Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pyotr Gannushkin wikipedia , lookup
Psychological evaluation wikipedia , lookup
Major depressive disorder wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Asperger syndrome wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Sleep paralysis wikipedia , lookup
Effects of genocide on youth wikipedia , lookup
Conversion disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Child psychopathology wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
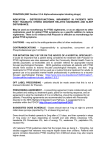
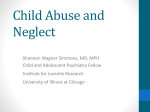
Characteristics of Chronic Nightmares in a Trauma-Exposed Treatment-Seeking Sample Joanne L. Davis, Patricia Byrd, and Jamie L. Rhudy University of Tulsa David C. Wright United States Air Force Chronic nightmares pose a significant problem for many individuals affected by trauma. The present study attempts to extend current knowledge on the nature, characteristics, and associated sequelae of chronic nightmares. Data were collected from 94 trauma-exposed, treatment-seeking participants (74 women and 20 men). These data suggest that most participants reported their nightmares to be similar or dissimilar to their traumatic experience rather than exact replications (replicative). Not surprisingly, though, nightmarerelated distress was positively related to the degree of similarity between their nightmare and their trauma, with replicative nightmares eliciting the greatest distress. Persons with a current diagnosis of posttraumatic stress disorder (PTSD) were more likely to report problems related to nightmares and sleep disturbance than persons without current PTSD. Nonetheless, even after controlling for PTSD-related symptomatology, frequency and severity of nightmares significantly predicted some distress outcomes (e.g., poor sleep quality), suggesting that nightmares contribute to psychological distress above and beyond PTSD symptoms. Implications for future research, and for the treatment of nightmares and PTSD, are discussed. Keywords: nightmares, posttraumatic stress disorder, trauma Nightmares are a pernicious and common complaint reported by individuals affected by trauma. Research has found that chronic posttraumatic nightmares are related to the presence and severity of posttraumatic symptoms (David & Mellman, 1997; Mellman, David, Bustamante, Torres, & Fins, 2001; Schreuder, Kleijn, & Joanne L. Davis, Patricia Byrd, and Jamie L. Rhudy, Department of Psychology, University of Tulsa; David C. Wright, United States Air Force. The activities described were supported by an OHRS award for project number HR02-002S from the Oklahoma Center for the Advancement of Science and Technology, by the Psi Chi National Honor Society, and by the University of Tulsa’s Office of Research and Sponsored Programs internal funding. Portions of this article were presented at the annual meetings of the following organizations: the Association for the Advancement of Behavior Therapy, the Oklahoma Psychological Association, and the Disaster Mental Health Institute. We wish to express our appreciation to the members of the Trauma Research: Assessment, Prevention, and Treatment Center for their assistance with this project. Correspondence concerning this article should be addressed to Joanne L. Davis, 600 South College Avenue, University of Tulsa, Tulsa, OK 74104. E-mail: [email protected] 187 Dreaming 2007, Vol. 17, No. 4, 187–198 Copyright 2007 by the American Psychological Association 1053-0797/07/$12.00 DOI: 10.1037/1053-0797.17.4.187 188 Davis, Byrd, Rhudy, and Wright Rooijmans, 2000; van der Kolk, Blitz, Burr, Sherry, & Hartmann, 1984), and nightmares may differ in persons with and without posttraumatic stress disorder (PTSD; e.g., Mellman, Kulick-Bell, Ashlock, & Nolan, 1995). The majority of studies examining characteristics of chronic nightmares have used combat populations; thus, much less is known about chronic nightmares in those exposed to civilian trauma. The purpose of this article is to explore the nature and characteristics of chronic nightmares in a clinical sample of diverse trauma-exposed persons with and without PTSD. The majority of studies on nightmares in trauma-exposed samples have focused on their prevalence, content, and association with PTSD. “Trauma nightmares” or “PTSD nightmares” are generally thought of as being exact replays (i.e., replicative) of a traumatic event. Indeed, Ross, Ball, Sullivan, and Caroff (1989) suggested that replicative nightmares were specific to PTSD. However, most of the research has failed to make a distinction between nightmares that are exact replays of the trauma and those that are only similar to the trauma. This has made it difficult to determine the prevalence of nightmares based on their similarity to the traumatic event (i.e., replicative, trauma similar, trauma dissimilar) and whether the degree of similarity