Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
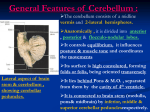
The Cerebellar Connections By Prof. Dr. Muhammad Imran Qureshi Intracerebellar Nuclei The intracerebellar nuclei (also called central nuclei) are masses of grey matter embedded in the white matter of the cerebellum. They are four in number on each side of the midline. From lateral to medial side these are: The Dentate nucleus, The Emboliform nucleus, The Globose nucleus, and The Fastigial nucleus. The Dentate nucleus This is the most prominent of the intracerebellar nuclei. It is largest in primates, especially in humans. It is also known as the nucleus of Neocerebellum and therefore receives afferent fibres from it. In sections, its shape resembles a crumpled (wrinkled) bag with its hilum facing anteromedially. The interior of the nucleus is filled with white matter made up of efferent fibres that leave the nucleus through the hilum. These fibres form most of the superior cerebellar peduncle. These fibres include dentatorubral and dentatothalamic fibres relaying in the red nucleus and ventral lateral nucleus of the thalamus respectively. Fibres from red nucleus project to the spinal cord. Fibres from the thalamus project to the cerebral cortex. The Emboliform nucleus This nucleus is oval in shape. It is located medial to the dentate nucleus, partially covering its hilum. It is also known as the nucleus of paleocerebellum, therefore receives afferent fibres from it. The effrents fibres from this nucleus pass to the red nucleus via superior cerebellar peduncle. From the red nucleus the fibres pass to the spinal cord through rubrospinal tract, and facilitates the flexor muscle tone. The Globose nucleus This is the smallest of the intracerebellar nuclei. It is rounded in shape and lies between the emboliform and fastigial nuclei. Its connections are similar to those of the emboliform nucleus. The globose and emboliform nuclei are sometimes collectively known as the nucleus interpositus. The Fastigial nucleus This nucleus is located near the midline in the cerebellar vermis being close to the roof of the fourth ventricle. It is smaller than the dentate but larger than the emboliform nucleus. It is also known as the nucleus of archicerebellum, hence receives afferent fibres from it i.e. from the flocculonodular lobe. Efferent fibres from this nucleus are conveyed to the vestibular and reticular nuclei. These fibres influence the extensor muscle tone. WHITE MATIER OF THE CEREBELLUM The white matter of cerebellum is made up of three types of fibres: The Intrinsic fibres, The Afferent fibres, and The Efferent fibres. The intrinsic fibres remain confined to the cerebellum. They connect different regions of the cerebellum either within the same hemisphere or the area of one cerebellar hemisphere with that of the other. The afferent and efferent fibres connect the cerebellum with other parts of the CNS. CONNECTIONS OF CEREBELLUM Afferent Fibres The cerebellum receives input through afferent fibres mainly from cerebral cortex, spinal cord, and vestibular apparatus (saccule, utricle and semicircular canals). In addition it also receives input from red nucleus and tectum of the midbrain. The cerebral cortex sends information to the cerebellum, through corticopontocerebellar, cerebroolivocerebellar, and cerebroreticulocerebellar pathways. The spinal cord sends subconscious proprioceptive information to the cerebellum via the posterior spinocerebellar, anterior spinocerebellar, and cuneocerebellar tracts. The spinocerebellar tracts form the major sensory input. The afferent fibres from vestibular apparatus pass to the cerebellum either directly or after relaying in the vestibular nuclei. Afferent Fibres The afferent fibres enter the cerebellum mainly through the inferior and middle cerebellar peduncles. They are classified into two types: Climbing fibres, and Mossy fibres. The Climbing fibres originate mostly in the inferior olivary nucleus. After giving a collateral to the intracerebellar nucleus, each fibre, makes a monosynaptic contact with the Purkinje cell. Afferent Fibres The Mossy fibres constitute the bulk of the afferent fibres of the cerebellum. Each mossy fibre ends by forming 30 to 40 terminal swellings called rosette. Each rosette forms synaptic contacts with dendrites of granule cells and axons of few Golgi cells. The rosette and its synaptic contacts with dendrites of granule cells and axons of Golgi cells forms the cerebellar glomerulus. Each glomerulus appears spherical or ovoid in shape and is surrounded by a capsule of neuroglial cells. The climbing fibre synapses directly with a single Purkinje cell while mossy fibre synapses with thousands of Purkinje cells through granule cells. One mossy fibre synapses with several granule cells, then each granule cell synapses with thousands of Purkinje cells through parallel fibres). Therefore one climbing fibre specifically influences only one Purkinje cell, whereas the influence of a mossy fibre is far more diffuse. The influences of both climbing, and mossy fibres are excitatory to the Purkinje cells. Note that All the afferent fibres of the cerebellum are mossy fibres except olivocerebellar (from inferior olivary nucleus) and par olivocerebellar fibres (from accessory olivary nuclei) which are climbing fibres. The cerebellum receives all kinds of sensory impulses but has got nothing to do with the conscious appreciation of these