increased depolarization
3. changes in the voltage of the resting membrane potential
a. resting membrane potential
1. average = -56 mV
2. range = -50 to -60 mV
b. depolarization
1. membrane becomes more positive and excitable
2. factors that depolarize the membrane:
a. stretching of the muscle
b. stimulation by acetylcholine
c. stimulation by the parasympathetic nerves that
secrete acetylcholine
d. stimulation by GI hormones
c. hyperpolarization
1. membrane becomes more negative and less excitable
2. factors that hyperpolarize the membrane
a. epinephrine
b. norepinephrine
c. sympathetics
4. calcium ions
a. entry of calcium into muscle fiber causes contraction
b. not affected by slow waves
c. large amounts of calcium enters muscles during spike
potentials and causes contraction
5. tonic contraction of some GI smooth muscle
(not completely understood)
a. continuous contraction
72
b. not associated with basic electrical rhythm of slow waves
c. lasts several minutes to several hours with varying intensity
d. can be caused by:
1. repetitive spike potentials
2. hormones
3. factors causing continuous depolarization without
causing action potentials
4. continuous entry of calcium
(channel stuck in open position)
IV. Neural Control
A. enteric nervous system
1. nervous system of GI tract - contains 2 plexuses
2. lies in the wall of the gut
CNS
Sympathetic and
Parasympathetic efferents
Myenteric Plexus
Submucosal Plexus
Chemoreceptors
Mechanoreceptors in
wall of gastrointestinal
tract
Muscularis externa
Muscularis Mucosae
Endocrine cells
Secretory cells
Blood Vessels
73
EXTRINSIC NERVOUS SYSTEM
ACH or peptides
ACH
Mucosa
NE
NE
Muscularis mucosae
Endocrine cells
Secretory cells
Submucosal plexus
NE
ACH or peptides
NE
NE
Circular muscle
ACH
Myenteric Plexus
NE
ACH or peptides
Vagus nerve or pelvic nerve
Longitudinal muscle
Sympathetic
ganglia
Parasympathetic
ACH
Sympathetic
74
INTRINSIC NERVOUS SYSTEM
Mucosa
Secretory
Cells
Endocrine
Cells
Mechanoreceptors
Chemoreceptors
Submucosal plexus
Circular muscle
Myenteric
Longitudinal muscle
Parasympathetic
Sympathetic
75
3. begins in the esophagus
4. extends to anus
5. contains about 100 million neurons
6. controls primarily GI movements and secretion
7. contains sympathetic and parasympathetic fibers
8. can function on its own or with the ANS
B. enteric plexuses:
1. myenteric plexus or Auerbach's plexus (cord appearance)
a. outer plexus
b. lies between the longitudinal and circular muscle layers
c. controls mainly the GI movements
1. increases tonic contraction (= tone of gut)
2. increases intensity of rhythmical contractions
3. slightly increases rate of rhythm of contraction
4. increases velocity of conduction (increases movement of
peristaltic waves)
d. mostly linear chains of interconnecting neurons extending
the length of the gut
e. excitatory and inhibitory
f. inhibitory to pyloric sphincter and ileocecal valve sphincter in order to move food
2. submucosal plexus or Meissner's plexus (net or mesh appearance)
a. inner plexus
b. lies in submucosa
c. controls mainly GI secretions and local blood flow
d. controls function of inner wall
1. local intestinal secretion
2. local absorption
3. local contraction of muscularis mucosae - causes folds
in intestinal mucosa
76
Neurotransmitters and Neuromodulators in the Enteric Nervous System
Substance
Source
Actions
Acetylcholine (ACH)
Cholinergic neurons
Contraction of smooth muscle in wall
Relaxation of sphincters
Salivary secretion
Gastric secretion
Pancreatic secretion
Norepinephrine (NE)
Adrenergic neurons
Relaxation of smooth muscle in wall
Contraction of sphincters
Salivary secretion
Vasoactive intestinal
peptide (VIP)
Neurons of mucosa &
smooth muscle
Relaxation of smooth muscle
Intestinal secretion
Pancreatic secretion
Gastrin-releasing peptide
(GRP) or bombesin
Neurons of mucosa and Gastrin secretion
smooth muscle
Enkephalins (opiates)
Neurons of mucosa and Contraction of smooth muscle
smooth muscle
Intestinal secretion
Neuropeptide Y
Neurons of mucosa and Relaxation of smooth muscle
smooth muscle
Intestinal secretion
Substance P
Co-secreted with ACH
Contraction of smooth muscle
Salivary secretion
C. neurotransmitters secreted by the enteric neurons (functions are not completely understood)
1. acetylcholine - most often excites GI activity
2. norepinephrine - almost always inhibits GI activity
3. adenosine triphosphate
4. serotonin
5. dopamine
6. cholecystokinin
7. substance P
8. vasoactive intestinal polypeptide
77
9. somatostatin
10. leu-enkephalin
11. met-enkephalin
12. bombesin
D. autonomic control of GI tract
1. parasympathetic innervation - extensive supply to portions nearest the
oral cavity and anus
a. two division:
1. cranial
2. sacral
b. transmitted almost entirely in the vagus nerves
c. innervate:
1. esophagus
2. stomach
3. pancreas
4. less extensive innervation to the intestines through
"approximately" the first half of the large intestine
d. sacral parasympathetics:
1. originate in 2nd, 3rd, 4th sacral segments
2. pass through pelvic nerves to distal ½ of large intestine
3. sigmoidal, rectal and anal regions highly supplied
with parasympathetics for defecation reflexes
e. postganglionic neurons:
1. located in the myenteric and submucosal plexuses
2. stimulation causes general increase in activity of entire
enteric nervous system; mostly excitatory but some
inhibitory
2. sympathetic innervation:
a. originate between segments T-5 and L-2
b. most enter and pass through sympathetic chain to
outlying ganglia
78
Hank's Solution
Gut
Motility
ACH
EPI
c. most postganglionic neuron bodies are located in the celiac
ganglion (CG), superior mesenteric ganglia (SMG), and inferior
mesenteric ganglia (IMG)
d. innervate all portions of gut
e. nerve endings secrete norepinephrine
f. generally inhibits activity
g. effects:
1. norepinephrine inhibits most smooth muscle
2. norepinephrine excites mucosae
3. norepinephrine inhibits neurons of the enteric
nervous system
4. strong sympathetic stimulation can block movement of
food through the GI tract
E. afferent sensory nerve fibers from the gut
1. many afferent sensory nerve fibers arise in the gut
2. some have cell bodies in the enteric nervous system
3. stimulated by:
a. irritation of the gut mucosa
b. excessive distention of the gut
c. presence of specific chemical substances in the gut
4. can cause excitation or inhibition
5. types:
a. afferent fibers that terminate in the enteric nervous system
b. afferent fibers with cell bodies in the enteric nervous system but
sends axon through the ANS nerves to terminate in the
prevertebral sympathetic ganglia (celiac, mesenteric, and
hypogastric ganglia)
79
c. afferent fibers with cell bodies in the dorsal root ganglia of s.c.
or cranial nerve ganglia; transmitting signal directly into spinal
cord or brain stem via nerve trunks along with the ANS fibers
(ex. vagus, which is 80% afferent, transmits into medulla and
initiates GI reflexes)
F. GI reflexes - 3 types
1. reflexes that occur entirely within the enteric nervous system (i.e.,
reflexes that control GI secretion, peristalsis, mixing contractions, local
inhibitory effects, etc.)
2. reflexes from the gut to the prevertebral sympathetic ganglia and
then back to the GI tract
a. transmits signals for long distances
b. gastrocolic reflex - from stomach to colon to cause evacuation
of the colon
c. enterogastric reflexes - signals from colon and small intestine to
inhibit stomach motility and stomach secretion
d. coloileal reflex - reflexes from the colon to inhibit emptying
of ileal contents into the colon
3. reflexes from the gut to the spinal cord or brain stem and them back to
the GI tract
a. reflexes from the stomach and duodenum to the brain stem and
back to the stomach - by way of the vagus nerves - to control
gastric motor and secretory activity
b. pain reflexes that cause general inhibition of the entire
gastrointestinal tract - generally inhibit gut motility
c. defecation reflexes that travel to the spinal cord and back again
to produce the powerful colonic, rectal, and abdominal
contractions required for defecation (=defecation reflexes)
80
Summary of Gastrointestinal Hormones
Hormone
Site of Secretion
Stimuli for Secretion
Actions
Gastrin
G-cells of the stomach
Small peptides and
amino acids
Distention of the
stomach
Vagal stimulation
(GRP)
Gastric H+ secretion
Stimulates growth of
gastric mucosa
Cholecystokinin cells of the duodenum
(CCK)
and jejunum
Small peptides and
amino acids
Fatty acids
Pancreatic enzyme
secretion
Pancreatic HCO3secretion
Stimulates contraction of
the gallbladder and
relaxation of the
sphincter of Oddi
Stimulates growth of the
exocrine pancreas
and gallbladder
Inhibits gastric emptying
Secretin
S cells of the duodenum
H+ in the duodenum
Fatty acids in the
duodenum
Pancreatic HCO3secretion
Biliary HCO3secretion
Gastric H+ secretion
Inhibits trophic effect of
gastrin on gastric
mucosa
Gastric
inhibitory
peptide (GIP)
Duodenum and
jejunum
Fatty acids
Amino acids
Oral glucose
Insulin secretion
from pancreatic
cells
Gastric H+ secretion
V. Hormonal Control of GI Motility
A. cholecystokinin
1. secreted by "I" cells in the mucosa of duodenum & jejunum
2. secreted in response to breakdown products of fat, fatty acids, and
monoglycerides
3. potent stimuli for contraction of gallbladder for the release of bile for
the emulsification of fatty substances
4. inhibits stomach motility moderately
81
B. secretin
1. secreted by "S" cells in the mucosa of duodenum
2. secreted in response to acidic gastric juice emptied from stomach
through the pylorus
3. mild inhibitory effect on the motility of most of the GI tract
C. gastric inhibitory peptide
1. secreted by the mucosa of the upper small intestine
2. secreted in response to fatty acids, amino acids, and to a lesser extent
in response to carbohydrates
3. mild effect on decreasing motor activity of the stomach
4. slows emptying of gastric contents into the duodenum when the upper
small intestine is already filled
VI. Functional Types of Movements in the Gastrointestinal Tract
A. propulsive movements
1. move food along the tract at an appropriate rate for digestion and
absorption
2. peristalsis = basic propulsive movement - aids in mixing
Orad
Caudad
Contraction
Peristaltic Contraction
3. contractile ring around gut moving forward
4. stimuli for peristalsis:
a. distention of the gut
b. irritation of the epithelial lining
c. extrinsic nervous signal (particularly parasympathetic)
82
Orad
Contraction
Caudad
Segmentation Contraction
5. effectual peristalsis requires an active myenteric plexus
6. peristalsis diminished or halted by:
a. congenital absence of myenteric plexus
b. atropine (paralyzes cholinergic nerve endings of
myenteric plexus)
7. peristalsis essentially moves analward
8. peristaltic wave moves 5 to 10 centimeters
9. receptive relaxation = peristaltic wave causes gut to relax downstream
10. myenteric reflex = peristaltic reflex (pattern of peristaltic wave and
downstream relaxation)
11. "law of the gut" = peristaltic reflex + analward direction of movement
of the peristalsis
B. mixing movements - rhythmical segmentations
1. keep intestinal contents thoroughly mixed
2. varying throughout the GI tract
3. local constrictive contractions occur every few centimeters in
the gut wall
Mixing Movements - Rhythmical Segmentations
83
C. migrating motor complex: (this section is found in chapt. 63 of G&H)
1. occurs many hours after eating or during fasting
2. recurs about every 90 minutes
3. moderately active peristaltic waves sweep slowly downward
along the stomach and small intestine
4. sweeps excess digestive secretions and debris into colon
5. begins in body of stomach and spreads through the ileum
6. 40 cm area of contraction moves @ 6-12 cm/min
7. a block of about 50 waves lasts about 6-10 min
8. when one complex reaches ileum, another starts in stomach
Migrating Motor Complex
VII. GI Blood Flow
A. splanchnic circulation - blood flow in gut, spleen, pancreas, and liver
B. blood flows through gut, spleen and pancreas and then to liver via portal vein
C. goes through liver sinusoids and leaves lever via hepatic veins and into
vena cava
D. reticuloendothelial cells lining sinusoids remove bacteria, etc., from GI tract
E. most non-fat, water-soluble nutrients absorbed from the gut are transported via
the portal venous blood
F. reticuloendothelial cells and hepatic cells of liver absorb and store temporarily,
½ to ¾ of all absorbed nutrients
84
G. most absorbed non-water-soluble, fat-based nutrients are almost all absorbed
into the intestinal lymphatics and returned to the blood by way of the thoracic
duct
H. blood supply:
1. superior mesenteric artery (walls of small and large intestine)
2. inferior mesenteric artery (walls of small and large intestine)
3. celiac artery (stomach)
I. blood flow after a meal:
1. 100-150%
2. muscle activity
3. secretions
4. absorption
J. local blood flow is directly related to local metabolism
1. increased release of vasodilators from mucosa
(most are peptide hormones)
a. cholecystokinin
b. vasoactive intestinal peptide
c. gastrin
d. secretin
e. adenosine
85
2. kinins released from GI glands (powerful vasodilators)
a. kallidin
b. bradykinin
3. decreased O2 concentration in the gut
K. countercurrent blood flow mechanism in the villi
1. arterial and venous flow are in opposite directions = countercurrent
2. O2 diffuses from arterioles to venules without reaching top of venule
(this can be a problem when coupled with other GI pathologies)
L. nervous control of GI blood flow
1. parasympathetic nerves to stomach and lower colon indirectly blood
flow along with glandular secretion
2. sympathetic stimulation has a direct effect on almost all the GI tract by
causing intense vasoconstriction of the arterioles
3. autoregulatory escape will override sympathetic stimulation to protect
GI tract
4. sympathetic vasoconstriction plays an important role in crisis
a. 200-300 ml of blood shunted from GI
b. exercise
c. circulatory shock
d. hemorrhagic shock
e. fight or flight
86
87
Transport and Mixing of Food in the Alimentary Tract
Physiology III, Tri 4
Guyton & Hall, Chapter 63
I. Ingestion of Food
A. controlled by:
1. hunger
a. desire for food
b. regulates intake of food
2. appetite - type of food desired
B. mastication = chewing - needs teeth & tongue
1. incisors
a. anterior teeth
b. strong cutting action
c. chisel shaped
2. molars
a. posterior teeth
b. grinding action
c. flat surface
d. strong root structure
3. jaw muscles generated force - up to 55 lbs. on incisors and
200 lbs. on molars
4. most muscles of chewing - innervated by motor branch of the 5th
cranial nerve
5. controlled by nuclei in brain stem
6. stimulation for continual rhythmical chewing movements
a. reticular formation near center for taste
b. areas of hypothalamus, amygdala and cerebral near sensory
areas for taste and smell
88
7. chewing reflex = presence of a bolus of food in the mouth at first
initiates reflex inhibition of the muscles of mastication, causing the
lower jaw to drop. The drop initiates a stretch reflex that leads to
rebound contraction, raising the jaw to cause closure of the teeth. The
bolus is compressed against the linings of the mouth and the process is
repeated.