affects distress. Furthermore, it remains unclear whether such trauma-similarity distinctions are clinically or empirically important. Several studies have found that replicative or trauma-similar nightmares are associated with severity of PTSD symptoms (Mellman et al., 2001, 1995; Schreuder et al., 2000; van der Kolk et al., 1984). Esposito, Benitez, Barza, and Mellman (1999) analyzed dream content in 18 combat veterans with PTSD and found that approximately half of the sample experienced dreams with content similar to combat. A relationship was also found between trauma-similar dreams and severity of reexperiencing symptoms of PTSD. Mellman et al. (1995) sampled 58 combat veterans, 37 of whom met criteria for PTSD, and found that veterans with PTSD were more likely to report having nightmares with combat content than those without PTSD. Similarly, van der Kolk et al. (1984) assessed 15 combat veterans with PTSD and 10 noncombat veterans without PTSD but who reported lifelong nightmares. Eleven veterans with PTSD and none without PTSD reported having nightmares that replicated a traumatic event. Moreover, all 15 of the veterans with PTSD reported having repetitive nightmares compared with 3 individuals without PTSD. So although the veterans without PTSD reported a lifelong problem with nightmares, their nightmares did not replicate an actual event and generally did not repeat over time. Limited research has examined the association of nightmares and PTSD among survivors of civilian trauma. David and Mellman (1997) researched 32 victims of Hurricane Andrew (20 of whom met criteria for PTSD) 6 to 12 months after the disaster who recalled a dream within the past month. Although significant differences were not found between those who met criteria for PTSD and those who did not, replicative nightmares (referred to as dreams by the authors) were only reported by those who met criteria for PTSD. Similarly, Mellman et al. (2001) assessed dreams and PTSD in 39 patients admitted to a hospital following a life-threatening event (e.g., motor vehicle accident, industrial accident, and interpersonal assault) and again 6 weeks later. Dreams were considered “trauma dreams” if raters indicated they were moderately to exactly similar to the traumatic event and moderately to extremely disturbing. From the 21 dreams reported, 10 were categorized as trauma dreams. The remaining dreams were either distressing Characteristics of Chronic Nightmares 189 but dissimilar to the trauma or not distressing and dissimilar to the trauma. Results indicated that more severe PTSD symptoms were reported by those experiencing dreams highly similar to their traumatic experience at admission and follow-up. Schreuder et al. (2000) conducted a larger study involving 167 civilian victims and 56 combat veterans of World War II. Of those, 124 participants met full criteria for PTSD and 102 reported posttraumatic nightmares. Posttraumatic nightmares were categorized as “mostly or completely replicative” (42%; nightmares that were very similar to the event), “mostly or completely nonreplicative” (28%; nightmares that were an unrealistic account of the event), and “mixed replicative and nonreplicative” (35%; nightmares that were somewhat similar to the event) of the traumatic experience. Individuals reporting “mostly or completely replicative” nightmares also experienced more frequent nightmares, more repetitive nightmares, and more symptoms of intrusion; however, they reported fewer psychological symptoms as measured by the Symptom Checklist–90 (Derogatis, 1975; Derogatis et al., 1973). The researchers suggested this may be due to the type of trauma experienced because combat veterans made up a larger portion of the replicative posttraumatic nightmare group and had lower overall Symptom Checklist–90 scores than those in the other trauma groups. This finding raises interesting questions about the relationship between the content of nightmares and psychological symptomatology other than PTSD. Chronic nightmares, regardless of content, pose a significant problem for those suffering from PTSD, but their effects may not be limited to individuals with PTSD (e.g., Mellman et al., 1995). Recent evidence has suggested that chronic nightmares may have negative consequences for trauma-exposed individuals without PTSD. In the Schreuder et al. (2000) study, those with PTSD and nightmares, regardless of content, reported more psychological symptoms. Persons with posttraumatic nightmares were also found to have worsened psychological and physical functioning and increased sleep problems relative to those without such nightmares. Thus, it appears that posttraumatic nightmares may be highly disruptive and affect multiple areas of functioning, regardless of the presence of PTSD. The present study extends current knowledge on chronic nightmare characteristics in a civilian sample by categorizing