Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Microneurography wikipedia , lookup
Nervous system network models wikipedia , lookup
Human brain wikipedia , lookup
Neuroplasticity wikipedia , lookup
Neuroeconomics wikipedia , lookup
Time perception wikipedia , lookup
Aging brain wikipedia , lookup
Environmental enrichment wikipedia , lookup
Molecular neuroscience wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Synaptogenesis wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Neuroanatomy wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
Optogenetics wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Central pattern generator wikipedia , lookup
Development of the nervous system wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Embodied language processing wikipedia , lookup
Muscle memory wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Synaptic gating wikipedia , lookup
Channelrhodopsin wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Cerebral cortex wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Eyeblink conditioning wikipedia , lookup
Motor System
본3 신경과학
신형철 교수
Movements
1. Reflex-controlled Movements
Knee Jerk, withdrawal from HOT stuff, reflex
Stimulus---> automatic, repetitive, stereotyped responses
Spinal Cord is important
Ex: decerebrate frog:
a) pinch to hind foot---> pulled away
b) noxious stimulation to frog's back---> response with hind foot
Corneal reflex , coughing , swallowing, food propel, breathing , blood flow etc.
Stimulus-Response theory of behavior: Combinations of reflex---> complex behaviours
2. Program-controlled (automatic) movements
walking (newborn baby: 12-18 month, independent), running , crawling breathing, chewing
species specific fixed action pattern (nesting, tunneling, urination, etc)
learned programs: sport, work, typing, drawing, driving
enough practice--->automatic.
central programs can be influenced by sensory feedback.
Program theory of behavior without any external sensory inflow
(stimulus independent, innate, inherited, spontaneous, voluntary (initiation & termination), rhythmic
motor pattern)
3. Voluntary & involuntary movements
Voluntary: Purposeful, goal directed, learned
Learning sports skills, speech, writing,
After learning---> automatic (program-controlled movements)
Involuntary: highly stereotyped reflex, learning unnecessary
4. Postural & goal-directed functions
Intrapersonal: posture (standing, sitting, lying, balance) orientation in
space
Extrapersonal: goal-directed
•intimate interlinkage between postural & goal-directed movements
Control: feed back: slow movement, object touch, feed forward: rapid
movement, catching ball
Three levels in hierarchy of motor control
1) motor areas of cerebral cortex - top of hierarchy
*3 major areas, all in frontal lobe
a) primary motor cortex - executes commands to
motoneurons
b) premotor cortex
c) supplementary motor cortex
*all three project directly to spinal cord via corticospinal tract
*premotor and supplementary motor cortex (b & c) also project
to primary motor cortex and are important in coordinating
and planning complex sequences of movement (motor
learning)
2) brain stem
*important nuclei include reticular formation, vestibular nuclei
and inferior olivary complex
*axons project and regulate the segmental networks of spinal
cord
*brains stem integrates visual and vestibular information with
somatosensory input to modify movements initiated by
cortex
3) spinal cord - neurons mediate automatic reflexes (e.g., stretch
reflex)
Two important subcortical systems which act on cortex
via the thalamus
1) cerebellum - receives input from spinal cord
-projects to both brainstem and thalamus (and onto
cortex)
-improves accuracy of movement (by comparing
descending motor commands with information
about resulting motor action; thus important in
learning)
2) basal ganglia
-receives inputs from all cortical areas (not just
motor)
-projects to thalamus and then to areas of cortex
involved in motor planning
-diseases of BG produce range of motor
abnormalities including hypokinesia and
hyperkinesia, Parkinson’s disease
Concept of upper and lower motor neurons (Sherrington)
lower motor neurons
- motoneurons of brainstem and spinal cord which directly innervate skeletal muscle
("final common pathway")
- symptoms of lesions:
1) muscle tone reduced or absent (flaccid paralysis)
2) stretch reflex weak or absent
3) muscle atrophy
4) fibrillation (observed by EMG)
- common causes: poliomyelitis (척수성 소아마비), nerve lesion
- can be mimicked by systemic diseases of nerve end-plate (e.g.,
myasthenia gravis) or muscle (e.g., dystrophy, myopathy
upper motor neurons
- all descending pathways of the brain and spinal cord involved in volitional control
of the musculature
- include vestibulospinal (postural) , reticulospinal and corticospinal
- unsatisfactory term for research as too inclusive but useful clinically to
distinguish from lower motor neuron
- symptoms of lesions
1) voluntary movements of affected muscle absent or weak
2) tone of muscle is increased (spasticity)
3) atrophy minimal initially
4) alteration of reflexes
common causes include infarctions of the following regions: posterior limb of
internal capsule, primary motor and premotor cortex
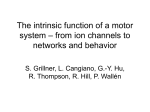
Schematic representation of the upper
motor neuron system and the muscle
motor-sensory unit.