8. break cellulose membranes of fruits and vegetables
9. increases surface area - rate of digestion is dependent on surface area
10. prevents excoriation (scratching) of GI tract
C. swallowing = deglutition
esophagus
1. complicated mechanism
><
2. passage of food is coordinated with breathing
3. stages of:
stomach
a. voluntary stage - initiates swallowing
b. pharyngeal stage - involuntary; constitutes passage of food
through pharynx into esophagus
1. stimulation of swallowing receptor areas of posterior
mouth and pharynx by bolus
2. stimulus travels to brainstem to initiate series of
automatic pharyngeal muscle contractions
3. soft palate is pulled upward to close posterior nares
4. palatopharyngeal folds (arches) are pulled medially to
form a sagittal slit for the passage of food (lasts about 1
sec.)
5. sagittal slit allows only sufficiently masticated
food to pass
6. larynx & hyoid bone is pulled upward and anteriorly by
neck muscles
7. epiglottis swings backward over the opening of the
larynx
8. food is prevented from entering the trachea
89
9. opening of the esophagus enlarges
10. upper esophageal sphincter (a.k.a. pharyngoesophageal
sphincter) relaxes, allowing food to pass (between
swallows it remains constricted)
11. when larynx is raised and pharyngoesophageal sphincter
is relaxed, a rapid peristaltic wave begins at the superior
part of the pharynx and spreads to the esophagus
12. summary- trachea closes, esophagus opens, fast
peristaltic wave forces food into esophagus
13. process takes less than 2 seconds
14. nervous control:
a. tactile area lie in ring around pharyngeal opening
b. sensory impulses are transmitted to trigeminal
and glossopharyngeal nerves in medulla in/near
tractus solitarius
c. stages of swallowing are controlled by reticular
substance of medulla and lower pons
d. sequence and timing of swallowing remains
constant
e. motor impulses - 5th, 9th, 10th, 12th, and superior
cervical nerves
f. swallowing is a reflex initiated by food in the
back of the mouth
g. swallowing center of medulla overrides
respiratory center
c. esophageal stage - involuntary
1. passage of food from pharynx to stomach
2. 2 types of peristaltic movements
a. primary peristalsis
1. continuation of pharyngeal peristalsis
2. passes from pharynx to stomach in
90
8-10 sec.
3. aided by gravity
b. secondary peristalsis
1. occur when primary peristalsis fails to
move food into stomach
2. caused by distention of esophagus
3. continues until all food is emptied
4. initiated by intrinsic neural circuits in
esophageal myenteric nervous system
and reflexes transmitted through vagal
afferent fibers from the esophagus to the
medulla and back again to the esophagus
through vagal efferent fibers
5. musculature of pharynx and upper third
of esophagus is striated muscle controlled
by skeletal nerve impulses in
glossopharyngeal and vagus nerves
6. lower 2/3 is smooth muscle controlled by
vagus via myenteric nervous system
7. myenteric nerve plexus causes
swallowing in lower 2/3 in the absence of
vagus input
3. receptive relaxation of stomach
a. esophageal peristaltic wave moves toward
stomach
b. myenteric inhibitory neurons cause wave of
relaxation to precede the peristaltic wave
c. stomach and duodenum become relaxed as wave
reaches lower esophagus
4. function of lower esophageal sphincter (gastroesophageal sphincter)
a. circular muscle
91
b. 2-5 cm above juncture with stomach
c. normally tonically constricted
d. about 30 mm Hg pressure (mid-esophagus is relaxed)
e. receptive relaxation causes esophageal sphincter to relax
f. achalasia = failure of sphincter to relax
g. sphincter prevents reflux of stomach into esophagus
h. lower esophageal sphincter is aided by valve-like mechanism of
the short portion of the esophagus that lies below the
diaphragm
5. dysphagia
a. Nut-cracker esophagus
1. pressure
2. angina-like pain
b. diffuse spasm - single wave
c. Achalasia
1. neuromuscular disorder
2. lower esophageal sphincter fails to relax
d. megaesophagus
1. genetic abnormally
2. myenteric plexus fails
3. esophagus does not empty into stomach
II. Motor Functions of the Stomach
A. functional and anatomical regions
1. fundus & cardia
2. corpus (body)
3. antrum
4. pylorus
5. proximal region
6. distal region
B. storage of large quantities of food until the food can be processed in the
duodenum
92
1. food forms concentric circles in orad portion of stomach
2. newest food near esophagus, older food near lining of stomach
3. vagovagal reflex causes reduction in tone of stomach wall
4. stomach stretches to hold about 1.5 liters
5. tone remains low until limit is reached
C. mixing of food with gastric secretions until it forms chyme
1. leading contraction - forces food through pyloric sphincter
2. trailing contraction
a. causes pyloric sphincter to contract
b. promotes mixing & grinding of food
3. gastric glands - (this section is covered in next lecture on chap. 64)
a. secrete digestive juices
b. cover wall of stomach except lesser curvature
4. mixing waves = constrictor waves
a. occur when food is in stomach
b. begin in midportion of stomach
c. move toward antrum
d. rate:
1. 1/15-20 sec.
2. 0.5 cm/sec in corpus
3. 4 cm/sec. at terminal antrum
e. initiated by basic electrical rhythm
f. occur without action potentials
g. become most intense as they move toward antrum
h. peristaltic constrictor rings
1. force antral contents toward the pylorus
2. mix stomach contents
3. < 7mm object can be pass through pyloric sphincter
with leading contraction
4. > 7 mm objects washed out by migrating contraction
93
i. retropulsion = squirting of contents backward through the
peristaltic ring toward the body of the stomach due pressure of
the peristaltic ring and the contraction of the pyloric muscle
5. formation of chyme
a. food mixed with stomach secretions
b. murky, milky semifluid or paste
6. hunger contractions
a. intense contraction of stomach
b. rhythmical peristaltic contractions
c. in body of stomach
d. can cause 2-3 min. tetanic contraction
e. most intense in young healthy people with high
degree of GI tonus
f. increase with blood glucose
g. hunger pangs
1. pain in the pit of the stomach due to hunger contractions
2. begin 12 - 24 hrs. after last ingestion
3. most intense - 3-4 days in starvation
4. in starvation - gradually weaken over time
D. regulation of stomach emptying
1. volume of food - volume emptying
2. composition of food
3. physical state of the food eaten
a. liquid food empties at a faster rate
b. osmolarity - isotonic food is absorbed faster
c. acidity - acid of chyme will damage duodenum
d. caloric content
1. fat increases satiety
2. fat is the slowest emptied from the stomach
E. slow emptying of the food from the stomach into the small intestine
1. emptying is promoted by intense peristaltic contractions of
94
stomach antrum
a. pyloric pump - pumping action provided by peristaltic waves
b. 20% of contractions in stomach are intense, 80% are weak
c. intense contraction produce a force of 50-70 cm of water
pressure
d. the intensity of the waves determines the rate of stomach
emptying
2. opposed by varying degrees of resistance to the passage of
chyme at the pylorus
a. pylorus
a. distal opening of the stomach
b. 50-100% greater muscular thickness than antrum
c. continuous tonic contraction
d. pyloric circular muscle = pyloric sphincter
b. water and fluids pass through the pylorus with ease
c. food must mix in the chyme and become fluid before passage
through the pylorus
3. tonicity of pylorus is influenced by nervous and humoral signals form
the stomach and the duodenum
a. duodenum has greatest influence on stomach emptying
1. multiple nervous reflexes are initiated by food entering
the duodenum
2. initiated by the duodenal wall to stomach
3. slow or stop the stomach from emptying
4. initiated via 3 routes:
a. directly from the duodenum to the stomach
through the enteric nervous system in the
gut wall
b. through extrinsic nerves that go to the
prevertebral sympathetic ganglia and then back
95
through inhibitory sympathetic nerve fibers to
the stomach
c. probably to the a slight extent - through vagus
nerves to the brain stem - to inhibit normal
excitatory signals to stomach through vagi.