nightmares as replicative of, similar to, or dissimilar to participant trauma experiences. Several hypotheses were formulated on the basis of past research. First, the prevalence of replicative nightmares was expected to be lower than nightmares similar or dissimilar to trauma experiences. Second, replicative nightmares were expected to be associated with greater distress (increased PTSD and depression symptoms, poorer sleep quality and quantity, and greater frequency and severity of nightmares). Last, PTSD-positive individuals were expected to report more frequent and severe nightmares and more replicative nightmares than PTSD-negative individuals. METHOD Procedure The present study is part of two larger studies evaluating the efficacy of a cognitive– behavioral treatment for chronic nightmares in trauma-exposed persons. 190 Davis, Byrd, Rhudy, and Wright Only baseline data from the two studies were used in this article. Participants were recruited via flyers, e-mail, and radio ads from August 2002 through July 2006. The ads stated that we were recruiting for a treatment study for recurring nightmares, that treatment was free, and that participants would be compensated for the evaluations. Potential participants were screened over the phone for trauma history, exclusion criteria, and frequency and duration of nightmares. Inclusion criteria consisted of experiencing a traumatic event and having had nightmares at least once per week for the previous 3 months. Exclusion criteria consisted of apparent psychosis or mental retardation, age younger than 18, active suicidality or recent parasuicidal behaviors, or current drug or alcohol dependence. There were no restrictions on race or ethnic background. All participants who met inclusion criteria were invited to participate in the study. Upper-level trained graduate students conducted the assessments. Participants were provided a $20.00 gift certificate to a local department store to compensate them for their time. Participants A total of 94 people participated in the baseline evaluations, of which 49 (52%) were in the first study and 45 (48%) were in the second study. Of the participants, 79% were women, 80% were Caucasian, and the mean age was 39.9 (SD ⫽ 11.99). Thirty-seven percent of the sample were married, and 23% were divorced, and 71% had at least some college education. The mean income of the sample was approximately $40,000 (SD ⫽ $54,043). Participants reported a mean of 4.6 different traumatic events (SD ⫽ 2.02, range ⫽ 1–9). The most frequent types of trauma reported were unwanted sexual contact (59.6%), car accident (58.5%), physical assault with a weapon (54.3%), and physical assault without a weapon (51.1%). Although having a PTSD diagnosis was not a requirement of the study, a total of 55% (n ⫽ 52) of the participants met criteria for current PTSD and 64% met criteria for lifetime PTSD. Measures Demographic Questionnaire The demographic questionnaire is a self-report measure designed to obtain standard background information about the participants, including age, native language, marital status, educational achievement, ethnicity, vocational status, and household income. Modified Trauma Assessment for Adults: Self-Report Version (TAA; Resnick, Best, Kilpatrick, Freedy, & Falsetti, 1993) The TAA assesses for lifetime history of 13 types of traumatic events, including serious accidents, sexual assault, interpersonal traumas, natural disasters, witnessing a violent crime, being diagnosed with a serious illness, having a friend or family Characteristics of Chronic Nightmares 191 member deliberately killed, and other situations that involve fear of being killed or seriously injured or in which injury took place. The TAA was modified to include an additional five items assessing for hate crimes. Follow-up questions include age of first and most recent occurrence for multiple incidents of a given type, physical injury, and perceived life threat. The TAA’s validity is supported by consistent findings with a different assessment measure of traumatic events. Furthermore, comparison of TAA results with archival data from records in a mental health clinic revealed that the TAA captured all reported and some unreported traumatic events (Resnick, 1996). Structured Clinical Interview for DSM–IV: PTSD Module (SCID; Spitzer, Williams, & Gibbon, 1995) The SCID is a formulized diagnostic interview developed to assess and closely follow the criteria in the Diagnostic and Statistical Manual of Mental Disorders (4th ed., or DSM–IV; American Psychiatric Association, 1994). The PTSD module assesses current and lifetime diagnoses of PTSD. Researchers have found the SCID to be a valid and reliable instrument in following diagnostic criteria set forth by the DSM (e.g., Davidson, Smith, & Kudler, 1989). All participants in Study 1 were administered the PTSD module of the SCID to determine current and