Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Baker Heart and Diabetes Institute wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
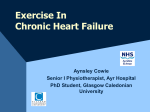
4th Congress of WHFS Drugs in chronic HF: the olds, the news and those coming Journey HF-TR In memory of Prof. Dr. Henry Krum Page 1-3 Page 3,4 Page 5,6 Page 6,7 Newsletter Volume 1, Issue 1, January 2017 World Heart Failure Society Board Members Albertino Damasceno Babak Sharif-Kashani Bambang Budi Siswanto Byung-Hee OH Cheuk Man Yu Dong Zhao Elsadig Kazzam Felipe Martinez Gilson Feitosa Inder Singh Anand Kewal Krishan Talwar Masatsugu Hori Mehdi Zoghi Siddiq Ibrahim Khalil Siddiq Reddy Simon Stewart Thikayat A Noorudin Willem J. Remme Yura Mareev The World Heart Failure Society’s Newsletter is published online every 3 months. Each issue features news and updates on diagnosis and management of heart failure, multicenter clinical study and/or questionnaires initiatives on field of heart failure for all health professionals. You can also find a column for announcement of your studies, congresses and case presentations. 4th Congress of WHFS Welcome to the first issue of WHFS-Newsletter! In this issue, we have focused on 4th WHFS Congress. Prof. Dr. Cheuk Man Yu gave some information about the congress. Prof. Dr. WJ. Remme, the founder of World Heart Failure Society, also wrote in memory of Prof. Henrry Krum, one of the active members of WHFS, who passed away 2 years ago. The results of JourneyHF-TR are presented by Dr. Ümit Yaşar in “Your Column” section. Prof. Dr. Cheuk Man Yu As the Immediate Past President of the World Heart Failure Society (WHFS), I am proud and delighted to conclude that the Fifth World Heart Failure Congress (WHFC 2016) was successfully held on 14-16 October 2016 at Beijing, China. In the WHFC 2016, we are particularly honoured that the congress was conjoint with 27th Great Wall International Congress of Cardiology (GW-ICC 2016). The WHFC 2016 had provided a unique platform that has united physicians, allied health and research professionals from around the world who are involved in the field of heart failure. The 3-day congress had covered all facets of heart failure. These included clinical trials in pharmacotherapy, device therapy, surgical management, interventional and novel therapeutics, heart failure rehabilitation, risk factors and prevention, acute decompensated heart failure, heart failure with preserved ejection fraction, imaging for heart failure, basic research, biomarkers, and more. Our speakers comprised a balanced mix between renowned international faculties and board members of WHS, as well as eminent cardiologists from China and Asia. As management of heart failure is gaining widespread recognition by cardiologists in China, the meeting hall for WHFC 2016 was full of enthusiastic audiences. In WHFC 2016, there was detailed presentation and extensive discussion on how heart failure treatment guidelines can be applied to developing countries, innovative heart failure implantable technologies such as cardiac contractility modulation, PARACHUTE devices, stem cell therapy, drugs under development, and multidisciplinary approach for heart failure management. Board members of WHFS will summarize some of these key topics in the upcoming Newsletters and thanks to their great efforts. During the Opening Ceremony, I have pointed out that heart failure has become a world-wide endemic including the developing countries. Therefore, the WHFS has been dedicating its effort in helping cardiologists in these regions to develop their heart failure management programs and training of heart failure physicians. I would like to thank the GW-ICC again for collaborating the organization of our WHFC 2016 in China. In particular, I have to express my gratitude to the Board Members of WHFS for their dedicated effort in supporting the Congress. I am glad that I could meet some of the members of the WHFS in person during my stay in Beijing, and again thank you for your participation to the Congress. In Year 2017, may I wish all members of WHFS a happy, healthy and successful year to come. Drugs in chronic HF: the olds, the news and those coming Prof. Dr. Felipe Martinez Most of international registries proved that approximately 1–2% of the adult population has heart failure (HF) in developed countries, with the prevalence rising to ≥10% among persons 70 years of age or older. These numbers are even higher in regions with low socioeconomic conditions. There are many causes of HF, and these vary in different parts of the world. Coronary artery disease (CAD) is the cause of approximately two-thirds of cases of systolic HF. Hypertension and diabetes are probable contributing factors in many cases. The above scenarios justify the large amount in research with the goal of discovering new drugs. The main goals are prevention, relief of symptoms and signs and improve survival. During the last 30 years many drugs have proved clear benefits in reducing outcomes and mortality and they are in use in most Countries around the world. This article reviews the pharmacologic treatment of chronic HF with reduced EF only and focusing in new drugs and some key compounds that appear in the horizons and are supporting the idea that HF is now becoming a preventable and treatable disease (Figure 1). Figure 1: List of main group of drugs with proved benefits in the reduction of outcomes and mortality in heart failure (HF) patients. ACEI= angiotensine converting enzyme inhibitors. BB= beta blockers. MRA= mineralocirticoid receotor antagonists. ARB= angiotensin receptor blockers. NEW DRUGS IN RECENT GUIDELINES In the past couple of years the evidence of new compounds and/or new mechanisms stimulates the need of Guidelines. Probably the 2016 version of the European Society of Cardiology is which reflects the most updated approach in this field. 