Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Endocrine disruptor wikipedia , lookup
Sexually dimorphic nucleus wikipedia , lookup
Triclocarban wikipedia , lookup
Sex reassignment therapy wikipedia , lookup
Xenoestrogen wikipedia , lookup
Hypothalamus wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
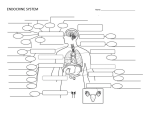
January 18th: Lecture 5 The Pancreas Located right next to the liver. Consists of the Exocrine and Endocrine Pancreas Endocrine Pancreas contains Islets of Langerhans (important for hormonal regulation) which produces insulin, glucagon, somatostatin and pancreatic polypeptides. The pancreas is associated with cellular nutrition and the balancing of glucose levels. If this fails you suffer from diabetes mellitus. This was the first endocrine disorder noted in history. Before you could treat it with insulin, diabetes was fatal. Diabetes Mellitus B cells in the Islets of Langerhans produce Insulin (45 units of insulin per day). Frederik Banting and Charles Best Diabetes Type I – no insulin production Diabetes Type II – little or insufficient production and high tissue insulin resistance. Adrenal Glands Regulated by ACTH. Attached superiorly to the kidneys. Consists of the Adrenal Cortex (Cortisol, aldosterone, androgens, estrogens) and the Adrenal Medulla (adrenaline, noradrenaline, dopamine, enkephalins). Adrenal insufficiency associated with metabolic effects of the hormones of the adrenal glands. Hypo activity is linked to weakness, fatigue, nausea, weight loss, low blood pressure. Hyperactivity is linked to obesity and high blood pressure. The Gonads Two distinct systems (male/female) Regulated by FSH and LH from the pituitary. Manufactures the sex cells (the gametes), and are responsible for the development of secondary sexual characteristics. Produces androgens, estrogens and progestins. Female Ovaries Contains a cortical layer that produces ovarian hormones (estrogens, androgens and progesterone). Menstrual Cycle: menses, follicular and luteal. Follicular phase: maturing of the follicles, regulated by estrogen. Once a certain level is reached LH causes follicle to release egg. Luteal phase: rupture follicle becomes corpus luteum. If egg is not fertilised, levels of hormone fall. Menses occur. Male Testes Endocrine glands are housed in the scrotum. Housed there for temperature maintenance and protection. Sperm must be housed a little below body temperature. The hormone producing units are called Leydig cells. Testosterone, dihydrotestosterone, estradiol, dehydroepiandrosterone, estrone, progesterone and androstenedione. It is the main regulator of male sexual behaviour, and also involved with energy and production of red blood cells and sperm. Female and Male gonads both produce the same hormones, just in different quantities. Summary: Endocrine systems consist mostly of glands in the body which secrete specific hormones that have a variety of effects throughout the body. These glands are mostly controlled by hormones from the pituitary. The pituitary hormones are mostly controlled by hormones from the HT. Exceptions: Some glands do not follow this scheme i.e. pancreas and the pineal glands in the CNS are not under the control of the HT or PT. What controls the HT? Whatever controls our emotions has a lot to do with the regulatory input into the hypothalamus. What our endocrine glands are doing has a lot to do with the activity of the limbic system which is our emotional regulatory centre. Do we have control over the limbic system? Divided topic. Organisational Hormone Action Pre and early postnatal development. These hormones sculpt neural and behavioural systems. These changes are permanent and irreversible and can only occur during critical development periods and can lead to permanent structural/physiological changes and are asymmetric with regards to the sexes. Activational Hormone Action Not permanent. After in development. No critical development periods. More subtle changes. Believed to be symmetrical. Example of organisational hormone effect: finger-length ratio Ratio of index finger (2) to ring finger (4). Determined during weeks 13 to 14 of gestation. There are three possibilities 2 < 4, 2 = 4, 2 > 4 The longer your ring finger is indicates you were exposed to more androgens (e.g. T) while in the uterus. Greater ring finger length indicates greater male characteristics. Differences between the NS and the ES Neural communication is fast, Endocrine communication is slower (via bloodstream). NS is either on or off (action potentials) whereas the endocrine system can yield no, low, medium or high