lifetime PTSD diagnosis. Clinician-Administered PTSD Scale (CAPS; Blake et al., 1995) The CAPS is a semistructured interview that assesses lifetime and current PTSD. It consists of 17 questions assessing the frequency and intensity of core PTSD symptomatology. All participants in Study 2 were administered the CAPS to determine current and lifetime PTSD diagnosis. Two methods for scoring criteria were used as outlined by Weathers, Ruscio, and Keane (1999), which included the symptom endorsement necessary to meet criteria according to the DSM–IV and the summing of the frequency and intensity scores for each symptom while using the cut-off score of 65. The symptom endorsement method has been shown to have a 91% sensitivity rate and a 71% specificity rate, and the cut-off score of 65 has been shown to have 82% sensitivity rate and a 91% specificity rate (Weathers et al., 1999). Blake et al. (1990) reported interrater reliability ranging from .92 and .99 and perfect diagnostic reliability using a sample of combat veterans. Weathers et al. conducted a test– retest reliability investigation with 60 combat veterans and found interclass correlations of .93 for frequency scores and .95 for intensity scores. Furthermore, with a sample of 243 veterans they also found internal consistency estimates using alpha of .93 for frequency and .94 for intensity with all 17 items. Beck Depression Inventory—II (BDI–II; Beck, Steer, & Brown, 1996) The BDI–II is a 21-item self-report inventory to assess symptoms of depression. For each item, respondents assess symptom severity from four choices. Items 192 Davis, Byrd, Rhudy, and Wright are added to yield a total score. This scale is a modified version of the BDI that has been used in numerous research projects on depression (e.g., Beck, Steer, & Garbin, 1988) and has also been used to assess depression in victims of crime (Falsetti, Resnick, & Davis, 2005). The BDI–II has a reliability of .92. Pittsburgh Sleep Quality Index (PSQI; Buysse, Reynolds, Monk, Berman, & Kupfer, 1989) The PSQI is a self-report measure designed to assess certain qualities and problems associated with sleep. Participants rate quality of sleep and degree of sleep difficulties for 1 month before the assessment. A global sleep quality score is obtained by summing the seven component scores, including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Higher scores reflect poorer sleep quality. The global score may range from 0 to 21. The PSQI has acceptable internal consistency, test–retest reliability, and validity (Buysse et al., 1989). Buysse and colleagues determined a cut-off score of 5 as distinguishing “good” sleepers from “poor” sleepers, with a diagnostic sensitivity of 89.6% and a specificity of 86.5%. Trauma Related Nightmare Survey (TRNS; Davis, Wright, & Borntrager, 2001) The TRNS was developed to assess characteristics of chronic nightmares. Likert-type, categorical, and open-ended questions assess the frequency, severity, and duration of nightmares, as well as cognitions, emotions, and behaviors related to nightmares. Participants were asked to indicate whether their nightmares were “exactly or almost exactly like the trauma,” “similar to the trauma,” or “unrelated to the trauma.” We allowed the participants to self-define their nightmares and asked them to explain what they meant if they indicated that their nightmares were trauma similar or trauma dissimilar. Examining their responses, trauma-similar nightmares included aspects of the actual trauma, but the place, people, or specific acts were different. Trauma-dissimilar nightmares included threatening or scary situations but did not include any clear aspect of the traumatic event. Test–retest analyses revealed adequate reliabilities for past-week hours of sleep per night (r ⫽ .72), fear of going to sleep (r ⫽ .77), depression upon waking (r ⫽ .72), feeling rested upon waking (r ⫽ .65), frequency of nightmares (r ⫽ .64), and severity of nightmares (r ⫽ .63; Byrd et al., 2006). Convergent validity was also found with daily behavioral records of sleep and nightmares (Daily Sleep Activity Log; Thompson, Hamilton, & West, 1995): nights with nightmares (rs ⫽ .74 –.82); number of nightmares (rs ⫽ .76 –.81); and the Modified PTSD Symptom Scale (MPSS) nightmare frequency (r ⫽ .64) and severity (r ⫽ .45; Byrd et al., 2006). MPSS Self-Report (MPSS-SR; Resick, Falsetti, Resnick, & Kilpatrick, 1991) The MPSS-SR is a modification of the PTSD Symptom Scale developed by Foa, Riggs, Dancu, and Rothbaum (1993). Changes were made to assess for both frequency and severity of PTSD symptoms. The scale consists of 17 items that Characteristics of Chronic Nightmares 193 correspond to PTSD symptom criteria in the text revision of the DSM–IV (American Psychiatric Association, 2000). Frequency of PTSD symptoms is assessed on a 4-point scale ranging from 0 (not at all) to 3 (5 or more times per