Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
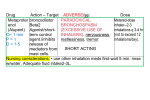
Asthma Definition Pathophysiology Epidemiology Diagnosis Chronic inflamm disorder of airways; variable reversible airway obstruction; bronchial hyperresponsiveness to stimuli Type I HS reaction; BronchoC, mucus hypersecretion, inflamm and oedema, thickening of BM, incr perm, lung overinflation, mucus plugging, SM hypertrophy; subepithelial fibrosis; incr physiological dead space, air trapping and airway obstruction, incr airway resistance, incr airway p, VQ mismatch; cytokines, chemokines, IgE, lymphocytes, mast cells, eosinophils involved 5% adults; 25% children Reversible airway obstruction with >15% improvement in FEV1 (>400ml in adult), FVC, PEFR with beta-agonist; 20% variation in PEFR readings over days-wks; abnormal reactivity with methacholine inhalation stimulation Symptoms Categories 85% >3hrs at presentation; 15% sudden onset; rapid onset = rapid response = less likely admission = less likely infectious trigger; initial response to beta-agonists most accurate measure of severity (not severity of presentation) Triggers: beta-blockers, ACEi, adenosine, aspirin (incr LT’s and bronchial hyperactivity), NSAIDs, sedatives (CI in acute asthma, risk sudden death) RF’s for severe: prev hyperCO2, ICU admits, ED attendances, compliance, on PO steroids in last 6/12, monotherapy with long acting beta agonist, 3+ classes of meds used, old, smoking, psych, social, co-morbidities, heavy beta-agonist use, >50% decr peak flow Mild: short acting beta agonist, low dose inhaler steroid Mod: DD includes… Investigation >75% PEFR, FEV1 50-75% PEFR, FEV1 >95% SaO2 90-95% SaO2 HR 100-120 talks in phrases; mod-loud wheeze; pulsus paradoxus and central cyanosis possible . Severe: long acting beta agonist, high dose inhaled steroid, >50% decr PEFR <40-50% PEFR, FEV1 <90% SaO2 HR >120 (>130 if 2-5yrs) RR >30 (>50 if 2-5yrs) talks in words; quiet wheeze; pulsus paradoxus (>10-20mmHg) and central cyanosis paradoxical chest wall movement; altered LOC; deterioration despite max trt Extremis: ?PEFR/FEV1 <80% SaO2 HR >140 or brady coma FB, carcinoid, PE, eosinophilic pneumonias, systemic vasculitis Bloods: hypoK (inhaled beta agonists decr K by 0.4), hypoP/Mg, hyperG, lactic acidosis, incr WCC (stress, steroids, E; is v common) ABG: should be resp alkalosis (if not, ?impending hypoventilation); PaCO2 >40-42 / PaO2 <60 = life threatening; concurrent metabolic . . acidosis also bad Chronic treatment (in order) Acute treatment (in order) Indications: severe - refractory, SaO2 <92%, monitor resp fatigue, monitor response to trt CXR: barotrauma, atelectasis, pneumonia, hyperinflation, bronchocoeles Indications: 1st presentation asthma, ?pneumonia / barotrauma, pyrexia >39 not explained by viral illness, focal signs not responding to beta agonist, chest pain, long term steroids, failure to respond to aggressive trt, severe resp distress PEFR: easier to measure, cheap, portable, safe; usually 5-10% more than FEV1; if <200ml / 30% predicted, likely pACO2 >40 (max daily PEFR – min daily PEFR) / mean PEFR = diurnal variation = measure of control (20%, poor control; 5% good) FEV1: gold standard; if <1L / 25% predicted, likely pACO2 >40; FEV1, PEFR, RC, FRC all decr with obstructive disease (can’t get air out) ECG: R heart strain, ST/T/P changes; normalise with trt ETCO2: concern if >37-39mmHg; not as sensitive as ABG as air trapping may cause normal ETCO2 Short acting beta agonist: use on >3/7 per wk needs review Low dose inhaled steroid (beclamethasone, budesonide, fluticasone): reduce mortality and hospital admissions; onset <3hrs; prescribe to all patients receiving PO steroids on discharge (either commence, or incr usual dose for 2/52); SE: oropharyngeal candidiasis Long acting beta agonist (eformoterol, salmeterol): DOA 12hrs Med – high dose inhaled steroid Incr dose of LABA and steroid Others: chromolyns (in exercise-induced asthma as prophylaxis), LT receptor antagonists O2: Effects: reverses hypoxic pul vasoC, reverses bronchoC, protects against decr pO2 from beta agonist Dose: use in all except mild; humidify to prevent bronchoC from dry gas; high flow O2 has been shown to worsen outcome, so stick to endpoints below Endpoint: aim SaO2 >92% Short acting beta agonist (salbutamol, terbutaline) Effect: bronchoD, incr ciliary activity, decr mediator release Onset: 3-5mins, DOA 3hrs Dose: 8 puffs spacer = 5mg (with optimal technique, 15% reaches lungs) NEB = equivalent effect; use 6 puffs regardless of age Q20minly NEB: Pros: not temp dependent; doesn’t require patient co-operation; continuous nebs recommended in severe Cons: delivery depends on RR and TV; only 55% dose nebulised, 33% nebulised, is inhaled; 20% dose overall delivered IV: Pros: use if can’t do inhaled (eg. Coughing ++) or refractory / life-threatening Cons: no benefit over INH, more autonomic SE’s 500mcg (10mcg/kg) IV bolus over 2mins repeat dose at 10mins if not improving 1-20mcg/kg/min infusion (start at 5-10mcg/kg/min for 1hr in children, then reducing down to 1-2mcg/kg/min) SE: tremor, headache, lactic acidosis, hypoK, hypoG, cramps, insomnia, tolerance; cause vasoD of poorly aerated areas therefore incr VQ mismatch Anticholinergics: use in mod-severe asthma, COPD, mod asthma in children; best in combination with beta agonist, otherwise poor effect Onset: 20mins, peak 2hrs, DOA 6hrs Dose: Ipratropium: 4 puffs via spacer, or 250mcg neb (add to 2nd neb); Q20minly for 3 doses, then Q4hrly; give Q20minly in severe SE: dry mouth, cough, blurred vision, glaucoma; no advantage to continuing after 1st 24hrs Steroids: early use decr hospital admission, relapse rate, beta agonist use Effects: decr inflamm, secretions, reactivity, mediators; incr beta receptor no, function and sensitivity Onset: 2-6hrs, DOA 24hrs Dose: Use IV if severe (PO absorption compromised); 10-14/7 course for adults (shorter if sudden onset, rapid response), 3-5/7 for children; tapering not required unless on maintenance steroids / >2/52 course Prednisone 25-50mg (1mg/kg) PO OD Dexamethasone 4-8mg (0.1mg/kg) IV – IV drug of choice Hydrocortisone 100-200mg (4mg/kg) IV – has mineralocorticoid effects / SE’s (HTN, hypoK, met alk, Na retention) MgSO4: severe refractory asthma; decr admission and improve FEV1 Effects: improves lung function; prevents tachyphylaxis to beta agonists, bronchoD, anti inflamm; safe Dose: 1.2-2g (25-50mg/kg) IV over 20mins one-off dose monitor levels and for toxic adverse events; inhaled is safe but lack of clear benefit for use SE: flushing, hypoT, sweating, N, sedation, arreflexia in toxicity Aminophylline: severe asthma refractory to above; role in children but not adults (unless COPD) Effects: bronchoD, CNS and cardiac stimulation, incr skeletal muscle contractility, diuretic, incr gastric secretion Dose: 6mg/kg (ideal body weight) (10mg/kg in children, max 500mg) loading dose IV over 60mins (NOT if on PO; if on PO, get serum level) 0.5-1mg/kg/hr infusion Pharmacology: factors increasing clearance = fags, phenytoin, carbamazepine, phenobarb; factors decreasing clearance = pul oedema, hepatic/renal probs, erythromycin, cipro Endpoint: goal is level 10-14mg/dL SE: anxiety, N+V, headache, ectopics, multi-focal atrial tachycardia, seizures Adrenaline: life threatening refractory to above; imminent cardioresp arrest Effects: alpha properties help airway oedema, beta cause bronchoD SE: hypoK, arrhythmia, lactic acidosis CI: cardiac disease, >40yrs NIV: may prevent/delay mechanical ventilation, decr