5. effects of these reflexes:
a. strongly inhibit antral propulsive contraction
b. increase slightly to moderately the tone of the
pyloric sphincter
b. weak gastric factors that promote emptying
1. food volume in stomach
2. stretching (not pressure)of gastric walls elicits myenteric
reflexes to excite pyloric pump and slightly inhibit the
pylorus
3. gastrin
a. hormone
b. secreted in response to digestive products
of meat
c. has potent effect to cause secretion of highly
acidic gastric juice by the stomach glands
d. mild to moderate stimulatory effects on motor
function of the stomach
e. activity of pyloric pump
f. pyloric sphincter
g. esophagus sphincter
h. relaxes ileocecal valve
F. factors that excite the enterogastric reflexes which are monitored
in the duodenum (approx. 12" long)
1. enteric nervous system
2. extrinsic nerves
a. prevertebral sympathetic ganglia
96
b. inhibitory effect
3. vagus
4. degree of distention of the duodenum
5. presence of irritation of the duodenal mucosa
6. degree of acidity of the duodenal chyme
a. reflex activated within 30 sec.
b. prevents movement of chyme into duodenum when
pH is < 3.5 - 4
7. degree of osmolality of the chyme
a. elicited by hypotonic or hypertonic solution
b. prevents rapid change in electrolyte concentrations in the
extracellular fluid during absorption
8. presence of certain breakdown products in the chyme - especially from
proteins and fats
G. hormonal feedback from the duodenum
1. fats - main stimulus
2. hormones carried through blood to stomach to inhibit activity of the
pyloric pump and increase contraction of the pyloric sphincter
3. fats are slower to be digested
4. cholecystokinin (CCK) - probably the most important
a. most powerful inhibitor
b. released from the mucosa of jejunum in response to fat
c. competitive inhibitor
d. blocks increased stomach motility caused by gastrin/acts in
opposition to gastrin
5. secretin
a. released from duodenal mucosa
b. stimuli = gastric acid
c. weakly decreases GI motility
6. gastric inhibitory peptide = GIP
a. released from upper small intestine
97
b. stimuli = fats and carbohydrates
c. inhibits gastric motility in some conditions
d. stimulates insulin secretion
H. summary of the control of stomach emptying
1. controlled moderately by stomach factors
a. degree of filling
b. excitatory effect of gastrin
2. controlled mainly by duodenum - enterogastric nervous system
feedback reflexes and hormonal feedback
a. too much chyme is in the small intestine
b. chyme is acidic, or contains unprocessed protein or fat
c. is hypotonic or hypertonic
d. irritation
3. stomach emptying is limited to by amount of chyme the small intestine
can process
III. Movements of the Small Intestine
A. mixing contractions
1. stretch of intestinal wall elicits localized concentric contractions
2. longitudinal length = 1cm
3. segmentation = set of contractions
4. frequency of segmentation is determined by frequency of slow wave in
intestinal wall (basic electric rhythm)
5. max. frequency in duodenum and proximal jejunum is 12/min
6. max. frequency in terminal ileum = 8-9 / min
7. atropine diminishes segmentation contractions
8. segmentation contractions are not effective w/o the enteric
nervous system
B. propulsive contractions
1. chyme is propelled by peristaltic waves
2. peristaltic waves occur throughout the small intestine
98
3. move analward @ 0.5 - 2.0 cm/sec
4. move faster in proximal and slower in terminal intestine
5. peristaltic waves are weak and die out after 3-5 cm
6. movement of chyme in small intestine = 1 cm/min
7. chyme requires 3-5 hrs. to move from pylorus to ileocecal valve
C. peristaltic activity
1. increased after a meal - due to chyme entering intestine & food
entering stomach
2. enhanced by gastroenteric reflex
3. enhanced by hormones:
a. gastrin
b. CCK
1. stomach motility
2. movement in small intestines
c. insulin
d. serotonin
4. inhibited by hormones:
a. secretin
b. glucagon
5. segmentation contractions also have propulsive effect
6. peristaltic rush:
a. intense irritation of intestinal mucosa
b. infectious diarrhea
c. powerful and rapid peristalsis
d. initiated by extrinsic nervous reflexes to ANS ganglia and brain
stem and back to gut and by direct enhancement of myenteric
plexus reflexes
e. powerful peristaltic contractions travel long distances
within minutes
7. migrating motor complex,(this is covered in the lecture on chapt. 62)
a. occurs many hours after eating or during fasting
99
b. recurs about every 90 minutes
c. moderately active peristaltic waves sweep slowly downward
along the stomach and small intestine
d. sweeps excess digestive secretions and debris into colon
e. begins in body of stomach and spreads through the ileum
f. 40 cm area of contraction moves @ 6-12 cm/min
g. lasts about 6-10 min
h. when one complex reaches ileum, another starts in stomach
8. muscularis mucosae
a. cause folds in intestinal mucosa
b. increase surface area
c. increase rate of absorption
d. contractions "milk" villi
e. contractions are initiated by local nervous reflexes in
submucosal plexus in response to chyme
D. function of the ileocecal valve
1. principal function - prevent backflow of fecal contents from the
colon into the small intestine
2. pressure in cecum forces valve closed - does not open after every meal
3. resist back pressure of 50 - 60 cm of water
4. ileocecal sphincter = thickened muscular coat
5. remains mildly constricted except after a meal (gastroileal reflex)
6. about 1500 ml of chyme into the cecum each day
E. feedback control of ileocecal sphincter
1. controlled by reflexes of cecum
2. distention of cecum intensifies contraction of ileocecal sphincter
3. irritant in cecum delays emptying (ex. inflamed appendix)
4. mediation of reflexes of cecum to ileocecal sphincter and ileum
a. myenteric plexus
b. extrinsic nerves - especially reflexes of the prevertebral
sympathetic ganglia
100
IV. Movements of the Colon
A. principal functions:
1. absorption of water and electrolytes - proximal 1/2
2. storage of fecal matter until expulsion - distal ½
B. movements:
1. mixing
a. large circular constrictions - segmentation
b. 2.5 cm in size
c. can constrict lumen of colon
d. haustrations
1. simultaneous contraction of circular and longitudinal
muscles
2. teniae coli = longitudinal strips of muscle
3. reach peak intensity in 30 sec.
4. last about 1 min.
5. provide forward movement
e. fecal matter is slowly dug into and rolled over in order to
maximize expose to wall of large intestine.
f. allows for maximum absorption
e. only 80-200 ml of chyme is lost in feces
2. propulsive
a. haustral contractions - slow analward movement
1. occurs from ileocecal valve to transverse colon
2. 8-15 hrs. to move chyme from ileocecal valve through
transverse colon
b. mass movements
1. occurs from transverse colon to sigmoid
2. occur 1-3 times / day
3. occur most abundantly for about 15 min. during 1st hr.
after eating breakfast
101
4. modified type of peristalsis
a. constrictive ring occurs at a distended or irritated
point in colon (usually transverse colon)
b. 20+ cm. of colon distal to constriction contract
as unit - forcing fecal material in mass down the
colon
c. contraction intensifies for 30 sec.
d. after 2-3 min, another mass movement occurs
e. mass movements continue to occur for
10-30 minutes
f. mass movements move feces into rectum
stimulating desire for defecation
5. initiation of mass movements;
a. gastrocolic reflex
b. duodenocolic reflex
c. reflexes result from distention of stomach
and duodenum
d. reflexes are dependent on extrinsic nerves
of ANS
e. irritation (ex. ulcerative colitis) stimulates
constant mass movements
f. intense parasympathetic stimulation
g. overdistention of a segment of the colon
C. defecation reflex
1. controlled by the nerves of S2, S3, S4,
2. rectum is usually empty
3. movement of feces into rectum initiates desire for defecation
4. movement of feces through is prevented by :
a. internal anal sphincter - thickened smooth muscle inside anus
b. external anal sphincter - striated voluntary muscle surrounding
internal sphincter and extending distally
102
1. controlled by fibers in pudendal nerve
2. under voluntary, conscious control
c. Valsalva
1. deep breath
2. contraction of abdominal muscles
5. reflexes:
a. gastrocolic reflex and duodenocolic reflex - moves contents to
colon
b. intrinsic reflex
1. mediated by local enteric nervous system
2. relatively weak
3. functions through myenteric plexus
c. parasympathetic defecation reflex
1. sacral segments of spinal cord
2. through pelvic nerves
3. powerful reflex
4. overridden by toilet-training
V. Other Autonomic Reflexes that Affect Bowel Activity
A. peritoneointestinal reflex
1. irritation of peritoneum
2. strongly inhibits excitatory enteric nerves
3. can cause intestinal paralysis (especially with peritonitis)
B. renointestinal reflex - kidney and bladder irritation
C. vesicointestinal reflex - kidney and bladder irritation
D. somatointestinal reflex - irritation of skin over the abdomen
E. these reflexes:
1. initiated by sensory signals that pass to prevertebral sympathetic
ganglia or spinal cord and transmitted through sympathetic nervous
system back to the gut
2. all inhibit gastrointestinal activity - often very strong
103
104
105
Secretory Functions of the Alimentary Tract
Physiology III, Tri 4
Guyton & Hall, Chapt. 64
I. General principles of alimentary tract secretion
A. anatomical types of glands
1. mucous cells = goblet cells
a. single-cell mucous glands
b. surface epithelium
c. respond to epithelial stimulation
d. extrude mucus for lubrication to protect surfaces
2. pits - invaginations of the epithelium
a. crypts of Lieberkühn - small intestine
b. deep
c. contain specialized secretory cells
3. tubular glands - stomach and upper duodenum
4. complex glands:
a. compound acinous glands
1. salivary glands
2. pancreas
b. liver
c. provide secretions for digestion or emulsification of food
d. lie outside the walls of alimentary tract
e. contain millions of acini lined with secreting glandular cells
f. acini feed into system of ducts that empty into alimentary tract
B. stimulation of alimentary tract glands
1. mechanical presence of food
2. enteric nervous system
a. tactile stimulation
b. chemical irritation
106
c. distention of gut wall
3. nervous reflexes stimulate both mucous cells on the epithelial surface
and deeper glands in the mucosa
C. ANS stimulation of secretion
1. parasympathetic stimulation
a. increase rate of secretion
b. upper portion of tract
1. salivary glands
2. esophageal glands
3. gastric glands
4. pancreas
5. Brunner's glands in the duodenum
c. innervated by vagus & other cranial parasympathetic nerves
d. distal portion of large intestine
e. innervated by pelvic parasympathetic nerves
f. (secretion in the remainder of the small intestine and in the 1st
2/3 of the large intestine occurs mainly in response to local
neural and hormonal stimuli)
2. sympathetic stimulation
a. slight to moderate increase in secretion in some parts
b. constriction of blood vessels - leads to reduced secretion from
glands
D. regulation of glandular secretion by hormones
1. stomach and intestines
2. from gastrointestinal mucosa
3. stimulated by the presence of food in gut lumen
4. carried by blood to glands
5. increases output of gastric juice and pancreatic juice
6. hormonal stimulation causes constriction of gallbladder to empty bile
7. gastrointestinal hormones are polypeptides or polypeptide derivatives
E. basic mechanism of secretion by glandular cells
107
1. all are not known
2. nutrient material needed for formation of the secretion must diffuse or
be actively transported from the capillary into the base of the glandular
cell
3. many mitochondria located inside the cell near its base use oxidative
energy for formation of adenosine triphosphate (ATP)
4. energy from the ATP, along with appropriate substrates provided by
the nutrients, is them used for synthesis of the organic substances; this
synthesis occurs almost entirely in the endoplasmic reticulum and
Golgi complex. The ribosomes adherent to the reticulum are
specifically responsible for formation of the proteins that are to be
secreted.