week/very much/almost always). Severity of PTSD is assessed on a 5-point scale ranging from 0 (not at all distressing) to 4 (extremely distressing). The convergent validity of the MPSS-SR with a structured clinical interview for PTSD (Spitzer et al., 1995) revealed excellent results, with an overall hit rate of 97% when using the cut-offs for the frequency scale (Wright, David, Inness, & Stem, 2003). The internal consistency of the full scale MPSS-SR has been reported at levels of .96 and .97 in treatment and community samples, respectively (Falsetti, Resick, Resnick, & Kilpatrick, 1992, as cited in Falsetti, Resnick, Resick, & Kilpatrick, 1993). The overall frequency and severity subscales were used for the analyses. Symptoms were also examined at the criterion level. For these analyses, the nightmare question was removed from the reexperiencing category and the sleep difficulties question was removed from the arousal category. RESULTS Participants reported a mean nightmare frequency of 4.01 nightmares per week (SD ⫽ 3.78), 3.24 nights per week with nightmares (SD ⫽ 1.96), and 1.81 nights per week with more than one nightmare (SD ⫽ 2.09). Average nightmare severity, rated on a scale ranging from 0 (not at all disturbing) to 4 (extremely disturbing) was 3.0 (SD ⫽ 0.78). Participants reported a mean of 5.65 (SD ⫽ 1.77) hour of sleep per night, and 37% of the sample reported sleep initiation taking 1 or more hours each night, on average. The hypothesis that replicative nightmares would be less prevalent than trauma-similar or trauma-dissimilar nightmares was supported. Fifty percent reported nightmares that were trauma similar, 29.5% reported nightmares that were trauma dissimilar, and 20.5% reported nightmares that were replicative. One-way analyses of variance were conducted on several measures of distress, with nightmare content (replicative, trauma similar, trauma dissimilar) entered as the independent variable (see Table 1). In support of the second hypothesis, individuals with replicative nightmares reported fewer hours of sleep per night, greater fear of going to sleep, greater depression upon waking, and poorer sleep quality than those with traumadissimilar nightmares. Individuals with replicative nightmares differed from those with trauma-similar or trauma-dissimilar nightmares in terms of greater depression, greater overall PTSD symptom frequency and severity, greater frequency and severity of PTSD reexperiencing, and avoidance and arousal symptoms. Relative to trauma-dissimilar nightmares, replicative and trauma-similar nightmares were associated with greater frequency of nightmares per week and more nights with nightmares per week. Finally, people who reported trauma-similar nightmares reported greater overall PTSD symptom frequency and severity and greater frequency and severity of reexperiencing and avoidance symptoms than those with dissimilar nightmares. Analyses of variance were conducted to compare characteristics of nightmares and sleep problems by PTSD status (see Table 2). As hypothesized, results indicated that PTSD-positive individuals reported greater frequency and severity of 194 Davis, Byrd, Rhudy, and Wright Table 1. Type of Nightmare and Related Distress Replicative Trauma similar Trauma dissimilar Dependent variable M SD M SD M SD F df No. hours slept per night Fear of going to sleep Depression upon waking Feeling rested upon waking Nightmares per week Nights with nightmares per week Nights with more than one nightmare per past week Disturbance of the nightmares Global depression (BDI-II) Overall sleep quality Panic symptoms upon waking from nightmare Frequency of PTSD symptoms Severity of PTSD symptoms PTSD reexperiencing symptoms PTSD avoidance symptoms PTSD arousal symptoms 4.86a 2.00 2.39a 0.78 4.58 4.06a 1.63 1.14 0.92 0.88 2.54 2.60 5.73 1.43 1.75 1.23 4.59 3.51a 1.56 1.15 1.08 0.81 4.86 1.95 6.21b 1.23 1.38b 1.35 2.48 2.35b 1.97 1.11 1.10 0.94 1.10 1.02 3.35* 2.55 4.84* 2.51 2.78 5.02** 2, 85 2, 85 2, 85 2, 84 2, 83 2, 85 2.56a 3.33 31.67a 15.35a 2.28 0.69 11.33 3.86 2.06a 2.93 19.18b 13.38 2.24 0.82 10.32 4.23 0.76b 2.92 17.73b 11.08b 1.01 0.80 12.56 4.04 5.14** 1.89 9.77*** 5.61** 2, 83 2, 85 2, 85 2, 81 5.89 40.59a 52.82a 22.82a 36.65a 21.59a 2.93 5.64 9.40 3.43 8.78 5.32 5.30 27.57b 32.25b 13.84b 23.50b 14.05b 2.98 11.97 16.35 7.69 11.55 7.67 4.00 16.35c 20.15c 8.12c 13.46c 10.08b 2.70 9.06 13.40 6.16 10.96 7.29 2.49 29.38*** 26.53*** 25.40*** 23.33*** 13.35*** 2, 83 2, 84 2, 84 2, 84 2, 84 2, 84 Note. Specific type of sleep problems were rated on a Likert scale ranging from 0 (not at all) to 4 (extremely). Subscript letters indicate significant differences. BDI-II ⫽ Beck Depression Inventory—II; PTSD ⫽ posttraumatic stress disorder. * p ⬍ .05. ** p ⬍ .01. *** p ⬍ .001. nightmares, poorer sleep quality and quantity, greater panic symptoms upon waking from nightmares, and greater global depression. The