impulses. (A function of the cerebral cortex) Efferent Fibres The efferent fibres from cerebellum pass to the red nucleus, thalamus, vestibular complex, and reticular formation. The entire output of the cerebellar cortex is through the axons of the Purkinje cells. Most of the axons of Purkinje cells end by synapsing with the neurons of intracerebellar nuclei. The axons of neurons of intracerebellar nuclei in turn project to the other parts of the nervous system. However a few Purkinje cell neurons from flocculonodular lobe and vermis pass directly out of cerebellum to end in the lateral vestibular nucleus. The fibers from dentate, emboliform and globose nuclei leave the cerebellum through the superior cerebellar peduncle. The fibers from the fastigial nucleus leave the cerebellum through inferior cerebellar peduncle. Intrinsic neuronal circuitry in the cerebellum All the afferent fibres to the cerebellum (i.e. mossy and climbing fibres) are excitatory to the cells of cerebellar cortex and their collaterals are excitatory to the intracerebellar nuclei. The climbing fibres excite Purkinje cells directly. On the other hand mossy fibres excite the Purkinje cells indirectly through the granule cells. In addition to Purkinje cells, the granule cells also excite the adjoining basket and stellate cells which in turn inhibit the Purkinje cells-a neural sharpening mechanism. The mossy fibres also excite the Golgi cells which provide the feedback inhibition to the granule cells. The Purkinje cells exert an inhibitory influence on the neurons of the intracerebellar nuclei which in turn modify the muscular activity through the motor control areas of the brainstem and cerebral cortex. Points to Note: All the cells in the cerebellar cortex are inhibitory except the granule cells which are excitatory. The Purkinje cells are the only neurons in the cerebellar cortex which are capable of transmitting efferent impulses. CEREBELLAR PEDUNCLES On each side the afferent and efferent fibres of the cerebellum are grouped together into three large bundles called cerebellar peduncles. The superior cerebellar peduncles connect the cerebellum to the midbrain. The middle cerebellar peduncles connect the cerebellum to the pons, and The inferior cerebellar peduncles connect it to the medulla oblongata. Each inferior cerebellar peduncle is formed on the posterolateral aspect of the upper half of the medulla oblongata. The two peduncles diverge as they ascend and pass into their respective cerebellar hemispheres. Each peduncle consists mainly of afferent fibres from the spinal cord, the olivary nuclei, the reticular formation of the medulla and the vestibular nuclei and nerve to the cerebellum. It also transmits efferent fibres from cerebellum to the medulla, mainly to the vestibular nuclei, and the reticular formation. The middle cerebellar peduncle is the largest of the three peduncles. On either side it arises from the posterolateral region of the pons and becomes continuous with the white matter of the cerebellar hemisphere. Each peduncle contains only afferent fibres, which transmit the impulses from pontine nuclei to the opposite cerebellar hemisphere. These fibres are called the pontocerebellar fibres. The pontine nuclei receive the impulses from ipsilateral cerebral cortex. The superior cerebellar peduncle emerges from the anterior cerebellar notch and runs superiorly, running lateral to the upper half of the fourth ventricle, to enter the lower part of the midbrain. It is the principal efferent pathway from the cerebellum and its fibres arise mainly in the dentate nucleus. Inferior Cerebellar Peduncle Afferent fibres Posterior spinocerebellar fibres from ipsilateral thoracic nucleus (Clarke's column). Olivocerebellar fibres from opposite inferior olivary nucleus. Par olivocerebellar fibres from medial and dorsal accessory olivary nuclei. Cuneocerebellar fibres (posterior external arcuate fibres) from ipsilateral accessory cuneate nucleus. Anterior external arcuate fibres from arcuate nuclei of both the sides. Vestibulocerebellar fibres: primary from vestibular nerve and secondary from medial and inferior vestibular nuclei. These fibres form juxtarestiform body. Reticulocerebellar fibres from lateral and paramedian reticular nuclei of the medulla oblongata. Efferent fibres Cerebellovestibular fibres from ipsilateral flocculonodular lobe and fastigial nuclei of both sides. These fibres pass through juxtarestiform body. Cerebelloreticular fibres from fastigial nuclei of both sides to the pontine and medullary reticular formation. Cerebello-olivary fibres of uncertain origin connect the cerebellum with the inferior olivary nucleus. Middle Cerebellar Peduncle Afferent fibres Pontocerebellar fibres form the bulk of this peduncle. These fibres arise from pontine nuclei, run transversely, cross the midline and enter the opposite cerebellar hemisphere (neocerebellum). The pontine nuclei receive input from the cerebral cortex, thus forming cortico-ponto-cerebellar pathway. Reticulocerebellar fibres from reticular formation of brainstem of the same side are projected to the vermal region of the cerebellum. Efferent fibres No efferent fibres pass through the middle cerebellar peduncle. Superior Cerebellar Peduncle Afferent fibres Anterior spinocerebellar tract. It is major afferent pathway. Tectocerebellar fibres from tectum of midbrain (superior and inferior colliculi of both sides). Trigemino cerebellar fibres