5. secretory materials are transported through the tubules of the
endoplasmic reticulum, passing in about 20 min. all the way to the
vesicles of the Golgi complex, which lies near the secretory ends of the
cells
6. in the Golgi complex, materials are modified, added to, concentrated,
and discharged into the cytoplasm in the form of secretory vesicles,
which are stored in the apical ends of the secretory cells
7. vesicles remain stored until nervous or hormonal control signals cause
the cells to extrude the vesicular contents through the cell's surface exocytosis
F. water and electrolyte secretion
1. nerve stimulation has a specific effect on the basal portion of the cell
membrane to cause active transport of chloride ions to the interior
2. resulting increase in electronegativity induced inside the cell by excess
chloride ions then causes positive ions also to move to the interior of
the cell
3. excess of both negative and positive ions inside the cell creates an
osmotic force that pulls water to the interior - increasing the hydrostatic
pressure inside the cell and causing the cell itself to swell
108
4. pressure in the cell results in minute ruptures of the secretory border of
the cell and causes flushing of the water, electrolytes, and organic
materials out of the secretory end of the glandular cell and into the
lumen of the gland
G. lubricating & protective properties of mucus and its importance in the GI tract
1. mucus
a. thick secretion composed mainly of water, electrolytes, and
glycoproteins
b. adherent qualities
c. prevents contact of food particles with the mucosa
d. low resistance for slippage - particles slide
e. causes adherence to fecal matter
f. strongly resistant to digestion by the GI enzymes
g. amphoteric properties - pH buffer
h. contain bicarbonate ions - neutralizes acids
2. mucus allows easy slippage of food along GI tract and prevents
excoriative or chemical damage to epithelium
II. Secretion of Saliva
A. principal glands (tubuloalveolar)
1. parotid
secretory end-pieces
serous cells
2. submandibular
3. sublingual
intercalated duct
4. buccal
striated duct
5. lingual glands
mucous cells
excretory duct
6. other glands
B. daily rate of secretion = 1000 - 1500 ml
C. types of saliva secretion
1. serous
a. ptyalin
1. an -amylase
109
2. salivary amylase
b. for digestion of starches
c. produced by parotid, submandibular and sublingual glands
2. mucous
a. mucin (glycoprotein)
b. for lubrication
c. produced by buccal, submandibular and sublingual glands
Mucous Cells
3. muramidase
a. lysozyme
b. acts on muramic acid of the cell wall
c. bacteria can not maintain osmotic pressure
Serous Cells
** 4. lingual lipase
a. fat digesting enzyme
b. digest milk fat
c. important in infants
110
Na
HCO3ClK+
5. lactoferrin
a. protein
b. binds with iron
6. epidermal growth factors
7. immunoglobulin - IgA
8. ABO blood factors (in persons who are secretors)
D. pH of saliva = 6-7.4 (excellent for ptyalin activity)
E. ions in saliva:
1. potassium (30 mEq/L, 7X plasma)
2. bicarbonate ion (50 - 70 mEq/L, 2-3X plasma)
3. sodium & chloride (15 mEq/L, 1/7 - 1/10 of plasma)
4. concentration of ions change with maximal salivation and
aldosterone secretion
F. stages of salivary secretion:
1. stage 1 - from acini
a. secrete primary secretion
b. contains ptyalin and/or mucin
c. ions - similar to extracellular fluid
2. stage 2 - from salivary ducts (amylase)
a. Na+ actively reabsorbed from all salivary ducts
b. K+ actively exchanged for sodium
c. chloride passively reabsorbed
111
d. bicarbonate ion secreted by ductal epithelium
End
Piece
ClHCO3Na+
K+
3. oral hygiene
a. flow of saliva helps to wash away bacteria and food
b. contains antibacterial agents:
1. thiocyanate ions
2. proteolytic enzymes - ex. lysozyme
3. protein antibodies
G. nervous regulation of salivary secretion
1. salivary glands controlled mainly by parasympathetic nervous signals
from the superior and inferior salivatory nuclei of brain stem
a. at juncture of medulla and pons
b. excited by taste and tactile stimuli
c. excitation from tongue, mouth and pharynx
d. "sour taste" = "sapid taste" & smooth objects copious
secretion of saliva
112
e. rough objects reduce/inhibit salivation
2. salivatory nuclei and appetite area of anterior hypothalamus effect
salivation
3. reflexes from stomach and upper intestines
a. irritating foods
b. nausea
c. GI abnormality
4. sympathetic stimulation BF saliva
a. less powerful than parasympathetic
b. originates from the superior cervical ganglia
c. travels along blood vessels to salivary glands
5. blood supply to glands
a. acts as secondary factor
b. secretion requires nutrition
c. parasympathetic nerve signals dilate blood vessels
d. saliva dilates blood vessels
e. kallikrein
1. dilates vessels
2. splits a blood protein to bradykinin (vasodilator)
H. functions of saliva:
1. chewing
2. swallowing
3. speech
4. dissolves components of food
5. enhances taste
6. cleans oral tissue (brushing teeth is still necessary)
III. Esophageal Secretion
A. mucoid
B. provide lubrication for swallowing
C. simple mucous glands in body of esophagus
113
D. compound mucous glands in the gastric end and initial portion of esophagus
1. prevents mucosal excoriation (initial segment)
2. protect esophageal wall from digestion by gastric
juices ( distal segment)
E. initiates starch digestion
F. aids in excretion of heavy metals
1. iron
2. lead
3. others
IV. Gastric Secretion
A. mucous-secreting cells
1. line entire surface of stomach between glands
2. secret viscid mucus - mainly insoluble
3. coats mucosa with gel layer of mucus
4. protection for stomach - lubrication for food
5. alkaline pH
6. stimulus:
a. food
b. irritation of mucosa
114
Cells within the Gastric Glands and their Secretory Products
Gland Area
Cell
Secretory Products
Cardiac
Mucous
Mucus, HCO3-, pepsinogens
(group II)
Oxyntic
Pyloric
Endocrine
Parietal (oxyntic)
Chief
Mucous neck
Enterochromaffin
Endocrine
Mucous
G cell
Enterochromaffin
Other endocrine
HCL, intrinsic factor
Pepsinogens (groups I and II)
Mucus, HCO3 -, pepsinogens
(group I and II)
Serotonin
Mucus, HCO3-, pepsinogens
(group II)
Gastrin
Serotonin
B. tubular glands
1. oxyntic (gastric) glands - body and fundus of stomach (80% of
stomach)
a. acid forming
b. secrete HCl, pepsinogen, intrinsic factor and mucous
c. cell types:
1. mucous neck cells
a. mucus
b. pepsinogen
2. peptic (chief) cells
a. pepsinogen
1. several different types
115
2. activated by HCl
3. forms pepsin
a. active proteolytic enzyme
b, active in high acid environment
c. pH 1.8 -3.5 optimum
d. > pH 5, is inactive
e. necessary for protein digestion
Gastric
Pit
Surface
Mucous Cells
Oxyntic
Cell
Isthmus
Mucous Neck
Cells
Neck
Endocrine
Cell
Base
Chief Zymogenic
Cells
3. parietal (oxyntic) cells
a. HCL
1. pH = 0.8
2. formed in membranes of canaliculi
3. fig. 64-6
b. intrinsic factor - B12
116
d. other enzymes:
1. gastric lipase
a. = tributyrase
b. acts on butterfat
2. gastric amylase
a. digestion of starches
b. minor role
3. gelatinase - liquefy proteoglycans in meats
4. intrinsic factor
a. essential for vit. B12 absorption in ileum
b. deficiency = pernicious anemia
2. pyloric glands - antral portion of stomach
a. mucous (lubrication)
b. pepsinogen
c. gastrin - controls gastric secretion
d. cell types:
1. structurally similar to oxyntic glands
2. few peptic cells
3. no parietal cells
4. mostly mucous cells
C. regulation of gastric secretion by nervous and hormonal mechanisms
1. acetylcholine
a. bind with receptor on secretory cells
b. excites all secretory cells in gastric glands
c. released at parasympathetic nerve endings with vagi stimulation
2. gastrin
a. bind with receptor on secretory cells
b. stimulates secretion of acid by parietal cell
c. little effect on other cells
d. secreted by gastrin cells (G cells) in pyloric glands
e. large peptide
117
1. 6 different molecules
2. 4 AA at end are active site
f. secreted in 2 forms:
1. G-34
a. large form
b. contains 34 amino acids
2. G-17
a. smaller form
b. contains 17 amino acids
c. most abundant form
g. absorbed into the blood
h. carried to oxyntic glands in body of stomach
i. stimulates parietal cells (strongly) and peptic cells (weakly)
j. increases HCl secretion by parietal cells
k. stimulated by vagi
l. may HCO3- release from liver and pancreas
m. gastric motility
n. pressure of LES
o. open ileocecal valve
3. histamine
a. bind with receptor on secretory cells
b. stimulates secretion of acid by parietal cell
c. little effect on other cells
d. amino acid derivative
e. formed continually in gastric mucosa
f. in the presence of acetylcholine will enhance acid secretion
g. necessary cofactor for exciting significant acid secretion
h. type H2 receptors on parietal cells
4. other substances that stimulate gastric secretions:
a. amino acids
b. caffeine
c. alcohol
118
d. food in stomach - causing distention
Neurocrine
Paracrine
Endocrine
Histamine
H2
ACH
Gastrin
Atropine
Ca++
Cimetidine
Proglumide
ATP
camp
pK
protein
ADP
protein
H
5. nervous stimulation:
a. ½ of signals originate in the dorsal motor nuclei of vagi
1. pass by way of vagus nerves
2. to enteric nervous system
119
3. then to gastric glands
4. release ACH
b. ½ of signals are generated by local reflexes
1. occur within the wall of stomach
2. release ACH
c. in pyloric glands
1. intermediate neuron serves as final path
2. secretes gastrin-releasing peptide as neuro-transmitter
3. probably the peptide bombesin
6. signals originate in
a. brain
b. stomach
1. long vagovagal reflexes
a. from stomach mucosa to brain stem
b. back to stomach through vagus nerves
2. short reflexes
a. originate locally
b. transmitted through local enteric nervous system
7. stimuli:
a. distention of stomach
b. tactile stimuli on surface of stomach mucosa
c. chemical stimuli
1. amino acids
2. peptides
3. acid
d. when acetylcholine, gastrin, and histamine are all present,
copious amounts of acid are secreted
D. regulation of pepsinogen secretion
1. stimuli:
a. stimulation of peptic cells by ACH from vagus nerves
& enteric nerves
120
b. stimulation of peptic secretion by acid in stomach (indirectly)
c. acid pepsinogen secretion
2. when pH falls below 3.0 , stimulation for gastric secretion becomes
blocked pepsinogen secretion
3. pH 3.0 = optimal pH for peptic enzymes
E. phases of gastric secretion (phases fuse together)
1. cephalic phase
a. occurs before food enters the stomach
b. results from:
1. sight
2. smell
3. thought
4. taste
c. appetite stimulation
d. neurogenic signals originate in cerebral cortex or appetite
centers of amygdala or hypothalamus
e. transmitted through the dorsal motor nuclei of vagi to stomach
f. accounts for about 20% of gastric secretion
2. gastric phase
a. food in stomach excites:
1. vagovagal reflexes
2. local enteric reflexes
3. gastrin mechanism
b. accounts for 70% of gastric secretion
3. intestinal phase
a. food in small intestine stimulates stomach to secret gastric juice
b. duodenal mucosa secretes gastrin in response to distention or
chemical stimuli
c. amino acids and other hormones reflexes play minor roles in
secretion of gastric juice
121
Stimulation of Gastric Acid Secretion
Phase
Stimulus
Pathway
Cephalic
Chewing,
Swallowing
vagus n. to:
1. Parietal
cells
2. G cells
Gastric
Gastric
Intestinal
Protein
digestion
products in
Stimulus to
parietal cell
Local and
vagovagal
reflexes to:
1. Parietal
cells
2. G cells
ACH
Gastrin
ACH
Gastrin
1. Intestinal G
Gastrin
cells
2. Intestinal enterooxyntin
F. inhibition of gastric secretion by intestinal factors
1. chyme stimulates gastric secretion during intestinal phase of secretion
and inhibits during gastric phase
a. presence of food in small intestine initiates an
enterogastric reflex
b. reflex inhibits stomach secretion that is initiated by:
1. distention of small bowel
2. presence of acid in upper intestine
3. presence of protein breakdown products
4. irritation of mucosa
122
2. presence of acid, fat, protein breakdown products, hyperosmotic or
hypo-osmotic fluids, or irritating factor in upper small intestine causes
release of several hormones:
a. secretin - opposes stomach secretion
b. gastric inhibitory peptide
c. vasoactive intestinal polypeptide
d. somatostatin
3. inhibition of gastric secretion by intestinal factors slows the release of
chyme from the stomach when small intestine is already filled
4. during interdigestive period small amount of nonoxyntic gastric juice
is secreted
a. mainly mucus
b. contains little pepsin
c. almost no acid
d. increases with emotional stimuli
G. chemical composition
1. gastrin
a. polypeptide
b. terminal five amino acids
same as cholecystokinin
c. activity resides in terminal 4 amino acids
2. cholecystokinin
a. polypeptide
b. terminal five amino acids same as gastrin
c. activity resides in terminal 8 amino acids
3. secretin
a. polypeptide
c. all the amino acids in secretin are essential
123
4. enzymes -secreted in inactive or zymogenetic form
a. pepsin
1. proteolytic enzyme
2. pepsinogen (zymogenetic) major enzyme
3. pepsinogen HCl pepsin
4. found in peptic and mucous cells of the gastric glands
5. pepsinogen is activated by HCl
6. pH < 3.0 is needed for activation of pepsinogen
b. gelatinase - helps to liquefy
c. gastric lipase
1. tributyrase (AKA)
2. acts on tributyrin (=butterfat)
3. does not breakdown triglycerides
d. gastric amylase - has minor role in digestion of starch