groups did not differ, however, on reported severity of the nightmares. PTSD-positive individuals were also more likely to report experiencing replicative nightmares and less likely to report experiencing trauma-dissimilar nightmares than PTSD-negative individuals. A series of regressions was conducted to determine whether nightmare severity or frequency contributed to any sleep problems or related distress when controlling for non–sleep-related PTSD symptoms. Results indicated that nightmare frequency was a unique predictor of poor global sleep quality (B ⫽ 0.57, SE ⫽ 0.22), t(86) ⫽ 2.58, p ⬍ .01, and fear of going to sleep (B ⫽ 0.13, SE ⫽ 0.06), t(90) ⫽ 2.34, p ⬍ .02, whereas a trend existed regarding the role of the severity of the nightmare in predicting panic symptoms on waking from a nightmare (B ⫽ 0.72, SE ⫽ 0.38), t(88) ⫽ 1.89, p ⫽ .06. DISCUSSION The results of the present study indicate that approximately half of our civilian sample reported experiencing nightmares that were similar in content to their traumatic event, and 21% reported replicative nightmares. Previous studies have found rates ranging from 40% (Schreuder et al., 2000) to 73% (van der Kolk et al., 1984). It is difficult to compare the current findings with these studies because of the different ways in which researchers have categorized nightmares (e.g., categorizing trauma-similar and replicative nightmares together) and different trauma types Characteristics of Chronic Nightmares 195 Table 2. Characteristics of Nightmares and Sleep Problems for Individuals Positive and Negative for Posttraumatic Stress Disorder (PTSD) Nightmare characteristics and sleep problems No. of hours slept per night Fear of going to sleep Depression upon waking Feeling rested upon waking Nightmares per week Nights with nightmares per week Nights with more than one nightmare per past week Disturbance of the nightmares Global depression (BDI-II) Overall sleep quality Panic symptoms upon waking from nightmare Replicative nightmare Trauma Similar nightmare Dissimilar nightmare PTSD positive PTSD negative M SD M SD F df 5.13 1.71 2.17 0.92 4.74 1.52 1.13 0.94 0.88 4.17 6.33 1.08 1.08 1.51 3.07 1.87 1.12 1.07 0.72 3.00 11.53** 7.27** 27.19*** 11.61** 4.44* 1, 90 1, 90 1, 90 1, 89 1, 88 3.82 2.08 2.50 1.55 11.19** 1, 90 2.30 3.12 25.81 14.63 2.23 0.78 10.98 4.13 1.13 2.85 14.39 11.00 1.70 0.77 10.79 3.78 7.30** 2.63 25.18*** 18.38*** 1, 88 1, 90 1, 91 1, 87 5.62 2.88 3.92 2.85 7.77** 1, 89 N % N % 2 18.03*** 17 32.69 1 2.77 27 8 51.92 15.38 17 18 47.22 50.00 2, 88 Note. Specific type of sleep problems were rated on a Likert scale ranging from 0 (not at all) to 4 (extremely). BDI-II ⫽ Beck Depression Inventory—II. * p ⬍ .05. ** p ⬍ .01. *** p ⬍ .001. (i.e., combat veterans may experience more replicative nightmares). The current study suggests it may be important to distinguish trauma-similar nightmares from replicative nightmares because differences were found on global depression, on overall frequency and severity of PTSD symptoms, and for each PTSD criterion category—reexperiencing, avoidance, and arousal. However, these results need to be replicated before conclusions can be drawn. A clear pattern emerged in the association between the degree of trauma similarity of the nightmare and symptoms of PTSD. Individuals who reported replicative nightmares also reported the greatest degree of distress. The present study did not find, however, that other indices of distress were lower for individuals with replicative nightmares, as did Schreuder et al. (2000). Indeed, replicative nightmares were associated with greater distress in terms of fewer hours of sleep per night, depression on waking, frequency of nights with nightmares, frequency of nights with more than one nightmare, total number of sleep problems, and overall sleep quality, in addition to the global depression and PTSD symptoms listed above. We did not, however, include a general measure of psychopathology (i.e., Symptom Checklist-90), as did Schreuder and colleagues. It is important to note, however, that trauma-similar and trauma-dissimilar nightmares were also associated with distress and sleep problems. This suggests that chronic nightmares have a negative impact on individuals’ functioning, regardless of the similarity to trauma experiences. The findings from analyses comparing PTSD-positive and PTSD-negative individuals were consistent with, and extended, previous work. Our findings re- 196 Davis, Byrd, Rhudy, and Wright vealed that of the 18 people who reported replicative nightmares, only 1 did not meet criteria for PTSD. Of those who met criteria for PTSD, 33% reported replicative nightmares, with 52% reporting trauma-similar nightmares and 15% reporting trauma-dissimilar nightmares. PTSD-positive individuals also reported greater overall distress and lower sleep quality and quantity. Results indicated that nightmares were