1: motor cortex; 2: basal ganglia; 3:
cerebellum; 4: red nucleus; 5: reticular
formation; 6: lateral vestibular nucleus;
7: axons from extrapyramidal neurons;
8: intertesial neurons; 9: alpha motor
neuron; 10: gamma motor neuron; 11:
dorsal ganglion cell; (A) brain; (B)
cerebellum; (C) brainstem; and (D)
spinal cord.
Treatment
1.
2.
3.
4.
Physical Therapy & Exercise
Medications
Spine Surgery
Is a cure possible?
Consequences of spinal cord injury
Cells from the immune system infiltrate the area of primary injury, which expands for
several days as local pathological processes continue in a cascade of secondary injury.
The primary and secondary injuries cause the death of neurons and oligodendrocytes,
disruption of synaptic connections and the
demyelination of axons.
resulting in the
Demyelination of surviving intact axons greatly impairs action potential message
conduction, and can render remaining connections useless.
By several weeks after the initial injury, the area of tissue damage has been cleared away by
microglia from the CNS and macrophages from the immune system, and a
fluid-filled
cavity surrounded by a glial scar made up of astrocytes is left behind.
Molecules that inhibit regrowth of severed axons are expressed at this site. This fluid-filled
syrinx, now forms a barrier to the reconnection of
the two sides of the damaged spinal cord.
cavity, called a
a surprising amount of the basic circuitry to control movement and process somatosensory
information can remain intact.
because the spinal cord is arranged in layers of circuitry. Many of the connections and
neuronal cell bodies forming this circuitry above and below the site of injury survive the
trauma.
The goal of spinal cord injury research is to reconnect the wiring that controls muscle
movement and provides sensory information to the brain.
can neurons in the spinal cord regenerate and make not only new connections, but the
correct connections ?
Why doesn't the nervous system
regenerate very well?
Many cells of the CNS, especially
neurons, are so specialized that they
have lost this ability to divide and
generate new cells. As a result, injury to
the brain or spinal cord isn’t easily
repaired by replacing the cells that have
been injured or have died with new ones.
Key Intervention Strategies for the treatment of spinal cord injury
Acute intervention strategies to limit degeneration that occurs immediately after an injury.
More long-term intervention strategies involve regenerative and reconstructive approaches to promote
rebuilding and reconnection of the injured cord.
1) Limit initial degeneration: primary necrosis, excitotoxicity, and apoptosis.
2) Treat inflammation: Swelling and inflammation may foster secondary damage to the cord after the
initial injury. Enhancement of axonal regrowth, the correct targeting of axons (path finding), the
formation of functional neuronal connections (synapses), and remyelination.
3) Stimulate axonal growth: Neurotrophins such as NT-3 and BDNF can both promote cell survival by
blocking apoptosis and stimulate axonal growth. Each neurotrophin has very specific target cell
functions.
(4) Substrate or guidance molecules to promote new growth
(5) Block endogenous inhibition of regeneration:
(6) Supply new cells to replace lost ones: Stem cells, which are isolated from the CNS and can divide
to form new cells, may make it feasible to replace lost neurons and glia.
(7) Build bridges to span the lesion cavity
The motor unit = a motor neuron + the muscle fibers it innervates.
A muscle cell is innervated by only one neuron.
An alpha motor neuron may innervate many muscle fibers (3-2000).
The fewer fibers involved, the finer the muscle control will be. Cell bodies for the alpha motor
neurons are located in the spinal cord.
Acetylcholine is the neurotransmitter between the motor neuron and the muscle cell, and the
muscle cell has nicotinic receptors.
Polysynaptic Reflexes
Most of the reflexes are polysynaptic
Sensor is remote from effector
autonomic reflexes, polysynaptic somatic reflexes.