WOB, bronchoD, decr airway resistance, decr CV impact of changes in p’s caused by asthma Dose: BiPAP (12:6 to start, 12-18:6-12 titrate) best requires less sedation, doesn’t require paralysis, preservation of airway reflexes, less pneumonia; may need 0.05-0.1mg/kg midaz or 0.5-1mg/kg ketamine to tolerate RSI: only intubate if life threatening and max therapy failed; 10-20% mortality if tubed; trial of apnoea if cardiac arrest Indications: cardiac / resp arrest or pre-arrest, profound decr RR, exhaustion, decr LOC, severe decr pAO2, severe resp acidosis despite trt Aims: limit PAP, avoid gas trapping permissive hypercarbia to help this (prevents barotrauma; CI if incr ICP / severely impaired myocardial Fx; risk of cerebral oedema, decr myocardial contractility, vasoD, pul vasoC, post-arrest; can give NaHCO3 if pH <7.2 and don’t want to change ventilator settings) Technique: Give IVF 20ml/kg bolus pre-intubation to minimise risk of hypotension Induce sitting up, ventilate by hand Lignocaine 1.5mg/kg 3 mins pre-induction to decr laryngospasm Ketamine: sympathomimetic and bronchoD SE: hypersecretion, hypotension/HTN, CI in IHD, HTN and incr ICP 2mg/kg IV induction bolus 2-3mg/kg/hr INF (may prevent need for ETT; intubating agent of choice but no proven benefit from ongoing treatment) Propofol: short acting, bronchoD, good if HTN SE: vasoD, hypotension esp if vol replete Volatile anaesthetics: may cause bronchoD, helpful in ICU (eg. Isoflurane, halothane) Sux 2mg/kg or roc 1mg/kg Vec 0.1mg/kg/hr Salbutamol via ETT: 1-2ml neb solution diluted to 5ml; continuous nebs using 2-4x dose (as ETT is barrier to delivery) Hand ventilate place on volume cycled ventilator once airway p and TV acceptable FiO2 1.0 (titrate to O2 goals), RR 6-8 (titrate to lowest tolerable pH), TV 5-8ml/kg (6-10ml/kg in children), I:E 1:5 or more (titrate to airway p’s; may not be possible on oxylog 3000); minimal PEEP, PIP <40-45, target plateau pressure <20 Heliox: at least 70% (therefore can’t deliver high conc O2 when using); lower density, decr resistance, decr WOB, improve nebulisation, decr resp distress, incr GE; in severe refractory asthma to avoid ETT External chest compression: decr air trapping, in extremis, cardiac arrest Admit if: ICU if: Discharge if: Discharge advice Pregnancy Pre-treatment PEFR <25-30% SaO2 <92% Post-treatment PEFR <40% (or -60% if not improving well over few hours) Child needing spacers <3hrly despite 4-6hr trt in ED Also consider: social factors, geographical factors, co-morbidities, previous asthma history Altered LOC; exhaustion; marked decr AE; incr pCO2 despite trt; high RF; failure to improve despite trt; intubation needed; multiple co-morbidities; need for ongoing intensive trt Post trt PEFR >60% (-40% if doing well) ASS 0-2 Adequate social circumstances etc…. Observe for 30-60mins after most recent bronchoD dose Combined use PO and INH steroids; written action plan (how to recognise Sx, mng of exac, how to gain medical attention, clear FU instructions); close FU; patient and family education; review preventative treatment; check inhaler technique Assoc with pre-eclampsia, prem, LBW, CS; worsens in 1/3, improves in 1/3, stays same in 1/3; exac most common in 2nd and 3rd trimesters; PEFR and FEV1 not changed much; steroids OK in acute; beta agonists and budesonide safe PaCO2 >35, PaO2 <70 worrying in pregnancy Cardiac arrest Referral Admission: SaO2 <95%, FEV1 / PEFR <70%, any fetal compromise Trial of apnoea; external chest compression; volume challenge; adrenaline; treat complications No GP; newly diagnosed asthma; change in medications; >2 ED attendances in 6/12; >2 admissions in 1yr; non-compliance; >4 courses of PO steroids per year Notes from: Dunn, Cameron (adult and paed), TinTin, Starship guidelines