associated with distress (global sleep quality and fear of going to sleep) even after PTSD symptoms were controlled. This suggests that chronic nightmares may be a major component of posttrauma response and may affect some areas of functioning independent of PTSD. This may help to explain why treatments that broadly target PTSD symptoms may not be successful at ameliorating nightmares (Forbes, Creamer, & Biddle, 2001; Schreuder, Igreja, van Dijk, & Kleijn, 2001) compared with treatments that directly target nightmares (Davis & Wright, 2007; Forbes et al., 2003; Krakow et al., 2001). Future research is needed to determine whether the association between nightmare content and distress severity is influenced by the length of time since the most recent trauma or the trauma that initiated the nightmare. Empirical studies have demonstrated that distress tends to be highest immediately after a trauma, with gradual amelioration across time (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Similarly, other studies have found that after a trauma, nightmares tend to be replicative or very similar to traumatic events, but over time change and distort (Hartmann, 1998). This brings into question the nature of this association. Is nightmare content a predictor of long-term difficulties? Is degree of trauma similarity of nightmare content a reflection of heightened distress or a maintaining factor? Does this relationship change when nightmares do not diminish, but remain a chronic problem? It will be important for future studies to address these questions. There are a few limitations of the present study to be considered. First, this was a sample of trauma-exposed individuals seeking treatment for their nightmares. These individuals likely represent an extreme end of the continuum of nightmare sufferers, so it is unclear to what extent the present results generalize to other trauma-exposed populations. The sample was also primarily composed of Caucasian women. Future studies will need to determine whether gender and ethnicity contribute to differences in the experience of nightmares. Finally, information distinguishing individuals who were lifelong nightmare sufferers versus individuals whose nightmares began following a trauma was gathered only in the second study. Previous research (e.g., van der Kolk et al., 1984) has suggested that this distinction may be an important component in understanding the nature of chronic nightmares. We plan to examine these issues on completion of the current treatment study. In spite of these limitations, the present study lends support to results of previous studies regarding the nature and characteristics of chronic nightmares in trauma-exposed persons. Although additional research is warranted, it does appear that all individuals with trauma, regardless of PTSD status, should be assessed for their experience of nightmares. It remains unclear whether the differing symptom levels by nightmare content suggest different considerations for or approaches to treatment of the nightmares. Future treatment studies should assess whether nightmare content is related to treatment outcome. Characteristics of Chronic Nightmares 197 REFERENCES American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author. American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text revision). Washington, DC: Author. Beck, A. T., Steer, R. A., & Brown, G. K. (1996). The Beck Depression Inventory—II. San Antonio, TX: Psychological Corporation. Beck, A. T., Steer, R. A., & Garbin, M. G. (1988). Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8, 77–100. Blake, D. D., Keane, T. M., Wine, P. R., Mora, C., Taylor, K. L., & Lyons, J. A. (1990). Prevalence of PTSD symptoms in combat veterans seeking medical treatment. Journal of Traumatic Stress, 3, 15–27. Blake, D. D., Weathers, F. W., Nagy, L. M., Kaloupek, D. G., Klauminzer, G., Charney, D. S., & Keane, T. M. (1990). A clinician rating scale for assessing current and lifetime PTSD: The CAPS-1. Behavior Therapy, 13, 187–188. Blake, D., Weathers, F., Nagy, L., Kaloupek, D., Klauminzer, G., Charney, D., et al. (1995). The development of the Clinician Administered PTSD Scale. Journal of Traumatic Stress, 8, 75–90. Buysse, D., Reynolds, C., Monk, T., Berman, S., & Kupfer, D. (1989). The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Research, 28, 193–213. Byrd, P. M., Davis, J. L., Schneider, C. N., Cantrell, C., Tracy, V., & Fernandez, S. (2006, November). Characteristics of chronic nightmare in a clinical, trauma-exposed sample. Poster presented at the annual meeting of the International Society of Traumatic Stress Studies. David, D., & Mellman, T. A. (1997). Dreams following Hurricane Andrew. Dreaming, 7, 209 –214. Davidson, J., Smith, R., & Kudler, H. (1989). Validity and reliability of the DSM–III criteria for posttraumatic stress disorder: Experiences with a structured interview. Journal