e. renin
1. chymosin (AKA)
2. not the same as in the kidney
3. not part of the human system
4. originally thought to be in the human GI tract
5. casein (a protein) paracasein
6. HCl produces curdling of mile in humans in order to
prolong time of in the stomach for protein digestion
124
Mechanisms for Inhibition of Gastric Acid Secretion
Region
Stimulus
Mediator
Inhibit
Gastrin
Release
Antrum
Acid (pH<3.0)
None, direct
+
Duodenum Acid
Secretin
Bulbogastrone
Nervous reflex
+
+
Duodenum Hyperosmotic
Jejunum solutions
Unidentified
enterogastrone
Fatty acids,
Gastric
+
inhibitory peptide
Monoglycerides Cholecystokinin
+
Unidentified enterogastrone
Inhibit
Acid
Secretion
+
+
+
+
+
+
+
V. Pancreatic secretion
A. pancreas
1. weighs about 100 gms
2. "sweet breads" = delicacy
3. secretes 1200 - 1500 ml/day of clear, odorless fluid
4. 7.7 - 8.2 pH, alkaline for the neutralization of acid form the GI tract
5. function:
a. endocrine
1. insulin
2. glucagon
3. somatostatin
b. exocrine - GI secretions
125
6. watery HCO- solution
a. CO2 is taken up by pancreas and mixed with H2O
b. Na and H move counter
c. Na is added to bicarb solution
B. pancreatic enzymes - secreted by acini
1. proteolytic enzymes:
a. synthesized in the inactive forms trypsinogen,
chymotrypsinogen and procarboxypolypeptidase
b. become active in the intestinal tract
c. trypsinogen
1. endopeptidase activated by enterokinase (secreted
by intestinal mucosa) and trypsin to form trypsin
Trypsinogen
Enterokinase
Proelastase
Chymotrypsinogen
Trypsin
Elastase
Procarboxypeptidase
Chymotrypsin
Carboxypeptidase
d. proelastase (endopeptidase)
e. chymotrypsinogen
1. endopeptidase
126
2. is activated by trypsin to from chymotrypsin
f. procarboxypolypeptidase
1. A&B forms
2. is activated by trypsin to form carboxypolypeptidase
3. exopeptidase
g. trypsin
1. most abundant
2. split whole and partially digested proteins into peptides
but does not cause release of individual amino acids
g. chymotrypsin
1. split whole and partially digested proteins into peptides
but do not cause release of individual amino acids
h. carboxypolypeptidase
1. split some peptides into individual amino acids
i. elastases
j. nucleases
k. trypsin inhibitor
1. stored in cytoplasm of glandular cells
2. prevents activation of trypsin
3. prevents digestion of pancreas (autodigestion)
4. w/o trypsin inhibitor, pancreatic secretions digest the
entire pancreas within a few hours = acute pancreatitis
a. often lethal
b. shock
c. not lethal - pancreatic insufficiency
l. ribonucleases & deoxyribonucleases
1. breaks down RNA & DNA
2. prevents ingestion & absorption of
DNA & RNA supplements
2. pancreatic amylase
a. digests carbohydrates
127
b. hydrolyzes
1. starches
2. glycogen
3. other carbohydrates
4. not cellulose
c. forms disaccharides and few trisaccharides
3. pancreatic fat digestion
a. pancreatic lipase
1. main enzyme for fat digestion
2. hydrolyzes fat into fatty acids and monoglycerides
3. needs bile and calcium ions
4. main enzyme that attacks fat
b. cholesterol esterase
1. main enzyme for fat digestion
2. hydrolyzes cholesterol esters
c. phospholipase
a. main enzyme for fat digestion
b. splits fatty acids from phospholipids
****
c. only non-proteolytic enzyme that requires
activation by trypsin
C. secretion of bicarbonate ions
1. secreted by epithelial cells of small ductules and larger ducts leading
from the acini
2. mechanism:
a. CO2 diffuses to interior cell from blood
b. CO2 combines with water to form carbonic acid ( in the
presence of carbonic anhydrase)
c. carbonic acid dissociate into bicarbonate ion and hydrogen ions
d. bicarbonate ions are actively transported into lumen of duct
e. hydrogen ions are exchanged with sodium ions in the blood
128
f. sodium ions are transported into pancreatic duct - providing
electrical neutrality for secreted bicarbonate ions
g. movement of sodium and bicarbonate ions from blood to lumen
creates osmotic gradient
h. water moves into pancreatic duct to create isosmotic
bicarbonate solution
D. regulation of pancreatic secretion
1. stimuli:
a. diet - change in diet may effect secretions
b. acetylcholine
1. released from parasympathetic vagus nerve endings
2. released from other cholinergic nerves in enteric
nervous system
3. stimulate acinar cells more than ductal cells
c. cholecystokinin
1. released by duodenal and upper jejunal mucosa
2. stimulated by the presence of food
3. stimulate acinar cells more than ductal cells
d. secretin
1. released by duodenal and upper jejunal mucosa
2. stimulated by highly acid food in small intestine
3. stimulates large quantities of sodium bicarbonate by
ductal epithelium
4. almost no stimulation of enzyme secretion
2. multiplicative effects - the effects of stimuli occurring simultaneously
is multiplied vs. the stimuli occurring alone
E. phases of pancreatic secretion - same as gastric secretion
1. cephalic
a. vagus nerve
b. smell, sight, thought are stimuli
129
c. same nervous signals that cause secretion in the stomach
d. acetylcholine released by vagal nerve endings
e. produce 20% of total pancreatic secretion
2. gastric
a. same nervous (vagus) signals that cause secretion
in the stomach
b. acetylcholine released by vagal nerve endings
c. produce 5-10% of total pancreatic secretion
3. intestinal
a. main control
b. stimulated by chyme entering intestine
** c. secretin (important one)
1. stimulates copious amounts of secretion
2. polypeptide with 27 a.a., mol. wt. = 3400
3. present in S cells of mucosa of upper small intestine
4. prosecretin = inactive form
5. chyme of < pH 4.5 entering the duodenum stimulates
release and activation of secretin
6. HCl, major stimulator of secretin release
7. secretin enters blood and travels to pancreas
8. causes pancrease to secrete bicarbonate ion in water
and sodium fluid with few enzymes
9. as more acid enters the duodenum, more bicarb is
released
10. provides neutral or slightly alkaline environment for
optimum pancreatic enzyme activity
d. cholecystokinin stimulates enzyme secretion
1. polypeptide with 33 amino acids
2. stimulated by the presence of food in the upper
small intestine
130
a. proteoses and peptones - protein breakdown
products
b. long-chain fatty acids
c. HCl
3. released from I cells in the mucosa of the duodenum
and upper jejunum
4. travels via the blood to pancreas
5. stimulates secretion of large quantities of digestive
enzymes by the acinar cells
6. accounts for 70 - 80% of pancreatic enzyme secretion
after a meal
VI. Secretion of Bile by the Liver
A. bile
Bile Salts = steroid acids
precursor = cholesterol
cholic acid
chenodeoxycholic acid
glycine or taurine
glycocholic acid
taurocholic acid
1. secreted @ of 600-1200 ml/day
2. contains:
a. no digestive enzymes
b. water
131
c. bile salts
d. bilirubin
e. cholesterol
f. fatty acids
g. lecithin
h. sodium
i. potassium
j. calcium
k. chloride
l. bicarbonate ion
3. components of bile become more concentrated with secretion
4. starts to empty about 30 minutes after a meal
5. purpose:
a. production of micelles for aiding absorption
b. fat digestion
1. emulsification of large fat particles - increase
surface area
2. transport and absorption of digested fat end products via
micelles to and through intestinal mucosal membrane
c. excretion of blood waste products
1. bilirubin - end-product of hemoglobin destruction
2. cholesterol
B. stages of bile secretion
1. initial portion
a. secreted by liver hepatocytes
b. contains large amounts of bile acids, cholesterol, and
organic constituents
c. secreted into the minute bile canaliculi
2. second stage
a. bile flows peripherally toward the interlobular septa
b. canaliculi empty into terminal bile ducts and them larger ducts
132
c. bile flows to hepatic duct and common bile duct
d. bile empties into duodenum or is diverted to gallbladder
via cystic duct
e. as bile flows through ducts second portion is added
1. watery
2. sodium and bicarbonate ions secreted by secretory
epithelial cells lining ductules
3. increases bile by 100%
4. stimulated by secretin
C. storage and concentration of bile
1. continual secretion of bile is stored in the gallbladder until
needed in the duodenum
2. maximum volume of gallbladder is 30-60 ml
3. up to 12 hours of bile secretion can be stored in the gallbladder
4. gallbladder concentrates bile that is stored
5. bile constitutes:
a. bile salts - accounts for half of total solutes
b. bilirubin
c. cholesterol
d. lecithin
e. electrolytes of plasma
6. in the concentrating process of the gallbladder, large portions of
electrolytes (except calcium ions) are reabsorbed by the gallbladder
mucosa
D. emptying of the gallbladder
1. stimulated by food in upper GI tract
2. rhythmical contractions occur in the wall of the gallbladder
3. sphincter of Oddi relaxes
a. cholecystokinin causes relaxation
b. peristaltic waves from gallbladder
c. relaxation phase of intestinal peristaltic waves
133
4. cholecystokinin - most potent stimulus of gallbladder contractions
5. stimulated by ACH-secreting nerve fibers from vagi and enteric
nervous system
6. in the presence of fat, the gallbladder will empty in about 1 hour
7. 90% of all bile is reabsorbed in distal ilium
E. bile salts
1. 0.6 grams of bile salts formed daily
2. cholesterol, from diet or formed by the liver, is precursor of bile salts
3. actions of bile salts:
a. detergent action on fat particles
1. decreases surface tension
2. allows for agitation to break fat globules
3. emulsifying or detergent function
b. help with absorption
1. fatty acids
2. monoglycerides
3. cholesterol
4. other lipids
5. form micelles
F. secretion of cholesterol; most common gallstone formation
1. bile salts are formed in the hepatic cells from cholesterol
2. 1-2 gm/day cholesterol is secreted into the bile
3. cholesterol is insoluble in water
4. in the presence of bile salts and lecithin, cholesterol is converted into
micelles, which are soluble
5. gall stones:
a. precipitated cholesterol
b. too much water absorption from bile
c. too much absorption of bile salts and lecithin from bile
d. inflammation of the epithelium of the gallbladder (ex. infection)
e. increased cholesterol due to high fat diet &/or no-fat diet
134
VII. Secretions of the Small Intestine
A. Brunners glands
1. compound mucous glands
2. located in first few centimeters of duodenum
3. mainly between the pylorus and the papilla of Vater
4. secrete alkaline mucus (bicarbonate ions - neutralize acid)
5. stimulated by:
a. tactile stimuli or irritation of mucosa
b. vagal stimulation
c. gastrointestinal hormones (mainly secretin)
d. secretin is major stimulus for Brunner's glands
6. function - protection of the duodenal wall from digestion by
gastric juice
B. Crypts of Lieberkhn
1. small pits
2. located throughout small intestine
3. lie between the intestinal villi
4. covered with epithelium containing 2 cell types:
a. goblet cells
1. secrete mucus
2. protect intestinal surfaces
b. enterocytes
1. secrete water and electrolytes (in the crypts)
2. reabsorb water and electrolytes with the end products of
digestion (over the surfaces of the villi)
5. secretions are formed by enterocytes of the crypts @ 1800 ml/day
6. secretions are almost pure extracellular fluid with pH of 6.5 - 7.5
7. secretion do not contain enzymes
8. fluid from crypts to villi supplies a watery vehicle for absorption
9. mechanism of secretion:
135
a. active secretion of chloride into crypts
b. active secretion of bicarbonate ions
c. formation of electrical drag of sodium ions
d. osmotic movement of water
C. enzymes of the small intestine
1. final digestion occurs by membrane bound enzymes
2. peptidases
3. enzymes for splitting disaccharides into monosaccharides:
a. sucrase
b. maltase
c. isomaltase = dextrinase
d. lactase
4. intestinal lipase
5. glucoamylase - breaks maltoligosaccharides
6. tripeptidases
7. dipeptidase
8. lie in brush border
9. catalyze hydrolysis of food on the outside surface of the microvilli
before absorption - absorption - provides aqueous solution
for absorption
10. lifespan of intestinal epithelia cell = 5 days
VIII. Secretions of the Large Intestine
A. has many crypts of Lieberkhn with many goblet cells
B. no villi
C. almost no enzymes
D. epithelial cells are mostly mucous cells that secrete only mucus
E. mucus - main secretion
1. protects against excoriation
2. large amounts of bicarbonate ions
136
3. regulated by tactile stimulation of mucous cells and local nervous
reflexes to mucous cells in crypts of Lieberkhn
4. secretion with parasympathetic (with extreme parasympathetic
stimulation, ropy mucus bowel movement can occur @ of 1 every
30 min)
5. protects bowel from bacterial activity and provides adherent medium
for fecal matter
F. irritation (enteritis)
1. secretion of large quantities of water and electrolytes with normal
alkaline mucus
2. acts to dilute irritating factors and cause rapid movement of feces
toward anus
3. diarrhea - protective mechanism; loss of large quantities of water and
electrolytes as irritant factor is washed away
137
Factors Affecting Gallbladder Emptying & Bile Synthesis & Secretion
Phase of
Digestion
Stimulus
Mediating Factor
Response
Cephalic
taste and smell
of food; food in
mouth and
pharynx
Impulses in branches
of vagus nerve;
Gastrin?
rate of
gallbladder
emptying
Gastric
gastric
distension
impulses in branches
of vagus nerve:
Gastrin?
