Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neurogenomics wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Biochemistry of Alzheimer's disease wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Central pattern generator wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Perivascular space wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Synaptic gating wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
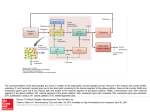
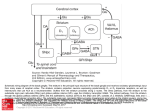
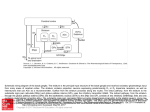
Cell Bio 8- Basal Ganglia Basal Ganglia: collection of gray matter nuclei located deep within the white matter of the cerebral hemispheres Striatum receives all inputs to the basal ganglia Cell Bio 8- Basal Ganglia Inputs to the Basal Ganglia The main input comes from massive projections from the entire cerebral cortex to striatum Putamen is the most important input nucleus of the striatum for motor control pathways: most cortical inputs are excitatory and use glutamate Another important input is the substantia nigra pars compacta: this dopaminergic nigrostriatal pathway is excitatory to some cells and inhibitory to others Outputs from the Basal Ganglia For motor control, the substantia nigra pars reticulata convey information for the head and neck, while the internal segment of the globus pallidus conveys information for the rest of the body These output pathways are inhibitory and use GABA. The main output pathways are to the VL and VA nuclei of the thalamus via the thalamic fasciculus Anteriolateral pathway VPL of thalamus Sensory from face VPM Internal Connections Direct pathway: travels from the striatum directly to the internal segment of the globus pallidus or the substantia nigra pars reticulata Indirect Pathway: takes a detour from the striatum, first to the external segment of the globus pallidus and then to subthalamic nucleus, before reaching the internal segment of the globus pallidus or the substantia nigra pars reticulata The net effect of excitatory input from the cortex through the direct pathway will be excitation of the thalamus The net effect of excitation of the indirect pathway will be inhibition of the thalamus, resulting in inhibition of movements through connections back to the cortex GPi: globus pallidus pars interna GPe: globus pallidus pars externa SNr: substantia nigra pars reticulata STN: subthalamic nucleus Cell Bio 8- Basal Ganglia Patients with basal ganglia lesions can have either hypokinetic or hyperkinetic movement disorders Parkinson’s disease (hypokinetic): rigidity, slowness, and marked difficulty initiating movements Huntington’s disease (hyperkinetic): uncontrolled involuntary movements produce a random pattern of jerks and twists Parkinson’s Disease Is a common idiopathic disease caused by loss of dopaminergic neurons in the substantia nigra pars compacta. It is characterized by asymmetrical ‘pill-rolling’ resting tremor, bradykinesia, rigidity, and postural instability, which usually respond to therapy with levodopa. The decreased blink rate and rigid and shuffling gate are typical of Parkinson’s disease. These problems result from a decreased input from the ventrolateral (VL) nucleus of the thalamus to the motor cortex of the brain. This input, which is modulated by the basal ganglia, normally modifies descending cortical motor output to allow the individual to initiate voluntary movements at an appropriate pace. o Thalamic input is modulated by the basal ganglia via two basal ganglia pathways. The extent to which the VL nucleus is inhibited depends on the balance of activity in each pathway. A- Section through the midbrain from a patient who died with Parkinson’s disease. Asymmetrical pallor affecting the right substantia nigra greater than the left can be seen, caused by degeneration of pigmented dopaminergic neurons B- Typical Lewy body. It has a characteristic dense (pink) center with a lighter halo and is located in the cytoplasm of a darkly pigmented dopaminergic neuron (Dementia with Lewy bodies for differential diagnosis) Cell Bio 8- Basal Ganglia Huntington’s Disease Is an autosomal dominant neurodegenerative condition characterized by a progressive, usually choreiform movement disorder, dementia, and psychiatric disturbances, ultimately leading to death. The pathologic hallmark is progressive atrophy of the striatum, especially involving the caudate nucleus. Usual age of onset is between 30 and 50 years, with prevalence of 4-5 cases per million. Subtle eye movement abnormalities can be detected before other manifestations become apparent. These are slow saccades, impaired smooth pursuit, difficulty initiating saccades without moving the head or blinking. The abnormal gene is mapped on chromosome 4, and it includes a region containing multiple repeats of the trinucleotide sequence CAG in tandem. Behavior changes may occur before movement problems, and can include: • Behavioral disturbances • Hallucinations • Irritability • Moodiness • Restlessness or fidgeting • Paranoia • Psychosis Abnormal and unusual movements include: • Facial movements, including grimaces • Head turning to shift eye position • Quick, sudden, sometimes wild jerking movements of the arms, legs, face, and other body parts • Slow, uncontrolled movements • Unsteady gait Dementia that slowly gets worse, including: • Disorientation or confusion • Loss of judgment • Loss of memory • Personality changes • Speech changes Cell Bio 8- Basal Ganglia Cell Bio 8- Basal Ganglia Bradykinetic (slowed movements) disorders can be caused by increased inhibitory basal ganglia outflow to the thalamus Rigidity Increased resistance to passive movement of a limb In spasticity, which results from upper motor neuron lesions, rigidity is velocity dependent. Resistive tone initially increases as the muscles of the limb are stretched, but it may then decrease, giving rise to claspknife rigidity in corticospinal disorders In contrast, rigidity caused by basal ganglia disorders tends to be more continuous throughout attempts to bend the limb, and it has therefore been called plastic, or lead pipe rigidity Dystonia The patient assumes abnormal, often distorted positions of the limbs, trunk, or face that are more sustained or slower than in athetosis Focal dystonias include torticollis, which involves the neck muscles; blepharospasm, which involves the facial muscles around the eyes, and spasmodic dysphonia, which involves laryngeal muscles o Many cases of dystonia respond well to injection of botulinum toxin into the affected muscles Athetosis is characterized by twisting movements of the limbs, face and trunk that sometimes merge with faster choreic movements, giving rise to the term choreoathetosis Cell Bio 8- Basal Ganglia Ballismus: Movements of the proximal limb muscles with a larger-amplitude, more rotatory or flinging quality than chorea Hemiballismus (the most common type): there are unilateral flinging movements of the extremities contralateral to a lesion in the basal ganglia Chorea Is applied to movement disorders characterized nearly continuous involuntary movements that have a fluid or jerky, constantly varying quality (dancing-like) In mild case, low-amplitude chorea may be mistaken for fidgeting or restless movements of extremities, face or trunk Often incorporated into voluntary movements in an attempt to conceal their occurrence Major cause of chorea is Huntington’s disease ( autosomal dominant neurodegenerative disorder).