Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
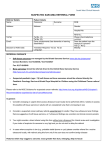
URGENT SUSPECTED CANCER REFERRAL FORM SUSPECTED MALIGNANT SOFT TISSUE TUMOUR IN ADULTS Sarcoma Diagnostic Clinic Patient Details Full Name: Other Names: Sex: Date of Birth: NHS No.: Hospital No.: Interpreter Required? Transport required? Address: Yes Yes /No /No Home Phone No.: Mobile Phone No.: Work Phone No.: Preferred Phone No.: Email Address: * N.B. It is essential that you provide a current contact telephone number for the patient so that the Health Board can contact the patient within 24-hours to arrange a convenient appointment. Practice Details Referring GP: Registered GP: GMC Code: Practice Name & Address: Practice Code: LHB Code: Tel No: Date seen by GP: Fax No: Decision to refer date: 7A3 SOFT TISSUE SARCOMAS Please refer patients to your local Sarcoma Diagnostic Clinic if one or more of the following symptoms apply. There is a palpable lump that is ANY of the following: Greater than 5cm in diameter (a golf ball is about 4.2 cm) Yes /No Deep to fascia, fixed or immobile Yes /No /No Yes /No Increasing in size rapidly Yes Painful Clinical details regarding the suspicious lump (inc. location of lump): Patient with suspected recurrence after previous resection should be referred to the Sarcoma Treatment Centre via fax to 01792 703875 NB: Patients with the following should be referred to the more appropriate specialist team for an urgent outpatient appointment using the Urgent Suspected Cancer Referral (USCR) form for that speciality: Any patient with a neck lump that persists for more than three weeks to the local Head & Neck Team Any patient with generalised lymphadenopathy or neck lumps with a lymphocytosis to the local Haematology Team Details of ABMU Health Board Soft Tissue Sarcoma diagnostic Clinics Please either: Fax to 01792 703875 Or attach to generic e-referral template and send to Plastic Surgery in Morriston Hospital as an USC referral Is the patient aware of the reason & urgency for referral & aware that they will be offered an appointment within 10 working days? Yes /No Name of referrer (please print): Signature: Date: ……………….................................. Soft Tissue Sarcoma Referral Form October 2011 Page 1 of 1