Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacognosy wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Neuropharmacology wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Drug discovery wikipedia , lookup
Bevacizumab wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Discovery and development of tubulin inhibitors wikipedia , lookup
Linköping University Medical Dissertations No. 982
Pharmacogenetic studies of paclitaxel
in ovarian cancer
– focus on interindividual differences in
pharmacodynamics and
pharmacokinetics
Henrik Gréen
Division of Clinical Pharmacology
Department of Medicine and Care
Faculty of Health Sciences
Linköping University
SE-581 85 Linköping, SWEDEN
Linköping 2007
Cover:
Upper left – The author with his daughter Linnea reading Pharmacology by
Rang et al.
Upper right – Pacific yew tree, Taxus brevifolia
Lower left – The chemical structure of paclitaxel
Lower right – Woman with DNA spiral by Don Carroll, reprinted with
permission from Concept Images.
© Henrik Gréen, 2007
All rights reserved.
ISBN: 978-91-85715-84-8
ISSN: 0345-0082
Published articles have been reprinted with permission from the publishers:
Paper I © 2006 Elsevier, Cancer Letters.
Paper II © 2006 American Association of Cancer Research.
Paper III © 2006 John Wiley & Sons Limited.
Printed in Sweden by LTAB Linköpings Tryckeri AB, Sweden, 2007. 862.
To my family
Anna, Linnea & Julia
Mamma & Pappa
- Every active drug is a poison, when
taken in large enough doses; and in
some subjects a dose which is
innocuous to the majority of people has
toxic effects, whereas others show
exceptional tolerance of the same drug Sir Archibald E. Garrod (1858–1936)
- Alla är vi olika -
TABLE OF CONTENTS
ABSTRACT ..................................................................................................... 9
POPULÄRVETENSKAPLIG SAMMANFATTNING............................. 11
PAPERS IN THE PRESENT THESIS ....................................................... 13
ABBREVIATIONS ....................................................................................... 14
INTRODUCTION......................................................................................... 15
INDIVIDUALIZATION OF CANCER CHEMOTHERAPY ....................................... 15
GENETIC VARIATIONS IN DRUG METABOLIZING ENZYMES AND
TRANSPORTERS ........................................................................................ 17
PHENOTYPING AND GENOTYPING ................................................................. 19
PACLITAXEL ................................................................................................. 20
The Clinical Use of Paclitaxel and Ovarian Cancer................................................... 21
Paclitaxel Pharmacokinetics....................................................................................... 24
Metabolism of Paclitaxel............................................................................................ 24
Resistance to Paclitaxel.............................................................................................. 28
Decreased sensitivity to apoptosis-inducing stimuli ......................................................... 29
Tubulin Alterations ........................................................................................................... 29
P-glycoprotein and other drug transporters....................................................................... 30
AIMS OF THE THESIS............................................................................... 37
MATERIAL AND METHODS.................................................................... 39
PATIENTS...................................................................................................... 39
METHODOLOGICAL OVERVIEW .................................................................... 41
Single Strand Conformation Analysis........................................................................ 41
DNA-sequencing........................................................................................................ 42
Solid Phase Extraction ............................................................................................... 44
High Performance Liquid Chromatography............................................................... 45
UV detectors ..................................................................................................................... 46
Fluorescence detectors ...................................................................................................... 47
Mass spectrometry ..................................................................................................... 47
STATISTICS ................................................................................................... 50
RESULTS AND DISCUSSION ................................................................... 51
THE SCARCITY OF β-TUBULIN MUTATIONS IN OVARIAN TUMORS................ 51
ALLELE FREQUENCIES OF SNPS IN ABCB1, CYP2C8 AND CYP3A4 IN A
SWEDISH POPULATION AND IN OVARIAN CANCER PATIENTS ................... 52
CORRELATIONS OF ABCB1 GENOTYPES WITH THE RESPONSE TO
PACLITAXEL ............................................................................................. 54
QUANTIFICATION OF PACLITAXEL AND ITS HYDROXYMETABOLITES IN
HUMAN PLASMA ...................................................................................... 59
Extraction of paclitaxel from human plasma ............................................................. 59
Quantification of paclitaxel and metabolites using HPLC......................................... 60
Quantification of paclitaxel and metabolites using LC/MS....................................... 63
CORRELATIONS OF PACLITAXEL PHARMACOKINETICS TO ABCB1,
CYP2C8, CYP3A4 GENOTYPES AND CYP3A4 PHENOTYPE ................... 67
CORRELATIONS BETWEEN PACLITAXEL EXPOSURE, RESPONSE AND
GENOTYPES OF ABCB1, CYP2C8 AND CYP3A4.................................... 71
CONCLUSIONS............................................................................................ 75
FUTURE ASPECTS ..................................................................................... 77
ACKNOWLEDGEMENTS.......................................................................... 79
REFERENCES .............................................................................................. 82
ABSTRACT
Ovarian cancer is one of the most common female cancer diseases in the
world today and in Sweden more than 800 new cases are diagnosed every year.
