Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
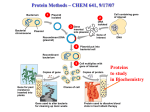
A reprint from American Scientist the magazine of Sigma Xi, The Scientific Research Society This reprint is provided for personal and noncommercial use. For any other use, please send a request to Permissions, American Scientist, P.O. Box 13975, Research Triangle Park, NC, 27709, U.S.A., or by electronic mail to [email protected]. ©Sigma Xi, The Scientific Research Society and other rightsholders Feature Articles Fighting Cancer Through the Study of Sarcomas Although rare, cancers of the muscle, bone or fat carry the same molecular errors as other tumors, making them ideal subjects for the discovery of new therapies Igor Matushansky and Robert G. Maki A 50–year-old Finnish woman was having mild stomach pains when she went to see her doctor in 1996. The physician in Helsinki found a large abdominal mass, and things got worse from there. Further exams discovered tumors, 7 and 10 centimeters in diameter, on her stomach, plus many small nodules of spreading cancer. Surgeons removed as much of it as they could find, but the diagnosis was grim. It was a gastrointestinal stromal tumor, or GIST, a cancer of the connective tissue in the gut that was inevitably fatal if surgery failed. Igor Matushansky is a fellow in medical oncology and a postdoctoral fellow in the laboratory of Carlos Cordon-Cardo at Memorial Sloan-Kettering Cancer Center in New York. He attended Columbia University for undergraduate studies and obtained his Ph.D. and M.D. from Yeshiva University’s Albert Einstein College of Medicine. Following a residency in internal medicine at the Weil-Cornell Medical Center, his work has focused on the relation between cellular differentiation and tumor formation and the application of this knowledge to the management of sarcomas. Robert G. Maki is an assistant professor at Weil Medical College of Cornell University and an assistant member and co-director of the Adult Sarcoma Program at Memorial Sloan-Kettering Cancer Center. After undergraduate studies at Northwestern University, he received his Ph.D. and M.D. from Cornell University Medical College. He completed a fellowship and residency at the Dana Farber Cancer Institute and Brigham and Women’s Hospital in Boston. His publications have examined the use of heat-shock proteins as tumor vaccines and the clinical care of sarcomas. Address for Matushansky: Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, Room C1179, New York, NY 10021. Internet: [email protected] 414 American Scientist, Volume 93 Two years later the cancer was back, and doctors had to operate again to remove growths on the liver and abdominal wall. Another surgery that year excised more tumors on the liver and ovary. The woman’s doctors tried to slow the proliferating cells with an intense barrage of combined chemotherapeutics—seven cycles using four different drugs over a five-month period—without success. As the cancer spread, it blocked the patient’s intestine, requiring yet another operation. When the surgeon went in to cut away the blockage, he found and removed 45 additional tumors. The patient began taking large daily doses of two cuttingedge, immune-system–enhancing drugs, to little effect. Having exhausted other options, the woman’s oncologist, Heikki Joensuu at the Helsinki University Central Hospital, suggested an experimental drug, STI571, which had just begun phase I testing for chronic myelogenous leukemia—a completely different kind of cancer from the soft-tissue tumors his patient carried. It was a desperate attempt to save the patient’s life, so despite the lack of any clinical supporting data, the hospital agreed to let him try. Two weeks later, an MRI exam showed the woman’s tumors were 40 percent smaller. Two months later, they had shrunk half as much again. At eight months, they were further reduced in size; about a quarter were no longer detectable. What’s more, the tumor cells that remained had stopped dividing and no longer showed the molecular signature of cancer. It was an incredible improvement. Why did Joensuu think to try this particular drug? Because he knew, based on the work of others, the molecular basis of GIST: The abnormal protein that caused his patient’s tumor was similar to the one that caused the leukemia for which the drug was approved. Furthermore, some reports indicated that STI571 could work on both types of proteins—at least in a dish of