levels of activity. Similarities They both act on receptors. NT and hormones both act on receptors. Mechanism of Hormone Action: Mediated Mediated because you need a second messenger which carries the information from the receptor on the membrane into the cell. 1. receptor action 2. second messenger 3. cell metabolism, gene expression. Polypeptide hormones (cannot pass through cell membrane), monoamines, prostaglandins are examples of hormones that use mediated mechanisms. Sometimes the docking of the hormone on the receptor changes the permeability of the cell. There are a variety of effects of mediated hormone action including protein synthesis. Direct These hormones can enter the cell. They find intracellular receptors, docking onto and forming a HR complex inside the cell and induce gene expression through mRNA. Protein synthesis then occurs at the endoplasmic reticulum. Thyroid (very small) and steroid (4 ring base. Synthesised from cholesterol.) hormones work this way. Mediated is faster than direct. Genomic effect takes a long time (direct). Mediated effect (e.g. changing permeability of the cell membrane) is much quicker. Receptor up and down regulation Too many hormones – down regulation Too little – up regulation No hormone – marked decline of receptors Types of Hormones Amine-derived hormones: derivatives of tyrosine and tryptophan (amino acids) Peptide hormones: chains of amino acids (small: TRH and vasopressin) big chains are known as proteins e.g. insulin and growth hormone. Steroid hormones: derived from cholesterol. The adrenal cortex and the gonads are the primary producers. E.g. T and cortisol. Lipid/phospholipid hormones: derived from lipids e.g. linoleic acid (lipid) and arachidonic acid (phospholipid) The main class is the eicosanoids, which includes the prostaglandins (widely studied). Steroids synthesised from cholesterol. E.g. glucocorticoids (catabolic: provides energy), mineralocorticoids (catabolic), sex steroids (anabolic: uses energy. Associated with building, maintenance and growth functions), estrogens, progestagens. Non-steroid hormone synthesis Synthesised from amino acids in the ribosomes of the rough endoplasmic reticulum of the endocrine cell body. Packaged into vesicles by the Golgi apparatus. Stored in secretory vesicles and released by exocytosis. Preprohormones – prohormones – hormones. Why pre and pro hormones? Prohormones stabilises the 3D structures of peptides during synthesis (acting as a wall). Prohormones are easier to transport and package (like a moving box). Prohormones act as a storage reserve. Prohormones can regulate the amount of hormones released. Prohormones are more resistant to degradation that hormones and they have a longer half life. Synthesis of Steroid Hormones Synthesised from cholesterol in the smooth endoplasmic reticulum of the gonads and adrenal cortex. Cells take up cholesterol from the blood and convert it to pregnenolone in the mitochondria. Pregnenolone is converted into progesterone which acts a s a hormone and can be used as a prohormone for further steroid synthesis. Both the adrenals and the gonads possess all enzymes necessary for steroid synthesis. Both glands can produce all steroid hormones. However, some glands express more of certain enzymes than others, differentiating them from each other. Gonads have more enzymes that use the T pathway. Adrenals have more enzymes that use the cortisol and aldosterone pathway. Hormone actions in the brain Hormones that are released in the brain act in the brain. Hormones released outside the brain can also act in the brain, as revealed by autoradiography. Hormones outside the brain must cross the BBB in order to affect the brain. BBB was discovered 100 years ago. It is semi-permeable. Cells are tightly packed so molecules must be small to cross the BBB and is lipid based so molecules must be liposoluble to cross the BBB (e.g. steroids). Circumventricular Organs Median eminence, pituitary gland and the pineal gland. These organs allow the brain to detect levels of hormone fluctuating in the blood. These are the only areas of the brain where the BBB has an opening. Cell membranes in the brain have the same properties as the BBB January 20th: Lecture 6 Hormone secretion regulated by negative feedback, an important way of maintaining homeostasis. Estrogen receptors in the brain In the hypothalamus, amygdala and the pituitary gland (the limbic system). Regulate sexual behaviours, emotions, parental behaviours, aggression, hunger and temperature. Testosterone and estrogen receptors Males have the enzyme aromatase which converts T into estradial (and