Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Common raven physiology wikipedia , lookup
Biofluid dynamics wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Homeostasis wikipedia , lookup
Circulatory system wikipedia , lookup
Intracranial pressure wikipedia , lookup
Haemodynamic response wikipedia , lookup
Hemodynamics wikipedia , lookup
Cushing reflex wikipedia , lookup
Cardiac output wikipedia , lookup
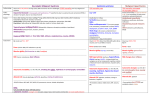
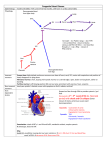
Physiology week 9 – Cardiovascular (flow/BP) Biophysics of blood flow Flow=pressure/resistance Laminar flow Parabolic distribution of velocity – infinitely thin layer next to vessel wall doesn’t move, greatest velocity in centre of stream. This applies up to a critical velocity, above which flow is turbulent. Turbulence Probability of turbulence (and resistance to blood flow) related to diameter of the vessel and viscosity of blood. Reynolds number=probability of turbulence p=density D=diameter V=velocity n=viscosity Plasma is 1.8 times more viscous than water, whole blood is 3-4 times more viscous. Viscosity depends on the haematocrit (percentage of blood volume occupied by red cells). The clinical effect of viscosity differs from that derived from Poiseuille- Hagen formula below. In large vessels, haematocrit increases viscosity. In arterioles, capillaries and venules the effect is less due to the nature of flow in these vessels. Incr turbulence is due to “critical velocity” Smaller diameter Decreased viscosity Velocity Important to differentiate between velocity (displacement per unit time) and flow (volume per unit time) Velocity V=Flow (Q) / cross sectional area (A) Therefore slow in capillaries because much higher cross-sectional area Poiseuille-Hagen Formula Describes basic factors which determine rate of flow of blood through a blood vessel Pressure drop in a fluid flowing through a long cylindrical pipe (assumes flow is laminar, viscous and incompressible) ‘flow varies directly and resistance inversely with the fourth power of the radius’ Critical closing pressure – the pressure within a vessel lumen at which blood flow ceases. Law of Laplace P=T/r (for spherical structure this is 2T/r) W can be ignored in thin walled structures. (transmural P = P inside - P outside – since tissue pressure inside body is negligible, p = pressure inside viscus.) The smaller the diameter of vessel, smaller the tension on wall necessary to balance distending pressure. In heart, dilated ventricle must generate greater tension to produce given pressure therefore work is greater. Arterial and arteriolar circulation Aorta flow is phasic, ranging from 120m/s in systole to negative value in diastole. (average is 40m/s) Arterial flow becomes progressively continuous due to elastic recoil of the vessel walls (Windkessel Effect) though pulsatile flow is necessary for optimal organ function. Pulse pressure – difference between systolic and diastolic pressure Mean pressure – approximation – diastolic pressure plus one third of the pulse pressure. Effect of gravity=0.77mmHg/cm from heart. (if heart=100, head=60, feet=180) 1 Resistance vessels ‘small arteries and arterioles are the principal site of peripheral resistance’. Measurement of Blood Pressure Auscultation Inflatable (Riva-Rocci) cuff attached to mercury manometer, wrapped around arm, stethoscope over brachial artery (at heart level so no effect of gravity) Cuff inflated over expected systolic BP Slowly lower pressure – when SBP just exceeds cuff pressure, spurt of blood passes with each heart beat – tapping sound heart below cuff Lower more – sounds louder then dull and muffled Disappear at diastolic pressure (but diastolic where sound muffled after exercise, in children, hyperthyroidism, aortic insuff) Korotkoff sounds – due to turbulent flow in narrowed, where flow though constriction exceeds critical velocity 1. 1st, snapping heard at systolic pressure 2. 2nd, murmurs heard between systolic and diastolic pressure (unknown significance) 3. 3rd, loud, crisp tapping sound (unknown significance) 4. 4th, within 10mmHg above diastolic, thumping and muting 5. 