cultured cells. In the end, this success owed much to many: The paper describing this striking case included as coauthors doctors and scientists from Helsinki, Turku University (also in Finland), Massachusetts Institute of Technology, Harvard, the Oregon Health Sciences University and the pharmaceutical company Novartis, which made the compound (now called imatinib and sold under the name Gleevec). Is this drug the long-sought silver bullet, the cure for all types of cancer? No. But it does illustrate how discoveries in research labs can quickly pay off in clinics. It is an early fruit from what promises to be a great harvest of medical advances made possible by two decades of accelerating progress in understanding how cells work. And it can’t come soon enough. Divide and Conquer In the United States in 2005, almost two and a half million people will be diagnosed with some form of cancer, and about 570,000 people are expected to die of this disease. Indeed, cancer passed heart disease this year as the top killer of people under age 85. Although © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. SPL/Photo Researchers, Inc. Figure 1. From a distance, cancer looks like a single disease: Cells divide uncontrollably and haphazardly. But up close, cancer is extremely diverse, not just because it involves different tissues, but because different genetic errors can turn a normal cell into a cancer cell. Among the subtypes of cancer, sarcomas—a relatively rare kind of tumor—represent a considerable part of that diversity, and many of the mutations that cause sarcomas also cause other cancers. As a result, many scientists who study the molecular basis of cancer, including the authors, use sarcoma cells as representative models for their investigations. This false-color image is a scanning electron micrograph of one type of sarcoma, a giant cell tumor of bone (brown), infiltrating healthy bone tissue (gray). these survival statistics would be even grimmer without modern medicine, the best efforts remain inadequate. The three pillars of treatment for cancer are surgery, radiation and chemotherapy. Of these three, chemotherapy is the least discriminating. Whereas surgical excision and radiation therapy are site-specific, standard chemotherapy kills dividing cells everywhere in the body. The rationale for administering such poison is that the cells that split frequently—usually cancer cells—should suffer the most. Although the strategy works well in some instances, say for treating leukemias, other types of cancer do not grow rapidly and are resistant to chemotherapy. Furthermore, normal cells that divide often—those in hair follicles and the lining of the gut, for example—are destroyed too, causing hair loss and diarrhea. Additional medications can alleviate some of these side effects but do not solve the fundamental problem, which is a lack of specificity. www.americanscientist.org Although new therapies based on advances in molecular biology have begun to enter clinical practice, the “holy grail” of oncology—a treatment that is both effective and completely specific to cancer cells—remains unknown. In fact, a single cure now seems more elusive than ever as physicians continue to learn about the many physiological changes that distinguish different forms of cancer from one another and from normal cells. This heterogeneity among cancers is reflected in a relatively rare, highly diverse class of tumors called sarcomas. Thus, sarcomas are good (and popular) subjects for the study of therapies that physicians can use on other types of malignancies: More than a dozen medical centers and hospitals around the country specialize in sarcoma research and treatment. The word “σαρκωµα”appears in the writings of the physician-philosopher Galen, who lived during the latter part of the second century a.d. In its original Greek, the term sarcoma describes a fleshy growth. Doctors use the word today to describe cancers derived from connective tissues such as bone, muscle, fat or cartilage. Each year in the United States, clinicians diagnose approximately 10,000 new sarcoma cases, encompassing 50 different types of cancer, each with its own distinctive biology. Because relatively few people are afflicted with each sarcoma subtype, the disease doesn’t lend itself to studies that require many patients, such as large-scale searches for susceptibility genes or big, randomized trials. Instead, most investigators look at pathological mechanisms using smallscale studies that are carried out on the cellular level. Consequently, scientists now know more about how sarcomas work than their scarcity might suggest, and clinical trials for sarcoma treatments are likely to reflect specific molecular data from experiments in a laboratory. © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. 