then to estrogen). This enzyme is present at the location of estrogen receptors in the brain. It has an interesting effect on the ageing brain. Estrogen has protective functions in the brain (neuro-regeneration). HC volume declines with age. Women have a drastic drop once they reach menopause. Testosterone Receptors Located in the septum, amygdala, HC, HT and PT. They regulate male sexual behaviour, emotion, motivation and spatial ability. Receptors also bind to dihydrotestosterone. Adrenal hormone receptors in the brain Type I: Mineracorticoid. High affinity for steroid hormones, stimulates further hormone release, predominantly in the limbic system and HC. Type II: Glucocorticoid. Low affinity, inhibits further hormone release, distributed throughout the brain. Thyroid hormone receptors Located throughout the brain with highest density in the cerebellum, limbic system and brain stem. Close interaction with adrenergic receptors. In the brain, thyroid hormones perhaps act as neuromodulators within the adrenergic system. Thyroid hormones and brain development cytoarchitecture of the brain can be permanently disrupted by thyroid hormone deficiency. Impairments in cell migration, outgrowths of neurons, synpatogenesis, building of myelin sheaths, proliferation of glia cells. If not treated immediately after birth, permanent mental retardation is inevitable. Some neurological effects (non-permanent) also as adults. Hormones and the HC HC very sensitive to levels of gonads and adrenal steroids. Structural changes, especially within dendrites. Small extensions from the surface, referred to as dendritic spines. Linked with learning and memory, long-term potentiation. Synaptic density and dendritic spines associated with the menstrual cycle: increase during follicular phase. Ablation and replacement Ablation: removal or extirpation of suspected hormone source followed by observation of effects. Replacement: re-implantation of hormone source followed by observation of reversed effects. *End of overview of endocrine system* Berthold's first experiment with Roosters Castration led to caponization. Castration and re-implantation or transplantation led to normal male development. Bioassay The test of the effects of a hormone on the morphology, or part of, a living being. E.g. looking at the size of a roosters comb or the size of a deer's antlers (indications of T levels). Changes in non-endocrine tissue. The vaginal smear technique: measurement of cell types in the vaginal epithelium. Biassay for E and P levels. Early pregnancy test: capacity of human chorionic gonadotropin in urine to induce sperm release in frogs or ovulation in rabbits. Bioassay in humans Large breasts and narrow waists indicate high reproductive potential in women. Behavioural Bioassay How to measure behaviours? Precise qualitative (verbal) or quantitative descriptions (mathematical e.g. number, frequency, amplitude) of behaviour modulated by hormones. Philip deFranco show: would measure hand gestures per minute. Immunoassay Radioimmunoassay: competitive binding assay Based on the principle that a hormone will bind to a specific protein (receptor, antibody, etc). Compare binding rates of ligand bound hormones with regular hormones. Can be used with blood samples and saliva samples. It is dependent on specificity of the antibodies. If the receptor is not specific for a given hormone, it will bind to and detect other hormones from the same category that are not of interest. E.g. 11deoxycortisol might also bind to cortisol receptor. Cross-reactivity with other hormones with a similar structure e.g. cortisol might cross-react with progesterone. January 25th: Lecture 7 Normal and Abnormal Sexual Development We attribute major significance to our sex (labelling, norms, rules). How do hormones cause the sexes to differentiate in terms of their morphology, physiology and psychology. Lawrence H Summers – Harvard President Sex (biological) and gender (societal) are two different terms. Historical Background Aristotle: epigenetic theory of sexual differentiation. Sex emerges during foetal and early life development. Primary and secondary sexual characteristics. Stages of Sexual development Chromosomal sex, gonadal sex, hormonal sex, morphological sex (chromosomal sex directly influences), behavioural sex. Things can go wrong at every stage. Chromosomal Sex XY vs XX. Gonadal Sex: Men have testes, seminal vesicles, prostate gland and tubing. Women have ovaries uterus, oviducts. Hormonal sex: men produce a high androgen to estrogen ratio, women produce the opposite. Morphological Sex: Men are larger and strong