Characteristics of polysynaptic reflexes, ex: coughing
a) presence of delay period
b) Summation of the subthreshold stimulus in central
neurons & motorneurons of the reflex arc.
c) Reflex time & intensity of response depend on the
stimulus intensity.
d) plasticity of the reflex response, habituation,
dishabituation, sensitization, conditioning (long-term
changes in the reflex response)
Recurrent inhibition & presynaptic inhibition in spinal motor
systems
Motor neuron--->excite muscle--->excite Renshaw cells
(inhibitory interneuron)---> feedback inhibition on the same
Motor neuron.
Function: to prevent an uncontrolled oscillation of motor
neuron activity
(increased muscle tone (spasticity) may be caused by
Renshaw cell malfucnction)
The Propriospinal System & the Capabilities of the Isolated Spinal Cord
1) Intersegmental reflex connections by Propriospinal neurons & propriospinal tracts
(fore- & hindlimbs, neck & limb movements)
2) Spinal Locomotion
Basic pattern of locomotion, programmed at the level of the spinal cord.
3) Spinal Shock Reversible motor & autonomic areflexia following spinal cord section
(local cooling, local anesthesia)
many months in humans, few minutes in frogs, hours in carnivores, days or weeks in
monkeys
Mechanisms responsible for the return of certain spinal function : not konwn
Types of Myasthenia Gravis
Drug Related
Viral/Bacterial
Transient Neonatal
Adult-Onset
Experimental Autoimmune
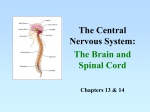
Schematic diagram of an intracellular muscle fiber recording
showing the generation of end-plate potentials (EPPs) and muscle
fiber action potential (APs).
On the left, normal neuromuscular junction function ensures that the
rise time and amplitude of successive EPPs are sufficient to
generate APs. Note the fluctuating threshold for generating an AP
and resultant variability of the AP latency. This is normal jitter.
On the right, in myasthenia gravis, there are insufficient
acetylcholine receptors and the EPP rise times and amplitudes vary
markedly. This results in increased jitter and at times failure to
initiate an AP This is called blocking.
Cortex Stimulation
Wilder Penfield, a Canadian surgeon, exploratory voyage of
the brain's organization starting in the 1950s.
epileptic patients (awake), electric currents to the brain's
surface in order to find problem areas.
trigger whole memory sequences.
familiar song that sounded so clear
any movement of the patients' bodies. From this information,
he was able to map out the motor cortex
http://www.pbs.org/wgbh/aso/tryit/brain/#
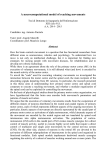
fMRI of the motor cortex, overlaid upon a
standard high resolution data set. Finger
oposition task at 2Hz. p < 0.05
[Efferent connection]
1)Corticospinal tract (Pyramidal
Tract), at spinal cord, cortical
control of segmental reflex circuit
2)The axons from the giant Betz
cells send short collaterals back to
the cortex itself
; inhibit adjacent regions of the
cortex when the Betz cells discharge
--> sharpening the boundaries of
the excitatory signal
3)To Caudate nucleus and putamen
4)To Red nucleus
5)To Reticular formation and
Vestibular nuclei
6)To Pontine nuclei
7)To Inferior olivary nucleus
[MI Afferent connection]
1) Subcortical fibers from adjacent regions of
cortex (somatic sensory areas of the parietal
cortex, frontal areas, visual cortex, auditory
cortex)
2) Subcortical fibers that pass through the
corpus callosum from the opposite cerebral
hemisphere.
3) Somatic sensory fibers derived directly
from the ventrobasal complex of the
thalamus
;transmit mainly cutaneous tactile signals
and joint and muscle signals.
4) Tracts from the ventrolateral and
ventroanterior nuclei of thalamus
;coordination between the functions of the
motor cortex, basal ganglia, and the
cerebellum
5) Fibers from the intralaminar nuclei of the
thalamus
;control the general level of excitability of
the motor cortex
Rubrospinal tract
Recent evolutionary adding than medial system
Origin: Red Nucleus (magnocellular portion) in the midbrain.
Termination: propriospinal neurons, lateral motor neurons, lateral interneurons
Function: fine movements, distal muscles (flexors) reaching, manipulating objects with fingers & hand
* in human, the remnant of rubrospinal tract, function carried by corticospinal system
The Supplementary Motor Area (SMA) The
neural activity increase in the SMA especially
in relation to complex movements.
Increased activity in the SMA is not related to
the movement itself, since it is sufficient that
the person imagines the goal directed
performance of a fairly complex movement. In
such case there is no increase of activity in
M1.
