Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
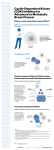
Undergraduate Category:PhysicalandLifeSciences DegreeLevel:B.S.HealthScience AbstractID#1048 Validating CDK4 and XPO1 dependencies in a pediatric undifferentiated sarcoma Bryan Kynnap1,3, Andrew L. Hong2,3,5, Glenn Cowley5, Moony Tseng5, Jamie Cheah5, Mihir Doshi3,5,Coyin Oh5, Alanna Church2, Carlos Rodriguez-Galindo2,3, Katherine Janeway2,3, Kimberly Stegmaier2,3,5, Paul van Hummelen3, Ali Samji5, David Root5, Jesse Boehm5, William C. Hahn3,4,5 1 Northeastern University; 2 Boston Children’s Hospital, 3 Dana-Farber Cancer Institute, 4 Brigham and Woman’s Hospital, Boston, MA, 5 Broad Institute, Cambridge, MA Introduction Results The intersection between nanomedicine and precision medicine depends on the understanding of cell pathway mechanisms. Undifferentiated sarcomas account for up to 20% of all soft tissue sarcomas and therapies for this type of cancer are ill defined with poor outcomes for those with metastatic disease. For patients with undifferentiated sarcomas, understanding of the biology is limited due to its rarity and lack of in-vitro models. We have developed a novel undifferentiated sarcoma cell line from a pediatric patient with metastatic disease. This cell line is genomically silent but carries a number of novel fusions. Through an orthogonal set of screens utilizing small molecules, shRNAs and CRISPRs, we identified CDK4 and XPO1 as potential actionable targets. C. G. Figure G. After cells are treated with KPT-330 for 24 hours, we see Caspase-3 activation and p53 accumulation inside the nuclear envelope. Figure B. Validation of knockdown with shRNAs to CDK4 in Peds015T. Approach Proof of Concept: Peds015T Undifferentiated Sarcoma Patient’s clinical course B. Results Cell line’s course 1) Generated from a metastatic brain lesion in RPMI media Figure C. Increased G0/G1 cell cycle arrest in Peds015T and TM87 when compared to A549 cells when treated with CDK4 inhibition after 24 hours. D. H. 2) Rapid growth without supplements Figure H. After cells are treated with KPT-330 for 24 hours, we see CRM1/XPO1 inhibitors activating p53 pathway. 3) Currently at passage 150+ Figure D. Inhibition of CDK4 with LEE011 causes decreased expression of pRb(S807/811). E. Results A. Figure F. Validation of shXPO1 knockdown in an early passage PEDS015T compared to historical samples. nM A549 796 A204 138 SMS-CTR A673 Peds015T 274 262 45 TM-87 18 TC-32 23 Figure E. Validation of targeting XPO1 drug sensitivities. F. Figure A. Validation of targeting CDK4 drug sensitivities of the highlighted compound in an early passage of the undifferentiated sarcoma cell line compared to other cell lines (e.g. rhabdomyosarcoma, Ewing sarcomas and rhabdoid tumors) with IC50 dose curves. IC50 Conclusions We have validated in-vitro dependencies to CDK4 and XPO1 using shRNAs and agents currently in clinical trials such as Palbociclib and KPT-330. When compared with other poorly differentiated sarcomas (e.g. rhabdomyosarcoma, Ewing sarcoma) and other poorly differentiated cancers such as rhabdoid tumors, we see similar correlations. Interestingly, for KPT-330, we have identified nuclear accumulation of p53 and subsequent activation of its pathway as a potential mechanism for cell death. In the case where small molecule therapeutics are lacking, nanotechnology could be employed as a potential delivery of shRNAs. References 1. Vanarsdale, T., Boshoff, C., Arndt, K., & Abraham, R. (2015). Molecular Pathways: Targeting the Cyclin D-CDK4/6 Axis for Cancer Treatment. Clinical Cancer Research. 2. Fletcher, C. (2013). The evolving classification of soft tissue tumors - an update based on the new 2013 WHO classification. Histopathology, 2-11. 3. Ho, Y. (n.d.). The expression of CRM1 is associated with prognosis in human osteosarcoma. Oncol Rep Oncology Reports. Acknowledgments This CaNCURE co-op research project was supported by National Cancer Institute grant #1CA174650-02 (BK), CureSearch for Children’s Cancer (ALH), and NIH 5K12 HD052896-09 (ALH).