2005 September–October 415 sarcomas (0.7%) oral cavity (2.1%) digestive system (18.5%) respiratory system (13.5%) skin (4.8%) breast (15.5%) genitals & reproductive system (23.4%) urinary system (7.4%) nervous & endocrine systems (3.4%) blood (3.7%) lymphatic system (4.7%) other & unspecified (2.3%) 9 50 45 8 40 7 35 6 30 5 25 4 3 20 15 2 10 1 5 0 <5 5–9 10–14 15–19 20–24 25–29 30–34 35–39 40–44 45–59 60–74 75+ age incidence per year per million percent of cancers 10 0 Figure 2. Sarcomas are a rare subtype of cancer, accounting for less than one percent of predicted cancer diagnoses in 2005 (top). However, these tumors make up a larger proportion of cancers among children. Excluding Kaposi’s sarcoma (which is restricted to the elderly or patients with suppressed immune systems), the percentage of all cancers that are soft-tissue sarcomas is highest for patients between 10 and 14 years of age (red bars). However, in absolute terms, soft-tissue sarcomas are more likely to occur in older people (pink bars) because they get cancer more frequently than younger people. The number of diagnoses by tissue type is from the American Cancer Society’s Cancer Facts and Figures 2005 and excludes basal- and squamous-cell skin cancer. The relative and absolute incidences of sarcomas by patient age are from Albritton 2005, based on data from 1975 to 1999. Absolute incidence data for people 45 years and older were not included in that report, although other studies show that the rates continue to climb with increasing age. Our own research at Memorial Sloan-Kettering Cancer Center in New York strives to understand how sarcomas arise and to exploit that knowledge in the development of new treatments. Our work and the work of our fellow physician-scientists has led to several therapies for individual sarcomas, some of which are also proving useful in the fight against common types of tumors, such as those found in some lung cancers. This review highlights some of these advances. Going After the Genes Like other cancers, sarcomas are products of genetic mutations, which can take many forms. One particular category of genetic errors, called chromosomal translocations, is responsible for several sarcomas. A chromosome is a single long strand of DNA—thousands of times longer than a cell is wide. When a human cell is preparing to divide, it copies each of its 23 pairs of chromosomes so that each daughter cell can receive a complete set. Occasionally, a strand of DNA will break during this process. The cell usually mends these fractures correctly, or, if it cannot, trips the self-destruct switch (leading to programmed cell death, or apoptosis). But sometimes a cell will incorrectly join two or more different chromosomes, yielding a translocation. If the cell subsequently escapes its own destruction, daughter cells can inherit too many or too few copies of that piece of chro- Figure 3. Normal fat cells (above, left) are characterized by their large size, storage vacuoles and sparse nuclei (stained purple in this image). By contrast, cells from a high-grade liposarcoma are densely packed (above, right). The cells are shown at 400× magnification. Sarcomas tend to be a particularly invasive form of cancer, so surgical treatments often take surrounding healthy tissue as a precaution against leaving malignant cells behind. In some cases the damage can be mitigated by surgical reconstruction. The image at right shows a three-dimensional projection of computerized tomography scans from a patient with osteosarcoma who received a bone graft and total replacement of the right hip joint. (Cell images appear courtesy of Carlos Cordon-Cardo, Memorial Sloan-Kettering Cancer Center; CT scan is courtesy of Edward Y. Cheng, University of Minnesota.) 