Recording of single-cell activity in the SMA
has shown that many cells change their
activity in relation to sensory stimulus (light,
passive movements, etc) that the animal
knows its signal to start a certain voluntary
movement.
The SMA is important for organizing and
planning fairly complex movements and for
mediating an appropriate motor response to
sensory stimuli.
The Premotor Cortex (PM), largest part of area 6.
Sends fewer fibers to the spinal cord than SMA but has strong
connections with the RF, red nucleus, basal ganglia. It has
important projection to M1.
The PM is important for the control of visually guided movements,
such as the proper orientation of the hand and fingers when they
approach an object to be grasped.
After damage to the M1, the handling of an object is clumsy and
insecure, but the ability to avoid an obstacle is not lost.
Connections from the extrastriate areas in the occipital lobe to the
PM are necessary for the ability to perform such goal directed
movements.
In agreement with the above observations, single-cell recordings
show that many cells in the PM change their activity about 60
msec after a light signal that the monkey is trained to respond to
with a certain movement.
In the acute stage after a stroke, patients with lesions of the SMA
reach out and grasp objects with the affected arm, even when
they have been told to refrain from moving.
This alien hand syndrome reflects a dominance of externally
guided lateral PM pathways. The sight of an object within reaching
distance evokes a motor plan to grasp an object. We usually can
inhibit movement if we are instructed to do so or if the movement
is inappropriate. But when internal control sources are removed,
the movement can be triggered by appropriate external stimulus.
Posterior Parietal Cortex
Many neurons are active in relation to movements in the posterior
parietal cortex (area 5, 7).
One kind of neuron is active before goal-directed, reaching
movements, such as when a monkey stretches its hand toward a
banana. Such neurons do not become active, however, in relation
to movement in the same direction but without a specific aim, or in
relation to a passive movement.
Other kinds of neurons increase their activity in relation to
exploratory hand movements, such as when a monkey studies a
foreign object.
In area 7, some neurons increase their activity only when the
monkey stretches the hand toward an object that it also looks at.
In humans, lesions of the posterior parietal cortex may, for
example, make them unable to open a door or to handle previously
familiar tools. Such persons also have difficulties with proper
orientation of the hand with relation to an object, and they easily
miss an object even though they see it clearly. This kind of
symptom is called apraxia.
Recent studies, using both single-cell recordings with primates
and brain imaging techniques suggest that parallel circuits may be
involved in motor planning. One circuit, including the parietal lobe,
lateral premotor and cerebellar pathways is essential for producing
spatially directed or guided movements. These regions are active
during the early stages of skill acquisition. A second circuit,
associated with the SMA, basal ganglia and perhaps the temporal
lobe, becomes more dominant as the skill is well learned and
driven by the internal representation of the desired action. Both
circuits converge on the motor cortex, the primary link between the
cortex and limbs for voluntary movements.
Vestibular reflex
: evoked by changes in the position of the head
: evoked by otolith organs
a) Vestibulocollic reflexes (act on the neck), counteract head movements, keeping the head stable
b) Vestibulospinal reflexes (act on the limbs)
: extension of arms, flexion of the lower limbs
c) Vestibulo-occular reflexes: stabilize images on the retina.
Neck Reflexes
: triggered by tilting (bending) or turning the neck
a) Cervicocollic reflexes: if neck pushed to one side, opposite
neck muscle contracts, to restore normal neck postition,
synergistic with vestibulocollic reflexes
b) Cervicospinal reflexes
*bending the neck forward==> flexion of the upper & lower
extremities
*tilting the neck backward==> extension of the upper & lower
extremities
*turning to right==> extension of right arm & leg (flexion of left
limb)
*** Vestibular and neck afferents converge on the Vestibular
Nuclei & Propriospinal Neurons
Asymmetrical Tonic Neck Reflex
Balance between basal ganglia
and cerebellum
The balance between these two
systems allows for smooth,
coordinated movement, and a
disturbance in either system will
show up as movement disorders
Damage to the basal ganglia results in:
Abnormal body movements:
-Tremor (uncontrollable shaking)
-Involuntary movements of the skeletal
muscles
-Paralysis – Akinesis: (destruction of the
caudate (most affected site in stokes)
results in paralysis in the opposite side
of the body).
-Globus pallidus: mostly concerned with
muscle tone for specific body
movements.
-Lesion in the subthalamic nucleus –
hemiballisms, jerky movements,
spontaneous movements of the arms
(affects the extremities – legs and arms)
most
symptoms do not appear until
striata DA levels decline by at least 7080%.