usually. Sexual orientation: Males are usually attracted to females and vice versa. Gender roles and identity: people belong to the sex they possess. From Chromosomes to Gonads: no difference during the first six weeks of development (bipotentiality). On the Y chromosome there is an SRY gene (sex determining region of the Y chromosome) which produces the TDF (testes determining factor), a protein which leads to development of the testes from the germinal ridge. You need this gene to change the blueprint of female development. From Gonads to Genitals: TDF stimulates Leydig cells to prevent the formation of the female genital tract from the Mullerian ducts. Happens through Mullerian Inhibitory Hormone (MIH). This hormone is high in males postnatally until puberty. No presence in females until puberty. No SRY, no differentiation, you will be a female. From Genitals to Sexual Development: The testes, once determined, will then start producing sex-specific hormones which will lead the way to specific sexual development. This whole cycle is only present in mammals. In reptiles, SRY is present but not critical, instead temperature is the deciding factor. In birds, males have ZZ chromosomes and females WZ (male is the default setting). Mechanisms of Hormone Action T has masculinising effects through conversion to estradiol via enzyme aromatase. Thus, estradiol has masculinising effects. Estradiol is absent in developing females. Estradiol leads to development of primary male sexual characteristics. Blocking aromatase blocks masculinisation. Exceptions are abundant as always e.g. Hyenas. Human Psychosexual Differentiation Babies at nine months are capable of discriminating between the sexes. Children soon learn to identify their own gender and understand that it's stable. This has an effect on gender roles and identity. Sexual Differentiation at Puberty Period of relative hormonal inactivity during childhood followed by a dramatic surge of HT hormones prior to and during puberty. GnRH → LH, FSH → (men) Leydig cells: T/(Women) E. In addition, adrenal cortex secretes DHEA and Androstenedione as puberty approaches. Puberty occurs at ages six to seven for girls and seven to eight in boys (growth spurt, acne, body odour). Abnormal Sexual Development Complete Androgen Insensitivity Syndrome (CAIS) When the perfect woman is genetically male. This occurs when the receptors for Androgens malfunction. This results in the lack of gene expression that codes for the sexual differentiation. This is due to a mutation in the location of the chromosome that codes for the androgen receptor. This is located on the X chromosome (carried by the mother). This gene is recessive. Sexual differentiation begins at 12-15 weeks after conception. Women with CAIS fail to go down the male pathway and so revert back to the female pathway though they are genetically male. The Prader Scale Used to describe what a baby's genitals look like. Scale is from 0 (woman) to 5 (man). Summary of Differentiation SRY in males not in females. Ovarian vs testicular. Leydig vs Follicle cells T vs E. Muller duct remains or regresses (male). Puberty with CAIS pubertal feminisation still occurs because individuals with CAIS DO respond to E. the testis are a source of androgen, which is converted to E. Therefore normal female secondary sexual characteristics develop. Physical indicators of CAIS in adolescence are: Amenorrhea (menses), no virilisation despite normal to high levels of circulating T. Absence of post-pubertal axillary hair and markedly decreased or absent pubic hair. Women with CAIS tend to be tall. Everything else looks normal. Risks Testicular cancer: due to lack of neg. feedback once puberty occurs and T is produced in high amounts. Depending on time of gonadectomy, hormonal complications can arise. Also, the side effects of E supplementation can cause complications. Osteoporosis (E helps maintain bone density) – this occurs if you do remove the gonads but do not supplement with E. Treatment – 2 options Surgical creation – in which dilation will still be necessary after surgery to prevent scarring and vaginal stricture. Vaginal dilation – can be quite painful and uncomfortable emotionally and physically for young girls. Creating length is the priority, afterwards attempts are made to create width. Counselling is encouraged. Psychologists should have experience in DSD (disorder of sexual development). Groups are there for support (AISSG). Klinefelter Syndrome – XXY An inter sexed individual. Chromosomal sex. It is a trsiomic anomalies. 