1) Mineralocorticoid Receptor Anatgonists (MRA): Almost 50 years after its approval, spironolactone had a revival of great impact with the results of RALES. 3 The initially so called “aldo blockers” group includes eplerenone and most recently finerenone. And these drugs are now recommended as first line indications in some types of HF, mainly chronic and post myocardial infarction. What are the reasons of this consolidated recommendation in most of the recent international guidelines? There are two main causes: a)The growing role of the mineralocorticoid receptor in the pathophysiology of cardiometabolic disorders, and in particular HF. b) The increased selectively in the pharmacologic antagonism of new compounds of the group. In summary, the MRA group of drugs has reached enough evidence to be prescribed in all NYHA class of chronic HF with reduced EF and post MI. 2) SRAA dual inhibition: This interventional strategy has been explored since many years ago and with different pathways. There were several failures, the most important was omapatrilat that inhibited the ACE and neprilysin simultaneously, but the adverse events observed in Phase III were enough to take the drug off. In 2014 the PARADIGM Trial was published and changed the history (Figure 3). This study compared LCZ696, a compound with a dual inhibition of the ATII receptor (valsartan) and a neprilysin inhibitor (sacubitril) versus enalapril on top of usual treatment for patients with chronic HF. The trial was stopped before the end due to the great difference in lowering mortality in the group receiving the study drug. The surprising results were consistently repeated in all subgroups and in all regions were the study was performed. 3)Glifozines or Sodium GLucose Transporter 2 inhibitors (SGLT2 I): This group of drugs was approved by most of the Regulatory Agencies for the treatment of Type II diabetes. Surprisingly in one of the largest Phase III studies, the EMPA-REG Trial, a significant lower incidence of heart failure was observed in the group of patients receiving empaglifozine, one of the five drugs approved in this group. Figure 3: The PARADIGM Trial. Primary Endpoint Despite of the evidence that these new compounds have a diuretic effect, many other beneficial effects on the cardiovascular system have been described, and still need more research. But after the provocative results published in EMPA-REG, the pharmacy industry has launched important programs to confirm if these drugs have very positive mechanisms to prevent and treat HF and also renal dysfunction in diabetics and nondiabetics patients. If the potential benefits are confirmed the new group will become a very useful tool for the management of HF. 4)What is in the pipe line? There is a long list of drugs under research for the treatment of HF. Many of them are also in studies including hypertensive patients, as it has happened in the past. Since the role of the RAAS in the pathogenesis of both diseases is very inportant, it is not a suprise that many of the investigatid compounds are direct or indirect intervention in that system. CONCLUSIONS: 1) “Old drugs” still in use have demonstrated clear benefits lowering morbidity and mortality in HF. 2) New compounds show solid evidence in improving the above , mainly in chronic HF. Among others, the most outstanding are: MRA and ARNI. 3) There are ongoing optimistic studies with more new drugs that could even increase the benefits in patients with HF. 4 Patient Journey in Hospital with Heart Failure in Turkish Population: on behalf of Journey HF-TR study investigators Dr. Ümit Yaşar Sinan Heart failure (HF) is one of the most important causes of morbidity and mortality in the world. The prevalence is 0.4 to 2% in general European population and 5 million Americans with chronic HF are mostly attributable to inpatient hospitalization. Acute exacerbation of chronic HF is a lifethreatening clinical syndrome characterized by rapid onset of HF symptoms and signs and requires urgent therapy. Patients with acute HF (AHF) have poor short and long-term prognosis. In-hospital mortality rate is high in AHF patients due to medical therapy and remains high after discharge. The surveys and registries provide valuable information regarding epidemiology, outcomes of realworld and better understanding of medical practice in this clinical condition. In this study, we aimed to evaluate the overall clinical characteristics, management and inhospital outcomes (from ICU admission to discharge) of hospitalized patients with AHF in Turkish population. The Journey HF-TR study is a cross-sectional, multicenter, non-invasive and observational trial that was conducted in ntensive/coronary care units and cardiology wards. We enrolled a total number of 1,606 patients in 39 centers, in seven geographical regions of Turkey. The patients who were hospitalized with the diagnosis of acute heart failure in intensive/coronary care units between September 2015 and 2016 were included in our study. 