Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
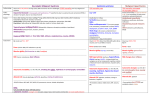
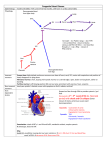
Metabolic Acidosis Severe = pH <7.1 Effects of metabolic acidosis RS: incr RR, shift of Oxy-Hb curve to R (Hb gives up O2) CV: myocardial depression (when pH <7.1), catecholamine release, pul vasoC Met: hyperK (O.5 K : 0.1 pH); hypoCa Neonates and pregnant women esp susceptible due to decr buffering capacity AGMA Incr AG = incr concentration of unmeasured anions (endogenous / exogenous; due to administration of acid or incr production of acid, or decr acid excretion; eg. Phos, SO4, Ca, Mg) Decr concentration of unmeasured cations Incr anions – Decr cations + CATMUDPILERS CO, cyanide Lactic acid Alcohol (ETOH alone will never cause severe met acidosis), alcoholic ketoacidosis Acetoacetate Toulene Hippurate Methanol, metformin Formic / lactic acid Uraemia (ie. Renal failure, aminoglycosides) Uric acid, phosphate, sulphate, Cr DKA Beta-OH-butyrate, glu Paraldehyde, paracetamol, polyethylene glycol Isoniazid / iron / idiopathic / inborn errors of metabolism Lactic acidosis = lactate >2.5; most common cause in ED; pure lactic acidosis in only 10% Lactic acid Type A Tissue hypoxia / hypoperfusion decr oxidative phosphorylation Type B1 Systemic disorders (eg., leukaemia, lymphoma, thiamine def, pancreatitis, short bowel syndrome) Incr production: exercise, seizures, trauma Decr metabolism: hepatic failure, renal failure, hypothermia, DM, sepsis Type B2 Drugs / toxins (eg. ETOH, meth, ethylene glycol, Fe, salicylates, isoniazid, cyanide, CO, metformin uncoupling of oxidative phosphorylation) Type B3 Hereditary metabolic disease (eg. G6PD def) Lactate 2.5-5 = mild = 35% mortality; >2.5 = aerobic capacity exceeded Lactate 5-10 = mod = 75% mortality (severe if >4; NAGMA in 50%) Lactate >10 = severe = 100% mortality Ethylene glycol Glycolic acid, oxylate Rhabdo Salicylates, starvation Salicylate NAGMA Incr AG without acidosis: penicillin, carbenicillin Due to renal and GI bicarbonate loss, or loss of ability to excrete H Cl retained while HCO3 lost incr Cl to maintain electroneutrality USEDCARP Uretersotomy Decr K Small bowel fistula Decr K Extra Cl (ED resus, HCl ingestion, TPN) Incr K Diarrhoea (accounts for >95%) Decr K Resolving DKA Diuretics (K sparing) Incr K Diuretics (eg. Acetazolamide) Decr K Carbonic anhydrase inhibitors Adrenal insufficiency / Addisons Incr K nd Renal tubular acidosis (2 most common cause; decr ability to excrete H in DCT and absorb HCO3 in PCT); other causes = toluene, chronic renal diseases, heavy metal toxicity RTA type 1 (amphotericin, severe hypoK, Sjogrens, SLE, urinary tract obstruction) Decr K RTA type 2 (Fanconi, myeloma, other genetic) Decr K RTA type 4 (hyperK, adrenal insufficiency, rickets, osteomalacia) Pancreatic fistula Decr K Incr K Early ARF usually NAGMA due to HCO3 loss LAGMA <5 Incr cations + Decr anions Mng Increase in unmeasured cations: Lithium, HyperCa / Mg / K, IgG (Multiple Myeloma) Decreased unmeasured anions: HypoAlb / Phos (may mask a AGMA) Chloride over-estimation (anion): Bromide toxicity, Iodide toxicity, Hypercholesterolemia, calculation error Other: nitrites Indications for HCO3: Acidosis (HCO3 <3, pH <7.2) and incr K / Cl ++ 0.5mmol/kg for each desired incr in HCO3; endpoint HCO3 >8 / clinical improvement / pH 7.2; 10-25mmol/hr infusion More likely to be required in NAGMA as 1Y problem is loss of HCO3, as opposed to AGMA where 1Y problem is gain of H Cardiotoxicity due to fast Na channel blockade: TCA OD (severe), type 1a/c antiarrhythmics, cloroquine, propanolol 2mmol/kg IV boluses rpt until stable, then administer as per blood gas results Urinary alkalinisation in OD: salicylate (mod severity not requiring haemodialysis), phenobarb (if continued toxicity despite MDAC), methotrexate 1-2mmol/kg IV bolus 25mmol/hr infusion; aim urinary pH >7.5 Incr urinary solubility: methotrexate, rhabdo Prevention of drug redistribution to CNS (incr unionised amount of drug): salicylate Severe hyperK 50-100mmol (1mmol/kg) slow IV Methanol / ethylene glycol / cyanide / isoniazid >15min cardiac arrest / cardiac arrest in young children or pregnancy HFl acid toxicity RTA Complications of HCO3: extravasation, gastric distension hyperNa, hyperosmolality, alkalosis (pH >7.6 bad for CV function), L shift of O2-Hb diss curve (impaired O2 unloading), hypoK, hypoCa (usually not clinically significant, but if low Ca, then correct Ca before correcting metabolic acidosis to avoid hypoCa); incr lactate production; resp acidosis (ventilation must account for incr CO2 production); paradoxical CSF acidosis; CSF acidosis may be protective and reversal dangerous vol overload, pul oedema In DKA: decr clearance of ketones may precipitate hepatic encephalopathy in susceptible people CI to HCO3: hypoK, hypoCa, alkalosis, acute pul oedema, renal failure, severe hyperNa Notes from: METABOLIC ACIDOSIS (PC02 < 35, HC03 , B.E > -2) ANION GAP (Na + K) – (Cl + HC03) ~ 12 ANIONGAP Due to H which consumes HCO3 NORMAN ANION GAP Due to loss of HC03, generally with Cl hence normal anion gap ACID EXCRETION ARF CRF ACID LOAD 1. Ketoacids DKA Starvation Alcoholic 2. Lactic 3. Exogenous. Check K levels K+ or Normal 1. Mineralot corticoid deficiency. eg: Addision’s. 2. Addition of Cl as the anion of an acid, eg, NH4Cl K 1. Lower GIT losses 2. Renal CA inhibitors RTA 3. Urinary ‘diversion’ Vesico-colic Utero-enterostomy