5th, silence as pressure drops below diastolic If use small cuff – BP incorrectly high Can have auscultatory gap between systolic and diastolic Palpate radial artery for when pulse returns (=systolic), ~2-5mmHg lower than auscultatory method Also can directly measure through arterial line Capillary circulation 5% of blood in capillaries at any one time. Starling Forces Rate of filtration any point along capillary depends on hydrostatic P gradient and osmotic P gradient. Net flow varies between capillary beds. Capillary hydrostatic pressure 30mmHg at arterial end, 10mmHg at venous end Plasma colloid osmotic pressure 28mmHg Interstitial fluid pressure –3mmHg Interstitial fluid colloid osmotic pressure 8mmHg Net outward force at arterial end = (30+3+8)-28=13 Net inward force at venous end = 28-(10+3+8)=7 Pulse pressure 5mmHg arterial end, zero at venous end. Transit time 1-2 seconds. Venous circulation Capacitance vessels A large amount of blood can be added to veins before there is a significant rise in venous pressure Aided by contraction of muscles, negative intrathoracic pressure during inspiration. Venular pressure 12-18mmHg, 5mmHg in great veins of thorax. Normal right atrial pressure is 0mmHg but can vary between –5 and 30mmHg Flow velocity – 10m/s CVP = Rt atrial pressure = 0 (range -5 to +5) Factors that determine CVP 1. balance between venous return and ability of heart to pump out of RA 2. factors affecting venous return: gravity, intraabdominal pressure (pregnancy), hypo/hypervolaemia, venodilation (drugs/fainting), sympathetic tone (vasoconstriction), arteriolar dilation (sepsis, drugs, anaphylaxis), resistance to venous return (tamponade, tumour) 3. factors affecting ability of heart to pump: contractility, hypertrophy (athlete), failure, MI (RV), arrhythmias, AF (volume, filling time and contractility), resistance to RV (Pulm valve stenosis), PE, LVF, hypoxia, tension PTX 2 Venous return Normal value 5-5.5l/min Major factors influencing venous return to the heart: Circulating blood volume Sympathetic and parasympathetic tone Muscle pump Rt atrial pressure (intrathoracic and intracardiac pressure and factors that influence them like phases of respiration, tamponade, PEEP) VR = venous return Psf = mean systemic filling pressure PRA = right atrial pressure RVR = resistance to venous return Relationship between Rt atrial pressure and venous return: 1. Downslope – reduced driving pressure 2. plateau – collapse of vein walls 3. normal value for MSPF = 7mmHg 4. normal value for mean RAP = 0mmHg Halving the resistance allows twice the blood flow – curve up Changes in pressure and velocity as blood flows through the systemic circulation Rapid fall in pressure in arterioles (main site of peripheral resistance) Pressure falls very slightly in large and medium arteries because resistance to flow is small TA (total cross-sectional area) is maximal in capillaries and venules (4.5cm2 in aorta cf 4500cm2 in capillaries) RR (relative resistance) Autoregulation and control of blood pressure ‘autoregulation describes the capacity of the tissues to regulate their own blood supply’ Most vascular beds have intrinsic capacity to compensate for moderate changes in perfusion pressure by changes in vascular resistance so that blood flow remains relatively constant. Myogenic theory of autoregulation – distension of vessel → incr pressure stretches vascular smooth muscle → contraction of muscle Metabolic theory of autoregulation – vasodilator substances accumulate in active tissues → relaxation of smooth muscle 3 Local control Myogenic and metabolic factors Chemical factors Adenosine - released in response to hypoxia. Carbon dioxide, Potassium, Lactate, Histamine Substances released by endothelium Nitric oxide From arginine, activate guanylyl cyclase - produce cGMP - mediate smooth muscle relaxation Release stimulation by Arterial wall sheer stress; Bradykinin; ATP; Parasympathetic nerves Causes dilation of upstream vessels in response to local vasodilation Half life 6 seconds Local vasodilators - Prostacyclin, kinins Local vasoconstrictors - Endothelin, thromboxane, serotonin Hormonal control Vasoconstrictors Circulating adrenaline and noradrenaline Produced by adrenal medulla Both increase force and rate of cardiac contraction Noradrenaline produces vasoconstriction in most if not all organs via alpha1 receptors Adrenaline dilates blood vessels in skeletal muscle and liver via beta2 receptors. Angiotensin II Formed from angiotensin I by the action of renin. Vasoconstrictor, increased aldosterone so incr Na and water retention Renin secretion at any given time is determined by the summed activity of several factors. Angiotensin II feedback Afferent arteriolar pressure decrease results in increased renin secretion. Sodium reabsorption across macula densa decreased