416 American Scientist, Volume 93 © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. daughter cells cell division incorrect repair or cell balanced normal unbalanced unbalanced normal normal DNA correct repair Figure 4. When a cell is preparing to divide, it must copy the DNA that makes up each chromosome so that both daughter cells receive a complete set. The DNA strands sometimes break during this process, but most of the time the cell rejoins the correct ends with no lasting damage. However, if a cell repairs the break incorrectly, daughter cells may inherit a so-called chromosomal translocation, in which portions of two different chromosomes are swapped. When this happens, the outcome will be more or less harmful depending on the random sorting of chromosomes into the cellular progeny. Unbalanced translocations represent too many copies of some genes and too few copies of others; balanced translocations may cause problems (or not) depending on the site of the break. Translocations occur in many types of tumors, but they are particularly common in sarcomas. mosome. Furthermore, if the DNA is snapped and incorrectly repaired in a region that specifies a protein, that valuable piece of the genetic code— that gene—may be destroyed, leaving the cell with only one remaining copy on the unbroken partner in the chromosome pair. Another possibility is that the improperly repaired DNA will encode a “fusion protein,” made from the sequences of two different genes spliced together. Many such fusion proteins are merely ineffective, like a bicycle with oars instead of pedals, but some can be dangerous. If the original performed some critical function in the cell, such as regulating cell division, the fusion protein can cause big problems. These breaking-and-joining events do not happen randomly, and certain translocations cause specific kinds of cancer. One example is the abnormal inheritance of an extra copy of the long arm of chromosome 12, which causes a version of the most common soft-tissue www.americanscientist.org cancer, liposarcoma—the class of sarcoma that develops from fat cells. Thanks to recent advances in “gene profiling” (a technique that measures gene activity), scientists have identified a cause of one subset of this class, the so-called dedifferentiated liposarcomas. With two normal copies of chromosome 12 plus the extra fragment, cells manufacture too much of the protein encoded by one of the resident genes: the cyclin-dependent kinase 4 gene, a mouthful that usually goes by the shorthand CDK4. As its name indicates, the CDK4 protein is a kinase—an enzyme that adds phosphate groups onto other proteins as a means of controlling how active or inactive they are. It so happens that this particular kinase acts on one of the master switches of cell division, the stoutly named retinoblastoma tumor suppressor, or RB, which acts through a DNA-binding protein called E2F. A glut of CDK4 causes RB to have an excessive number of phosphate groups attached, thereby jam- ming the cell-division switch in the on position—a hallmark of cancer. Once scientists understood this chain of events, they hypothesized that blocking CDK4 might slow the spread of liposarcoma. One candidate drug is flavopiridol, which inhibits several kinases, including CDK4. Our colleagues Gary K. Schwartz and Samuel Singer at Memorial Sloan-Kettering have shown that this drug destroys liposarcomas in the culture dish and in mice that carry human liposarcomas. Several clinical trials are now testing flavopiridol for various cancers. Sarcoma Antigens 101 Some tumors produce characteristic proteins. For example, melanomas churn out the pigment melanin and related molecules. Thus, training the patient’s immune system to attack such proteins—by using a vaccine, for example—can help the body identify the malignant cells and get rid of the cancer. This process of teaching the © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. 2005 September–October 417 three or more copies CDK4 gene (mutant) two copies CDK4 gene (normal) cyt P P leus m sm plas opla cyto RCBDK4 nuc E2F cell-division gene P P leus a P RB P nuc P CDK 4 P P two copies CDK4 gene (normal) P P P CDK4 P CPDK4 P cell-division gene RB P CDK4 on E2F RB sm opla m cyt las top c yl e u s us nuc cle nu CDK4 P CDK4 inactivates RB with phosphate RB P P P P RB CDK4 P P P P P P E2F cell-division gene CDK4 CDK4 off off b flavopiridol blocks CDK4 three or more copies CDK4 gene (mutant) iridol P idol P flavop three or morePcopies CDK4 gene (mutant) P P P P P C P DK4 PCDK4 CDKP4 P RB CDK4 RCBDK4 CDK4 P P P P P P cell-division gene P B cell-division gene E2F RB R P P P CDK4 CDK4 CDK4 on P off c d cell-division gene P copy of the long arm of chromosome P12. One of the genes gene E2F cell-division Figure 5.P Certain