Imbalance primarily between the
excitatory neurotransmitter Acetylcholine
and inhibitory neurotransmitter
Dopamine in the Basal Ganglia
movement, motivation, reward, and addiction
Major Symptoms Involve
-tremor
is most apparent at rest.
-Rigidity
is a result of simultaneous
contraction of flexors and extensors, which
tends to lock up the limbs.
-Bradykinesia,
or "slow movement", is a
difficulty initiating voluntary movement, as
though the brake cannot be released.
Postural Instability - abnormal fixation
of posture (stoop when standing),
equilibrium, and righting reflex
Other Accompanied Autonomic Deficits Seen Later in Disease Process
•
•
•
•
•
Hypotension
Dementia
Dystonia
Ophthalmoplegia
Affective Disorders
Etiology
• Cerebral atherosclerosis
• Viral encephalitis
• Side effects of several antipsychotic
drugs (i.e., phenothiazides,
butyrophenones, reserpine)
• Pesticides, herbicides, industrial
chemicals - contain substances that
inhibit complex I in the mitochondria
Putative Functions of the Basal Ganglia
Motor Functions
initiates motor patterns of cognitive or motivational significance (Heimer et al. 1982)
motor sequence planning, coordination (Graybiel 1995)
inhibition of competing motor programs (Mink 1996)
Sensory functions
somatosensory motor control (Schneider & Lidsky 1981, Brown et al. 1997)
somatosensory discrimination; pain (Brown et al. 1997);
visual discrimination (Pribram 1977) including facial expression and hallucinations (Middleton and
Strick 1996, Brown et al. 1997)
auditory (Brown et al. 1997)
Cognitive functions
cognitive sequence planning ("acquisition, retention, and expression of cognitive patterns" Graybiel
1997)
expectations, prediction (ventral striatum, Schultz 1998)
attention (Hayes et al. 1998)
categorizing (tactile stimuli, Merchant et al. 1997)
learning (Jueptner et al 1997); procedural memory (for habits and skills: Jog et al. 1999)
habit learning & acquisition of "non-motor dispositions and tendencies (Knowlton et al. 1996)
classify spatial patterns and serial ordering of sensory events (Beiser & Houk 1998)
executive function (". . . focused and sustained attention in concert with flexibility of thought . . .
planning and regulation of adaptive and goal directed behavior . . . [utilizing] working memory . . ."
Peigneux 2000)
creativity (ventral striatum becomes activated when predictions are violated by stimuli that appear in
an unexpected context: references in Cotterill 2001)
Neurotransmitters
Serotonin
Acetylcholine
GABA
Enkephalin
Substance
Glutamate
Dopamine
P
Parkinson's disease: Treatment
Its symptoms and potential therapies were mentioned in the
Ayurveda, the system of medicine practiced in India as early as
5000 BC
in the first Chinese medical text, Nei Jing, which appeared 2500
years ago.
Drug Therapy Against Parkinson Disease Is Aimed at Bringing the
Basal Ganglia Back to Balance
Decrease Cholinergic Activity Within Basal Ganglia and this
Can Be Done Two Ways:
Activating Dopamine receptors in Substantia Nigra feeding
back to Cholinergic Cells in the striatum
-Turn off the Cholinergic Cells, Then Things Are Brought
Back to Balance
Antagonize Acetylcholine receptors
Agents that Increase
Dopamine functions
•
•
•
•
Increasing the synthesis of dopamine - l-Dopa
Inhibiting the catabolism of dopamine - selegiline
Stimulating the release of dopamine - amphetamine
Stimulating the dopamine receptor sites directly bromocriptine & pramipexole
• Blocking the uptake and enhancing the release of
dopamine - amantadine
Parkinson's disease: Treatment
Treatment for akinesia: L-Dopa
*decarboxylase inhibitor
*Ach antagonist (atropine)
1. Replacement 2. Substitution, 3. Relase helper 4. Conservation
Increasing the synthesis of dopamine - l-Dopa
Inhibiting the catabolism of dopamine - selegiline
Stimulating the release of dopamine - amphetamine
Stimulating the dopamine receptor sites directly - bromocriptine & pramipexole
Blocking the uptake and enhancing the release of dopamine - amantadine
*fetal dopamine cell transplantation
* destruction of feed-back circuit:
ventrolateral, ventroanterior nuclei
Effects of L Dopa on the
Symptoms of Parkinson Disease
•
L Dopa Fairly Effective in Eliminating Most of the Symptoms
of Parkinson Disease
•
Bradykinesia and Rigidity Quickly Respond to L Dopa
•
Reduction in Tremor Effect with Continued Therapy
•
L Dopa less Effective in Eliminating Postural Instability and
Shuffling Gait Meaning Other Neurotransmitters Are Involved
in Parkinson Disease
•
Many side effects
Glial Cell Line Derived Neurotrophic Factor (GDNF) is Potent Promoting
Survival for Dopaminergic Neurons in Parkinson’s Disease
Neurotrophic proteins-These appear to protect
nerve cells from the
premature death that
prompts Parkinson's. One
hurdle is getting the proteins
past the blood-brain barrier.