absorption causes incr renin Stimulation of beta 1 adrenoceptors by circulating catecholamines - incr renin Increased sympathetic activity via renal nerves. Prostaglandins (especially prostacyclin) stimulate renin secretion. Increases aldosterone secretion and therefore increases reabsorption of sodium and water. Vasopressin/ADH More powerful than angiotensin, from posterior pituitary Actions mostly related to acute haemorrhage/volume loss and control of water reabsorption Vasoconstrictor Endothelins Act in a paracrine fashion and bind to specific receptors. Released in response to endothelial injury Haemodynamic actions Contracts vascular smooth muscle – initial depressor response then pressor response. Cardiac effects Positive inotropic and chronotropic effects. Vasoconstriction of coronary arteries. Neuroendocrine effects Increase levels of ANP, renin, aldosterone, catecholamines. Modulates synaptic transmission. Renal effects Increase renal vascular resistance Decreases glomerular blood flow and GFR Increase sodium reabsorption through haemodynamic actions, decrease sodium absorption by inhibiting sodium potassium ATPase. Respiratory effects Produces bronchoconstriction GIT effects Enhances gluconeogenesis Regulates gastrointestinal blood flow Vasodilators Kinins Bradykinin and lysylbradykinin. 4 Derived from HMW kininogen and LMW kininogen respectively by the action of plasma kallikrein and tissue kallikrein. Tissue kallekrein found in many tissues incl glandular tissue, pancreas, prostate, gut, kidney Kallikrein is activated by factor XII and catalysed by plasmin. Bradykinin and lysylbradykinin are metabolized to active fragments by kininase I. Inactivated by kininase II (ACE). Primarily limited to tissues although also found in circulating blood. Act via bradykinin receptors. Actions Contraction of visceral smooth muscle. Relaxation of vascular smooth muscle Increased capillary permeability Attract leucocytes Serotonin Histamine (from basophils and mast cells) Prostaglandins Prostacyclin (and thromboxane A2) Balance aggregation/vasoconstriction effects of thromboxane and antiaggregation /vasodilation effects of prostacyclin Nervous system control Receptors Baroreceptors Stretch receptors in walls of heart and blood vessels. Carotid sinus (just above bifurcation of common carotid) – pick up rise or fall Aortic arch – pick up rise Stimulated by distension of the structure causing increased rate of discharge. inhibits tonic discharge of vasoconstrictor nerves excites vagal innervation of heart producing vasodilation, venodilation, drop in BP, bradycardia, decree cardiac output Afferents pass via glossopharyngeal and vagus nerves to the medulla. Afferents end on the nucleus of the tractus solitarius resulting in glutamate transmission. Project to the RVLM and stimulates GABA inhibitory neurons. When baroreceptors detect decreased arterial pressure: 1. decr firing rate of Herings nerve 2. CN IX transmits to vasomotor centre 3. decr parasymp outflow to heart 4. incr symp outflow to heart 5. incr symp outflow to vessels 6. incr HR and contractility 7. arteriolar and venous constriction Low pressure receptors in atria and pulmonary arteries Effective in control of sudden volume change - volumer (atrial stretch) reflex Stretch causes Reflex dilatation of afferent arterioles in the kidney Decreased vasopressin/ADH secretion by the hypothalamus Release ANP Tachycardia (direct effect or Bainbridge reflex) Chemoreceptors Play a secondary role in BP control – more active in respiratory control Vasomotor control Vasomotor center in the medulla oblongata. Both vasoconstrictor and vasodilatory areas Neurons project directly to sympathetic preganglionic neurons in intermediolateral gray column of cord. Set point = neutral MAP for vasomotor centre ~100mmHg Inputs Factors affecting the vasomotor center Influenced by peripheral baroreceptors, peripheral chemoreceptors and higher neural centres 5 - NA vasoconstrictor fibres descend from medullary vasomotor centre via spinal cord to smooth muscle in walls of arterioles - Peripheral baroreceptors in carotid sinus and aortic arch respond largely t ochanging BP and act to inhibit vasoconstrictor centre - Peripheral chemoreceptors in carotid bodies and aortic bodies respond to hypoxia and act to excite the vasoconstrictor centre Outputs Vascular innervation Noradrenergic vasoconstrictor fibres Vasoconstrictor fibres some tonic activity – sympathectomy causes vasodilation Sympathetic vasodilator