1606 patients (male: 57.2%, mean age was 67.8±13 years old) who were diagnosed with AHF in 37 centers, in seven geographical regions of Turkey were enrolled in this study. Hypertension (67%), coronary artery disease (59.6%) and diabetes (41.9%) were the most frequent underlying diseases. Anemia (using WHO definition: Hb <13.0 g/dl for males and Hb <12.0 g/dl for females) was detected in 48.1% of the patients. Chronic kidney disease (CKD) (defined as glomerular filtration rate-GFR- <60 ml/min/1.73m2) was detected in 28.2% of the patients. Most frequent arrhythmia was atrial fibrillation (39%). Seventeen percent of patients were admitted to hospital with diagnosis of new onset AHF (de novo AHF) and 83% of patients were admitted with diagnosis of ADCHF. The 75.2% patients were in NYHA class III-IV. Biomarkers were used in 41% of patients at admission for diagnosis. Echocardiography was available in 92% of the patients and was performed averagely in three days after admission. Most of the patients (64%) had EF lower than 40% (defined as heart failure with reduced EF-HFrEF). The rest of the patients were consisted of heart failure with mid-range EF (HFmrEF) (19%) and HF with preserved EF (HFpEF) (17%). The prescription of guideline recommended medications were often more at discharge: Diuretics (from 71% to 81%), ACE inhibitors or ARBs (from 62% to 81%), betablocker (from 73% to 87%) and MRAs (from 39% to 60%). The median length of stay (LOS) in ICU was 3 days (IQR 1-72), in general or cardiology ward was median 4 days (IQR 1-62). In-hospital mortality rate was 7.6%. 5 The Journey HF-TR database is providing valuable and up-to-date information on demographics, characteristics, and underlying condition of AHF patients as well as etiology, investigation and treatment practices of AHF in Turkey. Analyses of data provide to observe compliance with the current ESC guidelines proposal on management of AHF and will help preparing a national database and distinctive diagnosis and treatment algorithms. The one-year follow-up data will be collected and these data will provide further improve for HF care in Turkey. In memoriam Prof. Henry Krum, 1958–2015 By Prof. Dr. Willem J. Remme Prof. Henry Krum, 1958–2015 Whereas basic cardiovascular pharmacology in which he started, always remained an important element , Henry Krum had the opportunity to follow a post-doctoral fellowship at Columbia Presbyterian Medical Centre in New York headed by Professor Milton Packer, a leading expert in large-scale clinical trials in heart failure. This episode laid the basis of his later career as one of the world’s most important pioneer in the conduct of controllled clinical studies in heart failure, hypertension, and diabetes and renal dysfuncion in relation to heart failure. At the occasion of the publication of this first Newsletter of the World Heart Failure Society we wish to commemorate Professor Henry Krum, one of the founding members of the Society, who died on November 28, 2015, at the age of 57 from pancreatic neuroendocrine cancer. Henry Krum was born in Melbourne, Australia. He started his medical studies at the Melbourne University in 1976, and subsequently trained and obtained a PhD as clinical pharmacologist. Back in Melbourne, Henry Krum founded the Monash Centre of Cardiovascular Research and Education in Therapeutics, an Institute that under his leadership became wellknown in the international scientific arena, and from which he supervised an endless production of scientific publications in highranking journals, and tutored many young trainees in both basic and clinical pharmacology of heart failure. 6 During his life Henry Krum has been involved in many crucial heart failure studies as a member or Chairman of Steering Committees and in this position has played a fundamental role in our recognition of beneficial effects of beta-blockers , renin-angiotensin inhibitors and aldosterone antagonists in heart failure, the cornerstones of current medical therapy. Moreover, Henry Krum had an interest in hypertension and published on the effectiveness of renal denervation on blood pressure reduction in patients with resistant hypertension. His more recent focus was on the role of co-morbidities in heart failure, including diabetes and chronic kidney disease, and the potential role of neurohormonal inhibition in these areas. Henry Krum was an excellent scientist. He was also a very amiable person with great interest in his companions and friends. Plagued by back trouble he would often stand for periods on end during our meetings, but would never complain, instead remained joyful and attentive. He saw this as his personal problem, not one that should be a concern of others. Henry Krum was also greatly interested in new developments. When approached at a very early stage in our setting up of the World Heart Failure Society, he immediately and enthusiastically accepted to become a member of the newly founded Steering Committee and became very much involved in the creation of the Society. His suggestions how to proceed and his direct input in this, have been very valuable for us in our efforts to develop the Society into what it currently has become. He was truly an asset for the World Heart Failure Society and will be very much missed by us. Prof. Mehdi Zoghi, MD, FESC Ege University, cardiology Dpt. İzmir-Turkey [email protected] http://www.worldheartfailure.org