47 XXY Chromosome. Males have an extra X in their cells. Not every male with XXY has KS. KS causes physical endocrine ,reproductive, cognitive and behavioural disabilities. Between 1/500 – 1/1000 births. 0 females. Other variants of KS – 1/50,000. The cause is not clear. KS is not inherited. Pregnant women over 35 have increased chances of the XXY chromosome. During meiosis, the 46 chromosomes divide into two new cells of 23 chromosomes each. For XXY, there is an error during the formation of the cells which results in an additional X. This is called non-disjunction. This can cause either an XY sperm to fertilise a X egg or a Y sperm to fertilise a XX egg. Physical Symptoms Symptoms variy depending on how many cells are affected, the amount of T and the age when the condition is diagnosed. They do not produce as much T (hypogonadism). Incomplete virilisation. They can live normal sex lives but they make little or no sperm (infertile). Penis does not reach adult size and they have small firm testicles (microorchidism). Enlarge breasts, less facial/body hair, less muscular body, pear shaped (long arms and legs, narrow shoulders and broad hips), taller and weaker bones. Effects on health: Increased risk of autoimmune, breast cancer, cardiovascular, diabetes, lung disease, osteoporosis, tooth decay, vein diseases, etc. Difficulty reading, understanding words, finding words, IQ within normal range though below average. Lower verbal IQ relative to performance IQ related to language deficits. Effects on physical development: as infants KS patients have reduced strength and weak muscles, however after age 4 they tend to be taller though they still have less muscle control and coordination. Gender Identity: Androgynous of feminine feelings that can develop at an early age. Some consider themselves to be transgendered or inter-sexed. Transition to live as a woman though most patients look male. Psychological Disorders from KS: Anxiety, depressions, ADHD, etc. Social Development: KS children need help. Language is used for learning and developing social relationships, therefore intensive language training helps children get by and behave better. Temperament and character of KS patients: shy, passive, un-leader-like and few friends at a time, though well behaved and eager to please. Damaged self esteem due to deficiency in athletics. Treatment Androgen replacement should begin at puberty. Early treatment: promotes normalisation of the body or development of secondary characteristics (facial hair, muscle, wider shoulders), may improve behaviour and work performance and reduces the risk of osteoporosis, autoimmune diseases and breast cancer. XYY Syndrome discovered in 1961 by Dr. Avery A. Sandberg. Incidental Karyotyping. 1/1000 prevalence. Caused by non-disjunction in meiosis II. XYY have increased acne, skeletal disfigurement, thinner build and taller structure. Nothing other really than your average joe. XYY and Aggression XYY males are overrepresented in a maximum security hospital in Scotland, therefore these men might by more aggressive and violent. February 1st: Lecture 8 Gender Roles and Identity Sex refers to biological sex, gender refers to psychological sex. “Sex is between your legs and gender is between your ears.” Gender Identity refers to an individual's basic sense of self as being either male or female. Factors influencing gender identity: biological factors (genes, hormone exposure), environmental factors (society, cultural and parental influences) and the interaation between the two. Congenital Adrenal Hyperplasia (CAH) CAH affects about 1% of the population. It is an autosomal recessive genetic disorder. Most common form of CAH is due to a 21-hydroxylase deficiency (21-OHD). It is a spectrum disorder affecting the adrenal glands (regulated by the pituitary, hypothalamic-pituitary adrenal axis). They mainly produce cortisol but also androgens like T. Adrenal cortex, the outer layer of the adrenal glands, (not the adrenal medulla) is affected by CAH. It produces cortisol (steroid, helps with physical and emotional stress, maintains adequate energy supply and blood sugar levels), aldosterone (steroid, maintains normal levels of sodium and potassium, maintains normal blood volume of the body) and androgens (male steroid hormone). 