fibres to skeletal muscle Cardiac innervation Noradrenergic sympathetic nerves inotropic and chronotropic action. Cholinergic vagal nerve negative inotropic and chronotropic action Cholinergic fibres have tonic activity (vagal tone) – division of vagus causes tachy Timeline of factors in regulation of arterial pressure Seconds-minutes: baroreceptors, chemoreceptors, CNS ischaemic receptors Minutes-hours: stress (stretch) relaxation, RAS vasoconstriction, blood volume changes and fluid shift through capillaries Longer term: renal compensation via aldosterone, blood volume changes, salt intake Control of HR Factors that incr HR also incr BP, except raised ICP and hypotension/tachy by stimulation of atrial stretch receptors Incr HR: Decr activity baroreceptors in arteries, LV and pulm circulation Incr activity atrial stretch receptors Inspiration, Excitement, Anger, Painful stimuli, Hypoxia, Exercise, Adrenaline, Thyroid hormones , Fever Bainbridge reflex Decr HR: NA Incr activity baroreceptors in arteries, LV and pulm circulation Expiration, Fear, Grief, Stimulation pain fibres in trigeminal nerve, Incr ICP Valsalva response Blood pressure rises at onset of strain due to increase intrathoracic pressure adding to the aortic pressure. Increased intrathoracic pressure causes reduced venous return and cardiac output. This causes tachycardia and increased peripheral vascular resistance. At cessation, intrathoracic pressure returns to normal but peripheral vessels are constricted, causing hypertension, This stimulates baroreceptors and blood pressure is returned to normal by vasodilation and bradycardia. Bainbridge reflex - aka atrial reflex - increase HR due to increase central venous pressure - increased blood volume detected by stretch receptors in atria at venoatrial junctions - Bainbridge reflex and baroreceptor reflex act antagonistically to control HR o baroreceptor reflex incr HR when BP drops/blood volume drops o Bainbridge reflex inc HR when blood volume incr Bezold-Jarisch reflex - causes shallow/slow breathing and bradycardia - prolonged upright posture – pooling in legs – decr intracardiac volume - resultant hypotension – sensed by carotid sinus baroreceptors – triggers autonomic signals increasing HR and contractility - however, pressure receptors in wall and trabeculae of underfilled LV may then sense stimuli and send signals that trigger paradoxical bradycardia and decrease contractility, causing hypotension - usually occurs with nitrates and serotonin agonists Cushing reflex - nervous system response to increased intracranial pressure - results in Cushing's triad - widening pulse pressure, irregular breathing, bradycardia - usually seen in terminal stages of acute head injury, may indicate imminent brain herniation - also be seen after intravenous administration of NA and similar drugs 6 - incr ICP – incr hydrostatic P of CSF until gradually exceeds MAP - cerebral arterioles become compressed, decr cerebral blood supply o chemoreceptors in hypothalamus sense cerebral ischemia (decr pH and incr pCO2) - activation sympathetic nervous system alpha-1 adrenergic receptors in arteries cause vasoconstriction – incr TPR, incr BP to try to maintain perfusion of brain incr contractility and cardiac output o baroreceptors in carotids detect incr BP trigger parasympthetic response via vagal stimulation • bradycardia o also caused by incr ICP impinging on vagal nerve - parasymp response Usually chemoreceptors of brain and baroreceptors of carotid sinuses work together to incr or decr BP In Cushing reflex, two sensors receiving mixed signals - even with sympathetic stimulation, which would normally produce tachycardia, there is bradycardia Pressure-Volume Loop left ventricle Factors determining myocardial O2 demand 1. HR 2. Intramyocardial tension 3. Contractile state of myocardium (OR SV and MAP) Effect of increase in preload or afterload on myocardial demand: Both increase myocardial O2 demand Changes in afterload have greater affect than changes in preload Ventricular work per beat correlates to O2 consumption Work = SV x MAP Stroke work LV is 7x that of RV Theoretically volume changes and pressure changes should affect myocardial O2 consumption equally Pressure work produces greater incr in O2 consumption that volume work (reason not understood) Tension in wall of hollow viscus proportional to radius Myocardial fibres stretched with incr SV in dilated heart Incr radius increases wall tension – incr O2 consumption 7