liposarcomas, or cancers of fat cells, are associated with an extra on in this region is CDK4, which encodes a protein that regulates one of the master switches of cell division, known as RB, by adding phosphate off groups (a). Normally, active and inactive forms of RB are in equilibrium, allowing some molecules to attach to the DNA-binding protein E2F, thereby keeping the genes that control cell division turned off (b). Too much CDK4 disrupts this balance, preventing RB molecules from keepflavopiridol blocks CDK4 ing the critical genes silent (c). The drug flavopiridol attempts to restore order by inhibiting CDK4 (d). flavopir ol P to create antibodies vopirid idol The Japanese team started by col- University of Wisconsin Children’s immune system fla three or morePcopies CDK4 gene (mutant) flavopiridol Hospital in Madison described their against cancer-specific (or in the case lecting and isolating the patient’sblocks own CDK4 P experiments with aidtype of cancer of melanin, cancer-enriched) proteins dendritic cells, a part of the immune sysC flavopir DK4 ir ol P idol PCDK4immunotherapy. DKP4 whose job it is to engulf P C P flavop called alveolar rhabdomyosarcoma—the tem invading is called RB P P P P P most common type of soft-tissue sarSarcomas are excellent candidates microbes, chew them up and wear P the P P P coma among children. This sarcoma for immunotherapy because many pieces on their outer membranes. (This P CDK4 CDK4 RBtypically characterized geneC dismemberment allows another type is byCDK4 a translo-CDK4 have Dchromosomal translocations that E2F cell-division RB DK4 C K4 generate fusion proteins not seen in of immune cell, the B cell, to make an- cation of chromosomes 2 and 13 that off any other cell of the cell-division body. Thegene im- tibodies that recognize each chunk, or fuses the genes PAX3 and FKHR, both P B P cell-division genetranscriptionP factors E2F mune Psystem can thus attack these antigen.) of which encode Matsuzaki and his Rcolleagues on that bind to DNA and switch specific molecules (and the cancer cells already knew that a translocation of (proteins off flavopir P P P P P CDK 4 P two copies CDK4 gene (normal) P P P CDK4 P CPDK4 sm opla toplasm cyt cy l e u su c l e u s n sm plasm opla cyto cyt s leus ucleu n nuc nuc E2F P P sm leus opla P cyt cyt sm leus opla nuc American Scientist, Volume 93 nuc E2F 418 P nuc P sm opla toplasm cyt cy l e u su c l e u s n P P P P E2F that contain them) without harming one of this patient’s X chromosomes healthy tissue. Of course, the body and a chromosome 18 had fused two does not automatically recognize the genes together so that they encoded a mutant proteins as foreign. If it did, unique protein. In the lab, the invesblocks CDK4 theflavopiridol tumor never would have appeared tigators combined the dendritic cells in the first place. Part of the problem withlthat protein and then returned the flavopir P pirido id ol abnormal is access: The proteins mayflavo“stimulated” cells to the patient. The P not show up on the surface of the cell girl’s immune system began to recogP at all; they may be present only within, nize the sarcoma, and the treatment CDK4 DK4 where they are hiddenRB from immune- Ctemporarily suppressed the growth of system surveillance. Fortunately, in the cancer that had spread to her lung. some instances, fusion proteins do ap- Although such outcomes have not yet B cell membrane, gene been tested systematically, the strong pear on Rthe albeit in E2F cell-division quantities too small to stimulate the scientific rationale and individual sucoff immune system. The challenge then cesses like that of Matsuzaki’s patient is only to generate antibodies to these have sparked dozens of clinical trials cancer-specific proteins. A few years that use a person’s own dendritic cells ago, investigators led by Akinobu as a form of therapy for advanced canMatsuzaki at the Graduate School of cers of the kidney, prostate, breast, coMedical Sciences in Fukuoka, Japan, lon and lung. succeeded in doing so in the treatment of an 11-year-old girl with synovial Sarcomas and Sick Kids sarcoma that had spread to other parts In a report published in 1997, Edmond S. Massuda and his colleagues at the of her body. other genes on and off). Normally, the PAX3 protein organizes embryonic muscle development, and FKHR is widespread. The fusion protein created from the melding of these genes causes muscle cells to remain immature and hence susceptible