Neuroprotective agents-Researchers are examining
naturally occurring enzymes
that appear to deactivate
"free radicals," chemicals
some scientists think may be
linked to the damage done to
nerve cells in Parkinson's
other neurological
Risk of Parkinsonism in smokers is 20-70% lessand
than
non-smokers; nicotine may increase firing rate disorders.
of
dopaminergic neurons
Neural tissue transplants--Researchers are studying ways to
implant neural tissues from fetal pigs into the brain to restore
the degenerate area. In a clinical trial conducted in part at
Boston University School of Medicine, three patients out of 12
implanted with the pig tissues showed significant reduction in
symptoms.
Genetic engineering--Scientists are modifying the genetic code
of individual cells to create dopamine-producing cells from
other cells, such as those from the skin.
Early symptoms of HD
mood swings, depression,
irritability or trouble driving,
learning new things,
remembering a fact, or making a
decision.
The Cause of Huntington's Disease
inherited as an autosomal dominant
disorder
resulting from a mutation on chromosome 4.
expansion of CAG repeats at the end of the gene.
the gene product (the protein huntintin) is not fully
understood. it is known to be expressed ubiquitously and
needed for normal cell survival.
huntinin mutation leads to inappropriate apoptosis,
and destruction of cells.
ACh neuron death at cerebral cortex
Why this cell destruction is differentially targeted to the
basal ganglia and cerebral cortex is not understood.
As the disease progresses,
concentration on intellectual
tasks becomes increasingly
difficult
difficulty feeding himself or
herself and swallowing.
Cerebellum
Involved in the coordination of movement
Compares what you thought you were going to do (according to
motor cortex) with what is actually happening down in the limbs
(according to proprioceptive feedback), and corrects the
movement if there is a problem.
-partly responsible for motor learning, such as riding a bicycle.
-the cerebellum works ipsilaterally.
-now the cerebellum is regarded as a structure that can help not
only motor but also non-motor regions to do their work
effectively.
-compared to a powerful computer, capable of making
contributions both to the motor dexterity and to the mental
dexterity of humans.
-immature at birth but develops through childhood and
adolescence, reaching its full structural growth by the 15th to
20th year of life.
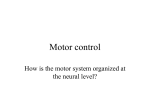
ANATOMY OF THE CEREBELLUM
Lateral
Zone
Intermediate
Zone
Floculonodular Lobe
[Characteristics]
1) contains more neurons than all the rest of the brain combined.
2) a more rapidly acting mechanism than any other part of the brain
3) it receives an enormous amount of information from the highest level of
the human brain (40 million fibers).
Divisions of the cerebellum
Vestibulocerebellum
Input from vestibular nuclei in medulla; output back to medulla, Maintains posture and
balance
Spinocerebellum
Sensory input from periphery; output to descending motor tracts
Compares intended and actual movement and corrects for differences
Cerebrocerebellum
Input from pontine nuclei in pons relayed from cortex; output through thalamus to cortex
Involved in planning and initiation of movement
Cat cerebellum, sagittal section
Single folium, enlarged
The cerebellum ("little brain") has
convolutions similar to those of
cerebral cortex, only the folds are
much smaller.
Like the cerebrum, the cerebellum
has an outer cortex, an inner white
matter, and deep nuclei below the
white matter.
Inputs and outputs of the
cerebellum
3 main inputs, 3 main outputs from
3 deep nuclei. They are:
peduncles, or "stalks". There are 3 pairs: the
inferior, middle, and superior peduncles.