21-OHD is necessary for the production of cortisol and aldosterone. This enzyme breaks down the precursor hormones into cortisol and aldosterone. If missing, the precursors can only be converted to the adrenal androgens (T). The HPA axis is a negative feedback axis. Stress leads to the HT releasing CRH leading the PT to release ACTH and the adrenal cortex to release cortisol leading to neg. feedback in the HT and PT. In the absence of 21-OHD, you never produce cortisol and no neg. feedback takes place and the system continues to produce CRH and ACTH triggering more cortisol production (which is impossible) so it leads instead to more androgen production and an overabundance of 17-OHP in the adrenal glands. Those with CAH have very little/no production of cortisol/aldosterone and an overproduction of androgens. Hyperplasia: enlarged adrenal glands due to CAH. Example of a use of bioassays. Different forms of CAH Classic and non-classic. Whether you have a deficiency or complete lack of it. 21-OHD or 11-OHD deficiency. Way worse for women than for men. Symptoms Premature pubic hair, advanced bone age, severe acne, childhood body odour, oily hair and skin, depression and anxiety. In women, symptoms usually commence shortly after menses. Thinning of hair on head and infertility. Facial hair that is dark and coarse. Formation of ovarian cysts to do disruption of GnRH release. Menarche (first menses) could be normal or delayed by menstrual irregularities common. Ambiguous genitalia. Enlarged clitoris, joined labia folds. Females born with CAH have XX chromosomes and normal internal genitalia, it is the external genitalia that is different. In men, acne, growth spurts, early beard growth, small tests, low sperm count, short stature. Gender Identity Relevance In childhood/adolescence: Increase in T levels (more male desires e.g. careers), more aggressive, less interested in marriage, motherhood, feminine appearance, lower levels of empathy/intimacy, less heterosexual activity, more homosexuals, CAH>NCAH>control, gender identity is ambiguous, rank themselves somewhere between typical girls and tomboys. Treatment Main goal: provide glucocorticoids to reduce excess CRH and ACTH (restore neg. feedback and reduce production of T). Mineralocorticoids for salt-wasting form or not, e.g. fludrocortisone. Hydrocortisone: infancy, childhood. Dex/prednisone: adolescents, adults (bedtime dose). Guevedoces Genetically born males with enzyme deficiency are raised as girls and establish female gender identity. By the time they reach puberty their bodies become masculinised and they change their gender identity from female to male. They are chromosomal men with a lack of androgens. Lacking DHT in utero leads to female external genitalia. Just before puberty, prior to T outpouring, the phenotype is still female. With the T surge at puberty, the phenotype changes to male, remaining this way for the rest of their lives (scant beard growth, no acne, small testes). There is an interaction of early hormone exposure and parental/environment influences on gender identity. Since the factors are confounded, individual influence is difficult to establish. Mismatch between biological and psychological sex and gender Gender Dysphoria XX or XY chromosomes. The male or female feels strong association with opposite sex. “Male/female trapped in a male/female body.” Belief that they will grow up to be the opposite sex. Desire to be the opposite sex. Disgust with their own genitalia. Withdrawal, isolation, depression. Not due to a physically inter-sex condition. Defects in normal human bonding, genetic abnormality and prenatal hormones all combine to establish gender identity and roles. Treatment As it is thought to be a disorder of the mind, psychotherapy is the normal treatment. Gender identity: continuum or bimodal? It is clearly a continuum. You are not one or the other, there is a spectrum. men – neutral/undefined – women. However due to society, we prefer to have boundaries and we only accept male or female as gender identities. Others are stigmatised. Transgender individuals have previously been protected in most Canadian provinces in the human rights act. Ontario laws now specifically include transgender individuals. From Gender Identity to Gender Role Gender Role: the sum of culturally based behaviour patterns specified to one sex-specific. A set of perceived behavioural norms that indicate one's gender, specifically the image projected by a person that identifies their femaleness or maleness. A gender role is the public expression of one's gender identity. Gender Identity: Identification as a male or female. Sexual Orientation: which gender you are attracted to. Gender roles are realised about the same time as children realise their own gender identity. Gender roles challenged in the 20th Century. Fashion styles and education for women specifically changed dramatically in the 1920's. During the World Wars women had to work while men were fighting, leading to a big change in gender roles.