to other cancer-promoting events. The investigators showed that this fusion protein is about a hundred times more effective at activating PAX3-regulated genes than PAX3 itself. Massuda and his coworkers took advantage of this property by taking the gene for diphtheria toxin A—a potent cellular poison—and modifying it so that it would be switched on only in the presence of the PAX3 protein. They then added that carefully crafted DNA to different strains of cultured cells, some of which carried the PAX3-FKHR mutant. Sure enough, the additional DNA selectively killed those cells that manufactured the fusion protein. Fur- © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. thermore, when they added the fusion gene to otherwise normal cells, those cells also died in the presence of the PAX3-regulated toxin. Although the thought of injecting toxin genes into patients and trusting a bit of DNA alongside to keep them from harming the rest of the body may seem dangerous, the results from these experiments give hope that the effects will be specific to the tumor. Like the cancer Massuda is trying to cure, Ewing sarcoma is one of the most common connective-tissue tumors in children and young adults, although it more commonly affects bone rather than soft tissues. It also stems from a chromosomal rearrangement, in this case the fusion of a gene from chromosome 22 with one from chromosome 11. The resultant protein transforms normal bone cells into cancer cells. In laboratory experiments, cultured bone cells proliferate rapidly when one adds this fusion protein and, conversely, stop dividing when it is removed— making the aberrant protein an ideal therapeutic target. One new technology for getting rid of a particular protein in the cell is called small interference RNA (siRNA). In 2004, a team of clinical scientists headed by Howard A. Chansky at the University of Washington School of Medicine in Seattle reported on their successful application of this tool, which is both powerful and specific, to the task of suppressing the fusion protein responsible for Ewing sarcoma. Figure 6. Many translocations that lead to cancer involve the fusion of two genes in such a way that they encode a single protein. Scientists believe such “fusion proteins” cause several cancers, including a number of sarcomas, by binding to DNA and disrupting normal gene expression (top). However, because fusion proteins are unique to the cancer cells, they also provide a means of attacking the tumor without harming healthy tissue. In one experimental therapy, scientists created a small interfering RNA, or siRNA, that included a sequence complementary to the fusion RNA. When the two RNA strands zipped together, the cell interpreted the double-stranded RNA as a virus and destroyed it (middle). Another potentially tumor-specific therapy capitalizes on the abnormal properties of the fusion protein by adding an engineered piece of DNA that encodes a toxin. The toxin gene only turns on in the presence of the abnormal protein (bottom). Thus, cancer cells, which contain the fusion protein, create the toxin and die, whereas normal cells lack the fusion protein, do not turn on the toxin and are spared. www.americanscientist.org The approach uses many short pieces of RNA that carry the complementary sequence to the fusion gene’s RNA. The interfering RNA binds to its target to form a double-stranded molecule that the cell perceives as a virus and snips apart. Without its RNA template, new copies of the fusion protein cannot be made, and existing copies are soon degraded. Using this strategy, Chansky and his coworkers silenced the mutant gene in Ewing sarcoma cells in culture, thereby preventing further cell division. These results represent the first use of siRNA to target the RNA that cancer cells make, and this approach will almost certainly lead to new therapies. GIST Deserts Although siRNA and similar experimental avenues for fighting cancer are still far from routine clinical application, the use of imatinib for treating GIST (sparked by the recovery of the Finnish woman) has now become accepted for certain advanced cases. How exactly does the drug work? disease fusion protein fusion fusion protein protein cytoplasm leus cnyut ocp l a s m cytoplasm nucleus nucleus RNA RNA RNA disease disease fusion gene cancer fusion gene fusion gene cancer cancer wrong genes on wrong genes on wrong genes on siRNA therapy siRNA therapy siRNA therapy