3 inputs are: 1) Mossy fibers from the
spinocerebellar pathways, 2) climbing fibers from the
inferior olive, and 3) more mossy fibers from the
pons, which are carrying information from cerebral
cortex.
The mossy fibers from the spinal cord have come up
ipsilaterally.
The fibers coming down from cerebral cortex,
however, DO need to cross.
The 3 deep nuclei are the fastigial, interposed, and
dentate nuclei. The fastigial nucleus: balance, and
sends information mainly to vestibular and reticular
nuclei.
The dentate and interposed nuclei: voluntary
movement, and send axons mainly to thalamus and
the red nucleus.
The cerebellar cortex has five kinds of
cells.
Basket cell, stellate cell, granule cell,
Purkinje cell, Golgi cell
The cerebellar cortex is arranged in
three layers:
The granular layer (Golgi and
granule cells)
the Purkinje cell layer (Purkinje
cells)
the molecular layer (stellate and
basket cells)
The cerebellar cortex receives
excitatory input through the mossy
fibers and sends inhibitory output from
the Purkinje cells to the deep nuclei of
the cerebellum and the brainstem.
On-beam excitation and off-beam
inhibition occurs because the parallel
fibers of the granule cells stimulate onbeam Purkinje cells but cause the
basket cells to inhibit off-beam
Purkinje cells.
Microcircuits in a
folium
molecular layer is nearly cell-free.
Instead it is occupied mostly by
axons and dendrites.
Purkinje cells, central players in
the circuitry of the cerebellum.
Below the Purkinje cells is a
dense layer of tiny neurons called
granule cells.
Finally, in the center of each
folium is the white matter, all of
the axons traveling into and out
of the folia.
These cell types are hooked
together in stereotypical ways
throughout the cerebellum.
SOMATIC SENSORY PROJECTIONS ONTO
THE CEREBELLAR CORTEX
CEREBELLAR DYSFUNCTION
1. General
a. Disequilibrium - Falling: forward, backward, laterally when standing; unsteady,
staggering gait; sensations of spinning and nausea.
b. Muscle tone disturbance - Softness of muscle bellies on palpation; decreased
tendon reflexes; asthenia (muscles tire easily). Pendular swinging of dependent
limb segment after displacement.
c. Movement disorders
1) Incoordination of movements - Ataxia, asynergia - decreased capability for
smooth, cooperative, segmental action between a series of muscle groups.
2) Decomposition of movements - Complex movement performed as a
sequence of irregular disjointed episodes.
3) Adiadochokinesis - Inability to rapidly pronate and supinate.
4) Dysmetria - Inability to correctly judge distances. Tested by reaching out and
touching an object ("prepointing; pastpointing").
5) Inability to trace a specific course with finger or heel (e.g., right heel to left
knee).
6) Staggering gait - Tendency to fall, particularly with closed eyes.
7) Intention tremor - Tremor when voluntary movement is attempted.
http://video.search.yahoo.com/search/video?p=CEREBELLAR%20DYSFUNCTION%20&ei=UTF-8&fr=yfp-t452&fr2=tab-img
d. Speech deficits - Slow onset, slurring, jerky, intermittent sound productions with
explosive nature: "scanning speech".
e. Cerebellar nystagmus - Inability to fixate on object. Conjugate drift of eyes away
from it, with rapid return. May be positional (more pronounced when body adopts
a particular posture), or directional (increasing when subject attempts to gaze in
particular direction).
CEREBELLAR DYSFUNCTION
2. Specific Syndromes
a. Flocculonodular syndrome:
Loss of whole body equilibrium. Swaying when standing,
staggering when walking, tendency to fall (usually backwards),
positional nystagmus.
http://www.dizzyfix.com/selftest.html#nystagmus
b. Neocerebellar syndrome:
Cerebellar hemisphere (lateral zone) or efferent pathways. In
unilateral disease, manifestations occur on same side as lesion.
Gross intention tremor and staggering gait only supervene if
dentate nucleus or brachium conjunctivum are involved. This
syndrome may include dysmetria, unilateral limb weakness,
adiadochokinesis, intention tremor and speech defects.
The cerebellum was strongly activated in a task involving ocular
pursuit of a target with simultaneous joystick control of a cursor.
Time offsets between eye and hand motion allowed control of the
degree of eye-hand coordination. Only the cerebellum showed
activity changes which co-varied with time offset.
The cerebellum coordinates eye and hand tracking movements.
Nature Neuroscience, 4:638-644.