rate of
gallbladder
emptying
Intestinal
fat digestion
products in
duodenum
cholecystokinin
acid in
duodenum
secretin
rate of
secretion of
bicarbonaterich fluid by the
bile duct
epithelium (this
effect strongly
potentiated by
cholecystokinin)
Absorption of
bile acids in
the distal part
of ileum
High concentration
of bile acids in portal
blood
stimulation of
bile acid secretion
inhibition of bile
acid synthesis
low rate of
release of bile
low concentration of
bile acids in portal
stimulation of
bile acid
synthesis;
inhibition of bile
acid secretion
Interdigestive
rate of
bladder emptying;
rate of bile acid
secretion
138
139
Digestion and Absorption in the Gastrointestinal Tract
Physiology III, Tri 4
Guyton & Hall, Chapt. 65
I. Digestion of Various Foods
A. classification of foods (except vitamins and minerals)
1. carbohydrates
2. fats
3. proteins
B. carbohydrates
1. most are polysaccharides or disaccharides
2. monosaccharides bound to one another by condensation
(H+ removed from one of the monosaccharides and a OH- removed
from the next one)
3. hydrolysis - return of the hydrogen and hydroxyl ions to the
polysaccharides and separation of the monosaccharides
digestive enzyme
R'' - R' + H2O
R''OH + R"H
C. fats
1. triglycerides
a. neutral fats
b. 3 fatty acid + glycerol (-3 molecules of water)
2. digestion
a. addition of water to triglyceride molecule
b. splitting of fatty acid away from the glycerol
c. hydrolysis
D. proteins
1. amino acids with peptide linkages
2. bound by condensation
140
3. digestion is by hydrolysis
E. chemistry of digestion
1. three types of food
2. hydrolysis
3. enzymes
a. all are proteins
b. secreted by GI glands
II. Digestion of Carbohydrates (CHO)
A. CHO intake
1. 280 gm / day
2. varies widely
B. sources of CHO
1. sucrose
a. disaccharide
b. sugar cane
2. lactose
a. disaccharide
b. milk sugar
3. starches
a. large polysaccharides
b. found in nonanimal food (grains)
c. largest source of CHO; > ½ of all CHO
4. other sources:
a. amylose
b. glycogen
1. from meat
2. degrades quickly with ingestion in the
presence of -amylase
a. maltose (most common product)
b. maltotriose
141
c. limit dextrins
3. highly branched
-amylase
maltose
glycogen maltotriose
c. alcohol
-limit dextrins
d. lactic acid - buttermilk, yogurt
e. pyruvic acid
f. pectins
g. dextrins
1. oligosaccharide
2. has branched point
3. 1-4, 1-6
produces branch
h. derivatives in meats
i. cellulose
1. not a food source for humans
2. no enzymes for breakdown - no cellulase
C. digestion of CHO in the mouth and stomach
1. mouth - saliva
a. ptyalin = -amylase
b. secreted by parotid glands
c. hydrolyzes starch into the disaccharide maltose and glucose
polymers
d. about 5% of starches are hydrolyzed before swallowing
2. stomach
a. digestion continues in body and fundus for up to 1 hr.
b. food is mixed with stomach secretions
c. acidic gastric secretions block activity of salivary amylase
d. salivary amylase is inactive when pH is < 4.0
e. 30 - 40% of starch is hydrolyzed before mixing with
stomach acids
D. digestion by pancreatic amylase
1. pancreatic secretion contain large amounts of -amylase
2. identical function as salivary -amylase - but more powerful
142
3. 15 - 30 min. after chyme enters duodenum almost all starches are
digested
4. starches are converted to:
a. maltose
b. glucose polymers (small amount)
c. conversion takes place in the duodenum and upper jejunum
E. hydrolysis by the intestinal epithelial enzymes
1. enzymes of the enterocytes lining the villi:
a. lactase
b. sucrase
c. maltase
d. -dextrinase
e. all of the above can split lactose, sucrose, maltose, & other
glucose polymers into their constituent monosaccharides
f. enzymes are located in the membranes of the microvilli brush
border of the enterocytes
g. disaccharides are digested as they come in contact with the
membrane
h. lactose 1 galactose + 1 glucose
i. sucrose 1 fructose + 1 glucose
j. maltose & glucose polymers glucose
k. monosaccharides = final product of CHO digestion
l. monosaccharides - absorbed into the portal blood
2. ordinary diet
a. CHO is mostly starches
b. >80% of the final CHO digestion product is glucose
F. absorption of carbohydrates
1. aided by increased surface area
a. folds of Kerckring = plica circularis
b. villi - increase surface area 30X
c. microvilli - increase surface area 600X
143
2. glucose and galactose taken up with Na
3. uses Na/K pump to create gradient
4. glucose & galactose compete for movement
5. movement is dependent on the presence of Na
6. absorption is assisted by:
a. diffusion
b. facilitated transport
7. fructose
a. probably receptor mediated
b. not dependent on Na
c. does not compete
8. glycemic index
a. not all foods release glucose at the same rate
b. high glycemic index
1. elevated glucose
2. elevated insulin
3. increased fat absorption
9. insulin blocks hormone sensitive lipase
10. glucagon stimulates hormone sensitive lipase
11. coffee and stimulants:
a. stimulate cyclic AMP
b. degradation of FFA
c. increase FFA release
G. RDA - CHO requirements
1. adult = 0.8 gm/Kg body wt.
2. child = 2 gm - 4 gm/ Kg body wt.
3. may need to increase with exercise
144
Digestion of Carbohydrates
Starches
Ptyalin (saliva) = 20 to 40% CHO digestion (3-5% of digestion is in the mouth, remaining is in
stomach; up to pH of < 4, approx. 30-40 min)
Pancreatic amylase = 50 -80% of CHO digestion (begins in duodenum, ~10 min., most CHO
digestion is in jejunum)
Lactose
Sucrose
Maltose and 3 to 9 glucose polymers
Maltase & -dextrinase
(intestine)
isomaltase, maltoligosaccharides
Glucose
Lactase
(intestine)
Galactose
Sucrase
(intestine)
Fructose
III. Digestion of Protein
A. dietary protein
1. long chains of aminos acids (A.A.)
2. bound by peptide linkages
B. characteristics determined by:
1. types of A.A. in molecule
2. arrangement of A.A.
C. sources of protein:
1. endogenous protein:
a. salivary secretions
b. bile
c. epithelium
d. digestive secretions
e. ~ 180 gm/day
2. exogenous protein:
a. diet
b. 80 - 100 gm/day - American diet
145
3. egested protein:
a. GI cells (mostly from the colon)
b. GI flora
D. digestion of proteins in the stomach
1. pepsin:
a. important peptic enzyme of stomach
b. most active at pH of 2.0 - 3.0
c. inactive at pH > 5.0
d. activity is dependent on acid environment created by HCl
e. can digest collagen
1. an albuminoid
2. major constituent of intercellular connective tissue
f. only begins the process of protein digestion
g. provides 10 - 20% of protein digestion
Digestion of Proteins
pepsinogen
HCL
Proteoses
Peptones
Polypeptides
pepsin
1. Proteins
Proteoses
2. Peptones
Polypeptides
3.
Polypeptides
+
Amino Acids
(in the stomach)
Polypeptides
+
trypsin, chymotrypsin, carboxypolypeptidase, proelastase
Amino Acids
Amino Acids
peptidases
E. digestion of proteins by pancreatic secretions
1. endogenous protein:
a. salivary secretions
b. bile
c. epithelium
146
d. digestive secretions
e. 180 gm / day
2. exogenous protein
a. American diet
b. 80 100 gm / day
3. egested protein
a. GI cells of colon
b. GI flora
4. protein digestion occurs mainly in the duodenum and jejunum in
alkaline environment
5. digestion occurs via proteolytic enzymes of the pancreas
6. forms of protein leaving the stomach:
a. proteoses
b. peptones
c. large polypeptides
7. major proteolytic pancreatic enzymes in the small intestine:
a. trypsin splits protein molecules into small polypeptides
b. chymotrypsin
c. carboxypolypeptidasecleaves A.A. from carboxyl ends of
polypeptides
d. proelastase gives rise to elastase, which digests elastin fibers
8. after digestion by pancreatic juices:
a. some A.A. constituents
b. dipeptides
c. tripeptides
d. larger peptides
F. digestion of peptides by peptidases in the enterocytes
1. enterocytes
a. perform last digestion of proteins in intestinal lumen
b. line the villi of small intestine
c. mainly in duodenum and jejunum
147
d. possess brush border with hundreds of microvilli on surface
e. peptidases are contained in cell membrane of microvilli
2. 2 types of brush border peptidase enzymes of importance:
a. aminopoly-peptidase
1. amino - oligopeptidase
2. amino - pepidase
3. dipeptidly aminopeptidase
b. several dipeptidases
3. peptidase enzymes split large polypeptides into tripeptide and
dipeptides, and some into A.A.
4. A.A., dipeptides, and tripeptides are transported through the microvillar
membrane to the interior of the enterocyte
G. digestion of protein in cytosol of enterocyte
1. multiple peptidases
a. prolidase
b. dipeptidase
c. tripeptidase
2. peptidases specific for linkages between amino acids
3. digestion to final stage of single A.A. occurs within minutes
4. A.A. pass through opposite site of enterocyte into the blood
5. about 99% of absorbed digested protein is single A.A.
6. very rare to have peptide and protein absorption
a. more common in fetal gut
b. used in rehab of injury via receptor mediated transport
c. creates allergic and immunological disturbances
H. no one method for AA uptake
1. L more easily absorbed than D type
2. AA carriers
a. dibasic AA
b. dicarboxycylic AA
c. neutral AA
148
d. imino acid-glycine
3. sodium transport
4. diffusion - major transport mechanism
IV. Digestion of fat
A. fat
1. mostly triglycerides - glycerol nucleus and 3 fatty acids
2. triglycerides = neutral fat
a. major constituent in food
b. mainly animal origin
3. also seen in the diet:
a. triacyelglicerides = triglycerides
b. phospholipids
1. a fat
2. contains fatty acid
c. cholesterol
1. sterol compound
2. contains no fatty acid, but is considered a dietary fat
3. derived from fat
4. has physical and chemical characteristics of fats
5. metabolized similarly as fats
d. cholesterol esters
1. a fat
2. contains fatty acid
B. digestion of fats in the small intestine
1. lingual lipase:
a. secreted by lingual glands
b. travels to stomach in saliva
c. digests small amount of triglycerides in stomach (<10%)
2. most fat digestion occurs in small intestine
C. emulsification of fat by bile acids and lecithin
149
1. emulsification
a. first step in fat digestion
b. occurs by:
1. agitation
2. bile:
a. prevents hydrolysis of fats
b. secreted by the liver
c. contains no digestive enzymes
d. contains large quantities of :
1. bile salts
2. phospholipid lecithin
2. bile salts and phospholipid lecithin
a. both are soluble in fat & water
b. act as detergents
c. increase surface area of fats
3. lipases are water-soluble compounds
a. can attack the fat globules only on their surfaces
b. co-lipase knocks bile off of fat so that lipase can
hydrolyze the fat
D. digestion of triglycerides by pancreatic lipase
1. pancreatic lipase = glycerol hydrolase
a. most important enzyme for triglyceride digestion
b. found in pancreatic juice
c. produced in enormous quantities
d. digests all triglycerides within a few minutes
2. enterocytes
a. found in small intestine
b. contain small quantity of enteric lipase
E. end products of fat digestion
1. most triglycerides are split by pancreatic lipase into free fatty acids
and 2-monoglycerides
150
2. small amount remains as diglycerides
F. role of bile salts in fat digestion
1. accelerates fat digestion
2. forms micelles
3. hydrolysis of triglycerides is reversible
4. bile salts remove monoglycerides and free fatty acids to prevent the
reversing of triglyceride hydrolysis
5. during triglyceride digestion:
a. monoglycerides and FFA are formed
b. fatty portion becomes dissolved in the central fatty portion
of micelles
c. concentrations of end products of digestion are reduced
d. digestive process continues
G. bile salt micelles:
a. transport medium to carry monoglycerides and FFA
b. transport to brush border of epithelial cells for absorption
c. bile salts are released at the brush border and reenter the chyme
Fat
Globule
_
Bile &
Agitation
bile salt
fat
_
bile salt
Micelles
bile salt
B
r
u
s
h
B
o
r
d
e
r
bile salt
151
fat
H. digestion of cholesterol ester and phospholipids
1. cholesterol esters
a. most common form in diet
b. free cholesterol + fatty acid molecule
2. phospholipids - contain fatty acid chains
3. lipases that free the fatty acids
a. cholesterol ester hydrolase - hydrolyzes cholesterol ester
b. phospholipase A2 - hydrolyses phospholipid
4. micelles are used for "ferry" free cholesterol and digested
phospholipids
5. essentially no cholesterol can be absorbed without micelles
I. chylomicrons - take ingested fat to CV side
J. plasma lipoproteins:
1. chylomicrons
2. VLDL
3. LDL
4. HDL
K. lipoprotein lipase:
1. stimulated by apo C-II
2. promotes fat storage
3. can be taken to monocyte
V. Basic Principles of GI Absorption
A. total fluid absorbed each day
1. 1.5 L ingested
2. 7 L secreted in GI secretions
3. 8 - 9 L total
4. all but 1.5 L is absorbed in the small intestine
152
B. absorption:
1. surface area
a. stomach does not absorb well
1. lacks villus membrane
2. tight junctions
b. duodenum and jejunum
1. folds of Kerckring = valvulae conniventes
2. villi
3. microvilli
2. mechanisms
a. active transport
b. diffusion
c. solvent drag
3. water
a. moved by diffusion
b. moves with absorbed substances
c. maintains osmotic environment
4. ions
a. sodium
b. bicarbonate
5. nutrients
a. carbohydrates
b. proteins
c. fats
6. large intestine
a. formation of feces
b. electrolytes and water
153
154
The Liver As An Organ
Physiology III, Tri 4
Guyton & Hall, Chapt. 70
I. The Liver
A. largest visceral organ = 2.5% of body wt.
B. receives 25% of cardiac output
1. 70-80% is from portal vein
a. from gut
b. poorly oxygenated
2. hepatic artery
C. contains lobes
D. functional unit = lobule
1. cylinder structure
2. several millimeters in length
3. 0.8 to 2 millimeters in diameter
4. 50,000 to 100,000 lobules/liver
E. lobules are constructed around a central vein
1. central vein empties into hepatic vein
2. hepatic vein empties into inferior vena cava
F. hepatic cellular plates
1. radiate centrifugally from the central vein like spokes of a wheel
2. two cells thick
G. sinusoids
1. lie between hepatic cellular plates
2. allows for the "collecting of blood" from the hepatic artery and
portal vein
3. has continuous flow of portal venous blood
4. endothelial in nature - extremely large pours
5. do not have basement membrane
6. are lined with specialized cells:
a. Kupffer cells (a.k.a. reticuloendothelial cells)
155
1. from macrophages
2. part of the fixed reticuloendothelial system
3. degrades:
a. bacteria
b. RBC's
c. debris
b. Ito cells
1. located near
a. Kupffer cells
b. sinusoid cells
2. contain fat droplets
3. stores vit. A
H. bile canaliculi
1. lie between the hepatic plates
2. empty into the bile ducts
I. hepatocytes are connected by tight junctions
J. arrangement of hepatocytes along liver sinusoids allow for rapid exchange of
molecules
K. hepatic arterioles
1. in the interlobular septa
2. supply arterial blood to the septal tissues between the adjacent lobules
3. empty into sinusoids
L. space of Disse
1. lies between the endothelial cells and hepatic cells
2. connect with lymphatic vessels in the interlobular septa
3. removes excess fluid via the lymphatic vessels
II. Functions of the Liver
A. vascular function
1. storage of blood - absorbs 0.5 -1.0 liter of blood
2. filtration of blood
156
B. metabolic functions
C. secretory and excretory functions - bile formation and distribution
III. Vascular Function
A. blood flow/min:
1. 1100 ml from portal vein
2. 350 ml from hepatic artery
3. 1450 ml/min total hepatic blood flow
4. 29% of resting cardiac output
B. Fick principle - measurement of blood flow
Hepatic blood flow (ml/min) = rate of dye excretion (mg/min)
A-V difference in dye (mg/ml)
C. pressure and resistance
1. portal vein = 9 mmHg
2. hepatic vein = 0 mm Hg
3. small pressure difference = low resistance
4. flow = 1.45 liters/min
D. cirrhosis
1. fibrous tissue
a. destroys parenchymal cells
b. restriction of blood vessels
c. impedence of flow
2. causes:
a. alcoholism
b. poisons - ex. carbon tetrachloride
c. viruses - ex. hepatitis
d. infections
E. blood reservoir:
1. normally: 450 ml ~ 10% of total blood volume
2. in congestive heart failure: can increase by and extra 0.5 to 1 liter
157
F. lymph flow
1. under resting conditions, ½ of lymph formed is from the liver
2. contains high protein concentration - 6 gm/dl
G. Ascites
1. increase in hepatic venous pressure (only 3 - 7 mm Hg above normal)
2. transude leaks through liver capsule
3. fluid collects in the abdomen
4. plasma like fluid (contains 80 - 90% as much protein as plasma)
H. hepatic macrophage system
1. blood flow to liver contains intestinal bacteria
2. Kupffer cells endocytosis bacteria within 0.01 seconds of exposure
3. < 1% of bacteria from portal blood leaves the liver
IV. Metabolic Function
A. detoxification
1. metabolism of drugs and xenobiotics often involves conjugation
2. conjugation is for the production of a less toxic water-soluble form
B. ethanol detoxification to acetate
1. requires the use of 2NAD+
2. males make more dehydrogenase enzyme than females and can detox
alcohol faster
(1st enzyme) alcohol
dehydrogenase
Ethanol
NAD+
acetaldehyde
dehydrogenase
(toxic)
Acetaldehyde
NADH + H+
NAD+
cytosol of hepatocyte
CoA
Acetate
citric acid cycle
NADH + H+
in mitochondrion
3. excess ethanol metabolism will tie up the NAD+ required for the
conversion of malate to oxaloacetate step of gluconeogenesis (inhibit
gluconeogenesis).
Malate
Oxaloacetate
NAD+
NADH + H+
158
4. excess ethanol metabolism after exercise will cause dehydration
5. enhancement of process of pyruvate reduction to lactic acid
Pyruvate
Lactate
NADH + H+
NAD+
(regenerated)
C. R-H degradation by the cytochrome P450 system
1. Phase I
a. for increasing water solubility, the body oxidizes the R-H to the
alcohol R-OH
b. enzymes are not well developed in newborn or the aged
c. excess production of enzymes (ex. smokers) will cause faster
degradation of drugs = less effect of medication
d. protein dependent - protein monooxygenases
e. monooxygenases:
1. uses 1 oxygen
2. not specific in nature
3. located in microsomal and intramitochondrial
membranes
NADPH + H+
Reducing equivalent
NADP+
OX
cyt P450
reductase
Fe-S
reduction
OX
RH
O2
cyt P450
reduction
H2O
RHO
2. phase II
a. the liver can still make R-OH more soluble by conjugation of
the newly made alcohol
b. (R-OH) most often conjugated with glucuronic acid
c. others:
1. glycine
2. taurine
3. sulfates
159
D. carbohydrate metabolism
1. functions:
a. storage of glycogen
1. maintains blood glucose levels
2. glucose buffer function
b. conversion of galactose and fructose to glucose
c. gluconeogenesis
1. occurs when blood glucose falls below normal
2. AA and glycerol are converted into glucose
d. formation of chemical compounds of carbohydrate metabolism
2. glucose
a. blood glucose following a meal
b. glucose is taken to liver via portal system
c. facilitated transport moves glucose into liver; co-transported
with sodium in the small intestine
d. glucose is phosphorylated by hexokinase to produce Glucose-6phosphate (G-6-P)
e. G-6-P used in the formation of glycogen
3. fructose
a. moved via facilitated transport - uptake from small intestine
b. phosphorylated to produce fructose 1-phosphate
c. fructose 1-phosphate is converted to G-6-P or used in the
glycolytic pathway
4. galactose
a. moved via facilitated transport - from gut Na co-transport
b. phosphorylated to produce galactose 1-phosphate
c. uridine diphosphate is then added to get UDP-galactose
d. UDP-galactose is used in glycolipid/glycoprotein structure in
the lipid membrane - glycocalyx
e. OR - converted to UDP-glucose and recycled
E. gluconeogenesis
160
1. formation of glucose
a. during starvation
b. during decreased CHO intake
2. oxaloacetate is used for the formation of glucose (reverse glycolysis not an exact reversal)
3. glucose is the preferred fuel of the brain
4. AA are used for fuel
a. alanine is most commonly used
b. found in abundance in muscle tissue
c. Alanine cycle
F. formation of glycogen
1. storage form of glucose
2. 7 - 10% of liver weight is glycogen
3. from lactate
a. 1/3 of lactate is used to produce glucose
b. 2/3 of lactate is used to produce pyruvate
G. glycogen degradation
1. -1-4 and -1-6 ; highly branched
2. 1st enzyme:
a. glycogen phosphorylase breaks down glycogen to
glucose-1-phosphate
b. glycogen is the major storage form of fuel - ATP and creatinephosphate stores are small
c. McArdle's disease - missing glycogen phosphorylase
3. 2nd enzyme:
a. release of glucose for the cell
b. G-6-Phosphatase
1. dephosphorylation is required
2. phosphorylated glucose can not leave the cell
c. skeletal muscle does not have G-6-Phosphatase
d. skeletal muscle does not release glucose into the blood
161
e. hormones which affect these processes:
1. insulin - liver is very sensitive to insulin
2. glucagon
3. epinephrine
H. fat metabolism
1. high rate of oxidation of fatty acids to supply energy for other
bodily functions
a. to derive energy from neutral fats:
1. fat is first split by beta-oxidation into two-carbon acetyl
radicals to form acetyl-CoA
2. acetyl-CoA can enter the citric acid cycle
3. excess acetyl-CoA is converted to acetoacetic acid
4. acetoacetic acid is transported throughout the body and
absorbed by other tissues
5. acetoacetic acid can be reconverted to acetyl-CoA and
oxidized
6. palmitic acid - base fatty acid synthesis in cytosol
7. liver lacks ketone acid transferase and can not use
ketone bodies for fuel
8. RBC and adrenal medulla can only use glucose
Fatty Acids
Acetyl-CoA
TCA cycle (in the presence of CHO)
Ketone bodies (in the absence of CHO)
9. brain prefers glucose but can use ketone bodies
10. ketone bodies
keto acidosis
a. fluid loss to get rid of ketones
b. mineral loss (especially Na+)
c. dehydration
d. emesis = vomiting
162
HDL
Gut
Chylomicrons
Remnant
Liver
Cholesterol
VLDL
IDL
LDL
Tissue
triacylglycerols
2. formation of most of the lipoproteins
a. lipoproteins produced in the liver:
1. VLDL - transport of fat products from liver
2. LDL
3. HDL
a. moves cholesterol (small amount) to liver
b. also produced by plasma
b. chylomicrons and VLDL (very little ir any) are lipoproteins
produced in the gut
c. chylomicrons are larger than VLDL
d. chylomicrons transport products of fat digestion from the gut to
various tissues
e. lipoprotein lipase:
1. required for lipid removal from chylomicron
2. elevated levels in the obese
f. the liver has LDL, HDL, and IDL receptors
g. liver is the main organ for getting rid of cholesterol
h. triacylglycerol is largest component in chylomicrons
i. VLDL gives rise to LDL as it gives up triacylglycerol
3. synthesis of large quantities of cholesterol and phospholipids
a. 80% of cholesterol synthesized in the liver (from Acetyl-CoA)
is converted into bile salts
b. phospholipids are synthesized in the liver and transported in the
lipoproteins
c. cholesterol and phospholipids are used by the cell for:
1. membrane formation
163
2. intracellular structures
3. chemical substances for cellular function
4. hormone production (steroids)
4. conversion of large quantities of carbohydrates and proteins into fat
a. almost all fat synthesis form CHO and proteins occurs
in the liver
b. transported in lipoproteins to the adipose tissue
I. protein metabolism - necessary for life
1. deamination of AA
a. primarily occurs in the liver
b. required for:
1. AA to be used as energy
2. AA conversion into CHO or fats
2. formation of urea for removal of ammonia from the body fluids
a. removes ammonia from plasma
b. without this function, hepatic coma and death can occur