cytoplasm custom siRNA custom custom siRNA siRNA leus cnyut ocp l a s m cytoplasm nucleus nucleus fusion gene fusion gene fusion gene genes stay off genes stay off genes stay off cytopla cancer-specific gene therapy sm cancer-specific gene therapy cancer-specific gene therapy cyto c y t o ppllaa s m sm toxin gene toxin gene toxin gene toxin gene toxin gene toxin gene toxin gene toxin gene toxin gene fusion gene fusion gene fusion gene fusion protein turns on toxin fusion protein fusion protein toxin gene turns on toxin turns on toxin toxin gene toxin gene © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. cancer cancer cancer 2005 September–October 419 tinib benefits more than 80 percent of patients. Unfortunately, this upswing is only a respite in some cases. The tumors vary in their genetic make-up, which presumably explains the slow remedy seen by some patients and the unresponsiveness of others. The latter group often carries tumors that have little or no KIT protein, a variety that can also be found among patients who initially respond well to the drug, but worsen as the susceptible cells die off, leaving others to spawn new tumors that resist imatinib. Figure 7. Gastrointestinal stromal tumor, or GIST, is an aggressive type of sarcoma that typically resists chemotherapy and radiation, leaving surgery as the only treatment. No therapies exist for advanced cases. However, five years ago a woman with widespread, inoperable GIST received a speculative form of treatment based solely on her tumor’s molecular resemblance to an unrelated form of cancer. A PET scan (which measures metabolic activity with a radioactive tracer) taken before treatment began shows the brain, a distended kidney (a consequence of the disease) and many abdominal tumors (left). Four weeks after starting treatment with STI571, now called imatinib, there was no abnormal uptake of the tracer in the abdomen, indicating that the cancer was no longer growing at an accelerated rate. (Images courtesy of Heikki Joensuu.) GIST is usually caused by mutations in a gene called—no kidding—v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog. This tongue-twister, called KIT for short, codes for a protein also named KIT, a kinase like CDK4, but one that adds phosphate groups only to tyrosine—one of the 20 different types of amino acids that make up human proteins. Tyrosine kinases are often embedded in the outer membrane of the cell. There, they can receive signals from the immediate environment and transmit them to the nucleus (via a chain of other messengers), thereby helping to determine which genes are turned on or off. Overactive tyrosine kinases cause many kinds of tumors. Although the KIT protein shows up in other cancers, such as small-cell lung cancer and seminoma of the testes, only GIST contains mutations in the gene that cause unregulated activity. In 420 American Scientist, Volume 93 a 2001 paper, David A. Tuveson, then a postdoctoral fellow in the laboratory of Tyler Jacks at MIT, showed that imatinib interferes with normal and mutant KIT and inhibits the growth of cultured GIST cells that contain the latter. These observations helped to hasten the Food and Drug Administration’s approval of imatinib for the treatment of GIST tumors that have spread so widely that surgery is impossible—granted a scant 10 months after the publication of the original case study. (Customarily, experimental drugs are first approved for use in people who have exhausted their other options.) To grasp the striking success of imatinib, one needs to understand that prior to its use there were no good treatments for GISTs. Most of these tumors are highly resistant to chemo- and radio-therapy, and multiple surgeries were the only palliative option. Now, the combination of surgery and ima- Beyond Sarcomas The success of imatinib has led to investigation of a growing number of compounds that interfere with the development of more-common (nonsarcoma) tumors in the lung, colon, breast and prostate. Among the approved drugs are gefitinib (Iressa) and erlotinib (Tarceva), which treat non–smallcell lung cancer (NSCLC) by inhibiting a tyrosine kinase called the epidermalgrowth-factor receptor (EGFR). This protein is overactive in many solid tumors and is typically associated with a poor prognosis. Early clinical trials of gefitinib in the United States and Japan showed that almost half of the patients improved while taking the drug—remarkable considering