of Nervous and Mental Disease, 177, 336 –341. Davis, J. L., & Wright, D. C. (2007). Randomized clinical trial for treatment of chronic nightmares in trauma-exposed adults. Journal of Traumatic Stress, 20, 123–133. Davis, J. L., Wright, D. C., & Borntrager, C. F. (2001). Trauma Related Nightmare Survey. Unpublished measure, University of Tulsa, Tulsa, OK. Derogatis, L. (1975). The SCL-90-R. Baltimore: Clinical Psychometrics Research. Derogatis, R. L., Lipman, R. S., & Covi, L. (1973). The SCL-90, an outpatient psychiatric rating scale. Psychopharmacological Bulletin, 9, 13–28. Esposito, K., Benitez, A., Barza, L., & Mellman, T. (1999). Evaluation of dream content in combatrelated PTSD. Journal of Traumatic Stress, 12, 681– 687. Falsetti, S. A., Resnick, H. S., & Davis, J. (2005). Multiple channel exposure therapy: Combining cognitive-behavioral therapies for the treatment of posttraumatic stress disorder with panic attacks. Behavior Modification, 29, 70 –94. Falsetti, S. A., Resnick, H. S., Resick, P. A., & Kilpatrick, D. G. (1993). The Modified PTSD Symptom Scale: A brief self-report measure of posttraumatic stress disorder. Behavioral Therapist, 161–162. Foa, E. B., Riggs, D. S., Dancu, C. V., & Rothbaum, B. O. (1993). Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress, 6, 459 – 473. Forbes, D., Creamer, M., & Biddle, D. (2001). The validity of the PTSD checklist as a measure of symptomatic change in combat-related PTSD. Behaviour Research and Therapy, 39, 977–986. Forbes, D., Phelps, A. J., McHugh, A. F., Debenham, P., Hopwood, M., & Creamer, M. (2003). Imagery rehearsal in the treatment of posttraumatic nightmares in Australian veterans with chronic combatrelated PTSD: 12-month follow-up data. Journal of Traumatic Stress, 16, 509 –513. Hartmann, E. (1998). Dreams and nightmares: The origin and meaning of dreams. Cambridge, MA: Perseus. Kessler, R., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52, 1048 –1060. Krakow, B., Hollifield, M., Johnston, L., Koss, M., Schrader, R., Warner, T. D., et al. (2001). Imagery rehearsal therapy for chronic nightmares in sexual assault survivors with posttraumatic stress disorder: A randomized controlled trial. JAMA, 286, 537–545. Mellman, T. A., David, D., Bustamante, V., Torres, J., & Fins, A. (2001). Dreams in the acute aftermath of trauma and their relationship to PTSD. Journal of Traumatic Stress, 14, 241–247. Mellman, T. A., Kulick-Bell, R., Ashlock, L., & Nolan, B. (1995). Sleep events among veterans with combat-related posttraumatic stress disorder. American Journal of Psychiatry, 152, 110 –115. Resick, P. A., Falsetti, S. A., Resnick, H. S., & Kilpatrick, D. G. (1991). The Modified PTSD Symptom Scale—Self-Report. St. Louis: University of Missouri & Charleston: Medical University of South Carolina, National Crime Victims Research and Treatment Center. 198 Davis, Byrd, Rhudy, and Wright Resnick, H. S. (1996). Psychometric review of Trauma Assessment for Adults (TAA). In B. H. Stamm (Ed.), Measurement of stress, trauma, and adaptation (pp. 362–365). Lutherville, MD: Sidran Press. Resnick, H. S., Best, C. L., Kilpatrick, D. G., Freedy, J. R., & Falsetti, S. A. (1993). Trauma Assessment for Adults—Self-Report Version. Unpublished scale, National Crime Victims Research and Treatment Center, Medical University of South Carolina. Ross, R. J., Ball, W. A., Sullivan, K. A., & Caroff, S. N. (1989). Sleep disturbance as the hallmark of posttraumatic stress disorder. American Journal of Psychiatry, 146, 697–707. Schreuder, B. J. N., Igreja, V., van Dijk, J., & Kleijn, W. (2001). Intrusive re-experiencing of chronic strife or war. Advances in Psychiatric Treatment, 7, 102–108. Schreuder, B. J. N., Kleijn, W. C., & Rooijmans, H. G. M. (2000). Nocturnal re-experiencing more than forty years after war trauma. Journal of Traumatic Stress, 13, 453– 463. Spitzer, R. L., Williams, J. B. W., & Gibbon, M. (1995). Structured Clinical Interview for DSM–IV, patient version. New York: New York State Psychiatric Institute, Biometrics Research Department. Thompson, K. E., Hamilton, M., & West, J. A. (1995). Group treatment for nightmares in veterans with combat-related PTSD. National Centre for PTSD Clinical Quarterly, 13–17. van der Kolk, B., Blitz, R., Burr, W., Sherry, S., & Hartmann, E. (1984). Nightmares and trauma: A comparison of nightmares after combat with lifelong nightmares in veterans. American Journal of Psychiatry, 141, 187–190. Weathers, F. W., Ruscio, A. M., & Keane, T. M. (1999). Psychometric properties of nine scoring rule for the Clinician Administered Posttraumatic Stress Disorder Scale. Psychological Assessment, 11, 124 –133. Wright, D. C., Davis, J. L., Inness, T., & Stem, P. (2003). Convergent validity of PTSD assessment measures in a sample of survivors of domestic violence. Poster presented at the annual meeting of the Oklahoma Psychological Association, Oklahoma City, OK.