c. is a result of ammonia released by deamination from
AA degradation
3. formation of plasma proteins
a. all are formed in the liver except gamma globulins
b. rate of formation 15 - 50 gm/day
c. plasma proteins produced by the liver
1. fibrinogen
2. prothrombin
3. transferrin
4. transferrin
5. haptoglobin
6. hemopexin
7. albumin:
a. main protein produced by the liver
b. about 3 g/day is produced
c. required for maintaining osmotic pressure
164
d. acts as a buffer
4. interconversions among AA and other substances
a. liver can synthesize all non-essential AA
b. AA are required for the synthesis of non-essential AA (11) form
essential ones (9)
c. essential AA:
1. histidine
2. threonine
3. phenylalanine
4. isoleucine
5. leucine
6. valine
7. lysine
8. methionine
9. arginine (sometimes)
Examples:
Phenylalanine
Methionine
Tyrosine (difference is OH group)
Cysteine (used for producing disulfide
bonds)
V. Excretion of Bilirubin in the Bile
A. bilirubin
1. greenish yellow pigment
2. major end product of hemoglobin degradation
3. bilirubin excretion is diagnostic tool for hemolytic blood diseases and
some liver diseases
B. RBC
1. 120 day lifespan
2. tissue macrophages = reticuloendothelial system
a. split hemoglobin into globin and heme
b. heme ring is opened to give:
1. free iron that is transported in the blood by transferrin
165
2. straight chain of four pyrrole nuclei that eventually
forms bilirubin
c. free (unconjugated) bilirubin is transported by albumin
d. bilirubin is transported to the liver and conjugated with:
1. glucuronic acid to form bilirubin glucuronide (80%)
2. sulfate to form bilirubin sulfate (10%)
e. bilirubin is excreted from the hepatocytes by an active transport
process into the bile canaliculi and into the intestines
f. bacteria in the gut convert bilirubin to urobilinogen
g. most urobilinogen is reabsorbed and re-excreted by the liver
h. 5% of urobilinogen is excreted by the kidneys in urine and
oxidized with exposure to air to form urobilin
i. in the feces urobilinogen is altered and oxidized to form
stercobilin
SEE Figure 70-2, Page 887 in Guyton and Hall
C. jaundice
1. yellowish tint to body tissues
2. due to large quantities of bilirubin in the extracellular fluids
3. causes of jaundice:
a. destruction of RBCs with rapid release of bilirubin
into the blood
b. obstruction of the bile ducts
c. damage tot he liver cells so that even the usual amounts
of bilirubin cannot be excreted in the GI tract
D. types of jaundice:
1. hemolytic jaundice:
a. excretory function of the liver is not impaired
b. RBC hemolyzed rapidly
c. hepatic cells cannot excrete bilirubin as fast as it is formed
d. rate of formation of urobilinogen
e. rate of urobilinogen absorption
166
f. most plasma bilirubin is in the "free" form
(van den Bergh reaction)
2. obstructive jaundice:
a. obstruction of bile ducts
1. gall stones
2. cancer
b. damage to the hepatic cells (hepatitis)
c. bilirubin cannot pass from the blood into the intestines
d. blood levels of conjugated bilirubin increase
e. urobilinogen in the urine is negative
f. stools are clay-colored - lack of stercobilin and bile pigments
g. significant quantities of conjugated bilirubin appear in the urine
(shaking the urine produces intense yellow foam)
VI. Storage Capabilities of the Liver
A. fat-soluble vitamins
1. vit A:
a. precursor of -carotene
b. -carotene is 2 vit A's combined
c. forms:
1. retinal (aldehyde)
2. retinoic acid
3. retinol
d. retinol is the form that is transported by chylomicrons
e. -carotene overdose causes skin color to be yellow/orange
f. -carotene overdose in pregnancy can harm unborn child
2. vit. D:
a. transported by chylomicron in non-esterified form to liver
b. is activated 1st by hydroxylation in the liver to form 25cholecalciferol (not the most active form)
167
c. 2nd hydroxylation occurs in the kidneys (1, 25dihydroxycholecalciferol = most active form)
3. vit. K
a. prothrombin production requires vit. K and CO2
b. active form produced in the liver
c. stored in liver and muscle
4. vit B12
a. 5 - 12 mg of vit B12 stored in the liver (50 - 90%)
b. enough to last 3-5 years
B. the liver is important in the storage and homeostasis of iron
1. presented in both heme and non-heme forms
a. heme - meats
b. non-heme forms - phytate in vegetables
2. transferrin - protein carrier of iron
3. ferritin
a. short-term storage of iron
b. easily released
c. stored in epithelial tissue
4. hemosiderin
a. long term storage of iron
b. not easily released
VII. Endocrine functions of the Liver
A. modification and amplification of hormone activity
1. vit. D
a. cholecalciferol (1st hydroxylation, 2nd occurs in kidney)
b. acts as a hormone
2. growth hormone = somatotropin
a. modified by insulin-like growth factors
b. somatomedins
3. thyroxine - modified by the liver
168
B. hormone degradation
1. insulin - liver is very sensitive to insulin
2. glucagon
3. growth hormone - half life of 20 minutes
4. gastrin
169
170
Dietary Balances and Metabolic Rate
Physiology III, Tri 4
Guyton & Hall, Chapt. 71 & 72
I. Some Facts:
A. one hour of nutritional counseling = $75
B. single coronary artery bypass surgery = $43,000+
C. 50% of all bypass surgeries need repeating within approximately 5 years
D. 50% of all diseases caused by diet
E. each school lunch contains 38-40% fat
F. American Heart Association states that diet should contain < 30% fat
G. < 10% fat in diet is recommended by Dean Ornish, MD
H. in 1532 autopsies of teenagers, 100% had coronary heart disease (CHD)
I. autopsies of American Soldiers killed in the Korean conflict, (18 - 21 yr.)
100% had CHD
J. 23% of American children are obese ( may be as high as 40%)
K. modernization of society:
1. caloric intake
2. caloric utilization
a. computers
b. TV
L. of men ages 18 - 79, 15,000,000 are overweight
M. of women ages 18 - 79, 16,000,000 are overweight
N. 2,290,000 lbs. of excess human fat in USA
1. = 1.3 billion gallons of fuel
2. = enough energy to supply electricity for Boston, Chicago, and San
Francisco for 1 year
3. enough fuel to supply 900,000 autos for one year
O. lbs of food consumed per person
1. the year 1978 = 1500 lbs. / person
2. the year 1980 = 1620 lbs. / person
171
P. American ice cream consumption = 46.3 pints / yr. / person
II. Alteration of Body Weight
A. 1 lb of body fat = 3,500 kilocalories (kcal)
B. 1 lb of body fat = 454 grams of fat + water
C. 87% of "body fat" is fat
454 gm X .87 = 395 gm
395 gm X 9 kcal /gm = 3500 kcal
D. reasonable goal for weight loss = .5 to 1.0 lbs / wk
E. body weight should be decreased gradually
F. Diet = lifestyle change
G. caloric input for diet:
1. 10 kcal / lb of body wt.
2. 180 lb person X 10 kcal = 1800 kcal/day
H. do not decrease caloric intake below 1200 kcal
I. supplements should be considered with reduced caloric intake
III. Weight Loss
A. body weight loss is not exclusively fat weight loss
B. with body weight loss, muscle mass is also lost
C. with a starvation diet, equal amounts of fat and muscle tissue are lost
D. weight training and aerobic exercise are advised with weight loss programs
IV. Energy In - Energy Out
A. amount of food eaten
B. composition of food
C. bomb calorimeter
1. used to measure calories contained in food
172
2. food is burned
3. heat is produced
4. heat is measured
5. heat generated is used to measure calories of food
D. calories
1. CHO = 4 kcal/gm
2. fat = 9 kcal/gm
3. protein = 4 kcal/gm
4. alcohol = 7 kcal/gm
E. stimulus for eating
1. feeling of hungry (Is there anything to eat?)
2. appetite (What do I want to eat?)
3. satiety center
V. Control of Eating
A. hypothalamus
1. lateral nuclei
a. hunger or feeding center
b. stimulation hyperphagia
c. destruction of center starvation
2. ventral medial nuclei
a. satiety center
b. stimulation aphagia
c. destruction of center hyperphagia
VI. Substances that effect eating
A. glucose = main influence
B. protein
C. fat
D. body temperature
1. body temperature. feeding heat production
173
2. body temperature feeding heat production
3. for increasing caloric expenditure:
a. run in cold environment
b. run uphill
c. run against wind
E. alimentary
1. distention - feedback to hypothalamus
2. hormones
a. CCK hypothalamus
b. lepton
1. fat rats = lepton
2. fat people = lepton
F. oral receptors
1. in animals
2. may be present in dogs - esophageal fistula
a. satiety following a meal
b. 20 - 40 min post eating - will be hungry
VII. Calorimetry - Measurement of Metabolic Rate
A. direct calorimetry - same as bomb calorimetry
B. indirect calorimetry
1. closed circuit
2. measures O2 uptake
3. does not allow for quick exchange of gases
4. not used for exercise
5. used for measurement of BMR
C. open circuit spirometry
1. ambient air
2. portable
a. units that are attached to person
b. measures calories while at work, play, various tasks
174
3. measures volume of gas exchanged
4. maintains aliquots of gas for measurement
D. Douglas Bag
1. antiquated system
2. used earlier in century
3. used for establishing accuracy between direct and indirect methods
VIII. Respiratory Quotient = RQ
A. measures:
1. O2 used / CO2 produced
2. what fuel is being burned
B. C 6 H 12O6 + 6O2 6CO2 + 6 H2O
carbohydrate
6CO2
6O2
= 1.00
RQ for CHO = 1.0
C. fat
C12 H32 O2 + 23 O2 16 CO2 + 16 H2O
palmitic acid
16 CO2
23 O2
= 0.696 (.70)
O2 C with fat as compared with CHO
D. protein = 0.818 (0.80)
E. mixed diet = mixed RQ
F. average RQ for mixed diet = 0.82
IX. Generation of Heat
A. basal thermogenesis:
1. basal metabolic rate
a. BMR
b. rate at rest
175
c. 2/3 (60-70%) of energy requirements
d. decreases ~10% during sleep
2. resting metabolic rate
a. RMR
b. sitting position
3. factors influencing BMR:
a. age
BMR peaks at ~ 4 yrs of age
BMR
_____________________
2
4 6 8 10
b. size
height = surface area = BMR
c. pregnancy
1. 2 & 3 trimester
2. increased tissue
3. increased mitotic rate
d. lactation
e. stress
1. trauma
2. psychological
3. illness
4. fever - for every degree of fever, BMR increases 7%
f. thyroid hormones
1. hyperthyroid
2. hypothyroid
3. 5' monodiodoionase - converts T4 to T3
g. other hormones
1. GH
lean
fat
2. testosterone
47%
20%
3. insulin
Age 25
4. etc.
other
h. environmental temperature
6% 27%
i. lean tissue mass
1. lean wt. = BMR
2. 20 - 25% of energy
bone & mineral
j. brain & liver
fat 36%
a. 4% of body wt.
Age 70
b. 40% of total energy output
lean
k. fasting, starvation, malnutrition = BMR
36%
24%
other
bone & mineral
4%
176
4. Calculation of BMR
a. BMR = 1.3 kcal / hr. /kg
1. fat free body wt.
2. for ages 20 - 60 yrs. of age
b. Men = BMR = 1.0 kcal / hr /kg
c. Women = BMR = 0.9 kcal / hr./ kg.
B. exercise induced thermogenesis
1. total body wt.
2. amount of lean mass
3. type of activity
4. intensity of activity
C. diet induced thermogenesis
1. thermic effect of food
a. energy required to utilize food ~ 10%
b. varies greatly
c. protein requires the most energy for utilization
D. adaptive (facultative) thermogenesis
1. 10% of energy requirement
2. brown fat - heat production
3. shivering - involuntary activity
E. total energy requirement
BMR + type of activity + thermic effect of food = energy requirement
XII. Body Composition
A. big bodies do not automatically mean person is overweight or fat
(ex. athletes with high lean weight and low body fat)
B. societal factors
1. sumo wrestlers
2. female fashion models
C. obesity - coupled with another factor(s) will exponentially increased
177
risk of disease
D. morbidity with obesity
E. diabetes mellitus
1. adult onset
2. high correlation with increased weight
F. blood pressure, heart disease, and stroke incidences all increase with obesity
G. cancer
1. uterine cancer
2. fat tissue produces estrogen
3. estrogen = cancer risk (endometrial)
4. estrogen = infertility
H. hiatal hernia - increases with obesity
I. orthopedic problems
1. arthritis
2. lumbar lordosis
3. impaired mobility
J. skin
1. apron ( excess skin)
2. moisture, friction, infection
3. infertility, sexual performance
K. breathing
1. apnea
2. shortness of breath
L. varicose veins - blood clots
M. risk during surgery
N. pregnancy
1. gestational diabetes
2. blood pressure
3. size of child
a. glucose
b. calcium
178
O. social prejudice
P. discrimination
Q. psychological suffering
179
180
181