their tumors had resisted standard chemotherapy. However, a different set of studies showed that adding gefitinib to conventional therapy did not provide an additional benefit. Nevertheless, the FDA quickly approved gefitinib for advanced NSCLC in patients whose condition had worsened under standard therapy. Erlotinib also works by inhibiting the EGFR. In clinical trials, oncologists saw modest success treating NSCLC and bronchoalveolar carcinoma, another form of lung cancer. Evidently, the people who responded the best to erlotinib were those who carried mutations in their EGFR. In November of 2004, the FDA approved, after priority review, erlotinib for the treatment of patients with advanced non–small-cell lung cancer who did not improve after traditional chemotherapy. Because many of the most common cancers contain EGFR proteins, it makes sense to test all the available inhibitors of this protein to find out which are best for each combination of tumor type and genetic constitution. Such studies are now going on, and they should help © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. improve the treatment of these types of cancer within the next few years. Over the past decade, scientists have made remarkable discoveries of the molecular mechanisms that cause sarcomas and other cancers and are just now seeing the payoff in the form of treatments that specifically target genes or proteins of those cancer cells. However, investigators have much more to learn about the translocationspecific sarcomas, not to mention the large majority of cancers that do not carry a known genetic abnormality. It is our hope that the knowledge obtained from the study of the better-understood sarcomas will apply to their uncharacterized relatives and to solid tumors as a whole, as demonstrated by recent advances in therapies for lung cancer. We believe strongly that the systematic analysis of these remarkable tumors will result in an enormous benefit to patients within the next few years. www.americanscientist.org Bibliography Albritton, K. H. 2005. Sarcomas in adolescents and young adults. Hematology / Oncology Clinics of North America 19:527– 546. Cheng, E. Y. 2005. Surgical management of sarcomas. Hematology / Oncology Clinics of North America 19:451– 470. Chansky, H. A., F. Barahmand-Pour, Q. Mei, W. Kahn-Farooqi, A. Zielinska-Kwiatkowska, M. Blackburn, K. Chansky, E. U. Conrad III, J. D. Bruckner, T. K. Greenlee and L. Yang. 2004. Targeting of EWS/FLI-1 by RNA interference attenuates the tumor phenotype of Ewing’s sarcoma cells in vitro. Journal of Orthopaedic Research 22:910–917. Dagher, R., M. Cohen, G. Williams, M. Rothmann, J. Gobburu, G. Robbie, A. Rahman, G. Chen, A. Staten, D. Griebel and R. Pazdur. 2002. Imatinib mesylate in the treatment of metastatic and/or unresectable malignant gastrointestinal stromal tumors. Clinical Cancer Research 8:3034–3038. Joensuu, H., P. J. Roberts, M. Sarlomo-Rikala, L. C. Andersson, P. Tervahartiala, D. Tuveson, S. L. Silberman, R. Capdeville, S. Dimitrijevic, B. Druker and G. D. Demetri. 2001. Effect of the Tyrosine kinase inhibitor STI571 in a patient with a metastatic gastrointestinal stromal tumor. New England Journal of Medicine 344:1052–1056. Massuda, E. S., E. J. Dunphy, R. A. Redman, J. J. Schreiber, L. E. Nauta, F. G. Barr, I. H. Maxwell and T. P. Cripe. 1997. Regulated expression of the diphtheria toxin A chain by a tumor-specific chimeric transcription factor results in selective toxicity for alveolar rhabdomyosarcoma cells. Proceedings of the National Academy of the U.S.A. 94:14701–14706. Matushansky, I., and R. G. Maki. 2005. Mechanisms of sarcomagenesis. Hematology / Oncology Clinics of North America 19:427– 449. Matsuzaki, A., A. Suminoe, H. Hattori, T. Hoshina and T. Hara. 2002. Immunotherapy with autologous dendritic cells and tumor-specific synthetic peptides for synovial sarcoma. Journal of Pediatric Hematology/Oncology 24:220–223. Tuveson, D. A., N. A. Willis, T. Jacks, J. D. Griffin, S. Singer, C. D. Fletcher, J. A. Fletcher and G. D. Demetri. 2001. STI571 inactivation of the gastrointestinal stromal tumor c-KIT oncoprotein: Biological and clinical implications. Oncogene 20:5054–5058. © 2005 Sigma Xi, The Scientific Research Society. Reproduction with permission only. Contact [email protected]. For relevant Web links, consult this issue of American Scientist Online: http://www.americanscientist.org/ IssueTOC/issue/761 2005 September–October 421