from superior sensory and spinal nuclei of trigeminal nerve. According to some authorities, these fibres pass through inferior cerebellar peduncle. Ceruleocerebellar fibres. These are nonadrenergic fibres from locus ceruleus. Hypothalamocerebellar fibres. These are few in number and are cholinergic fibres from hypothalamus. Efferent fibres Cerebellorubral fibres: They arise mainly from globose and emboliform nuclei and project to the contralateral red nucleus. Dentatorubral and Dentatothalamic fibres arise from dentate nucleus and project to the opposite red nucleus and thalamus respectively. Cerebello-olivary fibres: These arise from dentate nucleus and pass to the opposite inferior olivary nucleus. Cerebelloreticular fibres: They arise from the fastigial nucleus and pass to the reticular nuclei. COMPARATOR FUNCTION OF THE CEREBELLUM The cerebellum plays a key role in accomplishing smooth and coordinated movements by means of its comparator function. If the cerebral cortex decides on a movement to take place, the impulses from motor cortex stimulate the anterior horn cells (LMNs) of the spinal cord to initiate voluntary movement. At the same time, the motor cortex informs the cerebellum about the intended movement. The cerebellum also receives proprioceptive information from muscles and joints, informing it about the movement that is actually taking place. The cerebellum now compares the intended movement with the actual movement that is taking place. If a difference is detected, the cerebellum sends the information to the motor cortex and lower motor neurons to correct the discrepancy. This results in smooth and coordinated movement i.e. the movement produced is accurate with reference to time, rate, range, force, and direction. With training, a person can develop highly skilled and rapid movements. The cerebellum thus plays an important role in learning of motor skills. ARTERIAL SUPPLY OF THE CEREBELLUM The cerebellum is supplied by 3 pairs of cerebellar arteries: Superior cerebellar artery, a branch of basilar artery supplies the superior surface of the cerebellum. Anterior inferior cerebellar artery, also a branch of basilar artery supplies the anterior part of the inferior surface of the cerebellum. Posterior inferior cerebellar artery, a branch of vertebral artery supplies the posterior part of the inferior surface of the cerebellum. Cerebellar Lesions The cerebellar lesions may occur due to trauma, vascular occlusion, tumours, etc. They produce a number of signs and symptoms, which together constitute the cerebellar syndrome. The signs and symptoms produced by cerebellar lesions are as follows: The involvement of archicerebellum will lead to: Trunkal ataxia and staggering gate: The patient is unsteady while standing and staggering while walking [he walks with legs well apart (i.e. on a wide base) and sways from side to side]. Nystagmus: The involuntary, to and fro, oscillatory movements of the eyeballs while looking to either side (Rhythmic oscillations of the eyeballs) N.B. The patient is unable to maintain a steady posture with the feet close together, after the eyes are closed because of loss of proprioceptive input (Romberg’s sign). The involvement of paleocerebellum will lead to diminished muscle tone (hypotonia asthenia) of limb muscles. This manifests in the form of: Lack of stability of joints (flail joints). Disturbances of tendon reflexes, e.g. tapping of patellar tendon produces oscillating movements of the leg (i.e. leg swings backwards and forward) called pendular knee jerk. Inability to maintain balance while walking (ataxia). The involvement of neocerebellum leads to muscular incoordination called asynergia. This manifests in the form of: Dysmetria, i.e. inability to measure the distance correctly for reaching an intended target, described as past-pointing. Clinically this is tested by the finger-nose test. If the patient is asked to touch the tip of his nose by his finger, he either undershoots or overshoots the tip of his nose. When patient tries to correct the mistake, it results in to and fro movements. Intention tremors (probably due to dysmetria). The tremors occur during purposeful movements and disappear with rest. Adiadochokinesis/dysdiadochokinesis, i.e. inability or difficulty to perform alternate or succesive movements in rapid succession, e.g. pronation and supination of the forearm. Dysarthria or scanning speech: The speech is slurred, prolonged, explosive and with pauses in wrong places. Rebound phenomenon The patient is unable to check the action of agonist muscles by the corresponding antagonist muscles. If the patient is asked to push the palm of a doctor by his palm, the force that the patient can develop slowly rises and now if the doctor suddenly removes his hand, the limb of patient flies back (i.e. rebounds) and hits against his chest because he is not able to stop his pushing act immediately. The lesions of cerebellar hemisphere give rise to signs and symptoms on the side of lesion as each cerebellar hemisphere is connected by nervous pathways with the same side of the body. The cerebellum and basal ganglia both control motor functions but have opposite effects, and many signs and symptoms associated with their dysfunction are also opposite. For example, cerebellar dysfunction results in decreased muscle tone and an intentional tremor, whereas the dysfunction of basal ganglia results in increased muscle tone and resting tremor.