The standard treatment consists of chemotherapy with paclitaxel in
combination with carboplatin after initial cytoreductive surgery. The response
to treatment and the severity of adverse drug reactions after chemotherapy
varies greatly among individuals, and one of the most important factors
responsible for these differences is now recognized to be the genetic
variability. One of the major obstacles to successful treatment is drug
resistance. Several potential mechanisms have been suggested for the
resistance to paclitaxel, such as mutations in the target protein β-tubulin,
single nucleotide polymorphisms (SNPs) in the gene ABCB1, which encodes
the transport protein P-glycoprotein. P-glycoprotein can mediate efflux of
various drugs from cancer cells as well as from the circulation into the
intestinal lumen, and overexpression and/or high activity leads to drug
resistance and/or increased elimination. Another reason might be the high
interindividual variability of paclitaxel plasma concentrations, which has been
suggested to be influenced by variability in metabolic enzymes, such as
CYP2C8 and CYP3A4, and transport proteins e.g. P-glycoprotein.
In the studies constituting this thesis we have investigated the possibilities
of predicting the pharmacokinetics of paclitaxel as well as the tumor response
and adverse drug reactions after chemotherapy in the preparation of
personalized chemotherapy. We studied the correlation between the response
and the presence of mutations in the dominant β-tubulin gene and SNPs in
ABCB1. DNA from 40 ovarian tumors was screened for sequence variations
in the β-tubulin gene without finding any, showing that β-tubulin mutations
are rare and unlikely to be a clinically relevant resistance mechanism for
paclitaxel. The SNPs G2677T/A and C3435T in the ABCB1 gene were
determined in 53 ovarian cancer tumors from patients with poor (progressive
disease or relapse within one year) or good (disease-free survival of more than
one year) response to paclitaxel-carboplatin chemotherapy. Patients
homozygously mutated for G2677T/A had a higher probability of responding
to chemotherapy. There was also a dose-dependent influence of the number
of mutated alleles on the response to paclitaxel treatment. No correlation was
found for the C3435T variant.
By using a newly developed quantitative LC/MS method for the
simultaneous determination of paclitaxel and its hydroxymetabolites in human
plasma we assessed the individual elimination of paclitaxel in 33 ovarian
cancer patients. The patients were genotyped for SNPs in the ABCB1,
CYP2C8 and CYP3A4 genes and their in vivo CYP3A4 enzyme activity, tumor
response and toxicity, especially the neurotoxicity, were determined. Patients
heterozygous for G/A in position 2677 in ABCB1 had a significantly higher
clearance of paclitaxel than patients with the wild type or homozygously
mutated, but not compared to patients carrying the G/T alleles. A lower
clearance of paclitaxel was also found for patients heterozygous for
CYP2C8*3 when stratified according to the ABCB1 G2677T/A genotype.
The CYP3A4 enzyme activity in vivo affected the relative influence of CYP2C8
and CYP3A4 on the metabolism, but not the total clearance of paclitaxel. The
exposure to paclitaxel was correlated to the neurotoxicity, but not to the
treatment response. In conclusion, our findings suggest that the SNP
G2677T/A in the ABCB1 gene, but not β-tubulin mutations, might be a
predictor for paclitaxel response and that the interindividual variability in
paclitaxel pharmacokinetics might be predicted by ABCB1 and CYP2C8
genotypes and provide useful information for individualized chemotherapy.
POPULÄRVETENSKAPLIG SAMMANFATTNING
Ovarialcancer (äggstockscancer) är en av de vanligaste cancerformerna hos
kvinnor i Sverige idag. Behandlingen består vanligen av tumörreducerande
kirurgi följd av kemoterapi med paklitaxel och karboplatin. Målsättningen med
detta avhandlingsarbete har varit att förbättra cytostatikabehandlingen
(cellgiftsbehandlingen) med framförallt paklitaxel vid ovarialcancer genom att
lägga grunden för individualisering av doser och förutsäga tumörsvaret vid
behandlingen. Ett problem med dagens cancerbehandling är att många
cancerceller så småningom blir resistenta mot olika cytostatika. För att angripa
den mest resistenta cellen innan den induceras att öka uttrycket av, eller
utveckla, fler resistensmekanismer vore det en fördel om vi före behandlingen
kunde prediktera vilken dos av cytostatika som är bäst lämpad för individen
samt om tumören kommer att reagera på behandlingen eller ej. En av de
viktigaste faktorerna för skillnader i behandlingseffekt tros vara genetiska
variationer mellan olika individer.
I våra studier har vi använt genetiska metoder för att studera om vi kan
prediktera tumörsvaret vid behandlingen genom att bestämma mutationer i
genen för paklitaxels målprotein, β-tubulin, samt bestämma genetiska
variationer i ABCB1-genen, kodande för transportproteinet P-glykoprotein.
Tanken är att ett förändrat målprotein eller en förändrad förmåga hos
cancercellerna eller kroppen att transportera ut paklitaxel skulle leda till en
skillnad i påverkan på tumören. DNA från 40 ovarialtumörer analyserades
utan att en enda sekvensvariation hittades i genen för β-tubulin, vilket tyder på
att genetiska förändringar i genen för β-tubulin sannolikt inte är en klinisk
relevant resistensmekanism. De normalt förekommande genetiska
variationerna G2677T/A och C3435T i ABCB1-genen bestämdes i DNA från
53 ovarialtumörer där behandlingen endera givit en bra (tumörfri minst ett år)
eller dålig (progression av tumören eller tumörfri mindre än ett år) antitumöreffekt. Patienter som var dubbelmuterade i position 2677 dvs hade
endera T/T eller T/A (A/A hittades inte i materialet) i denna position hade
en högre sannolikhet att få ett bra anti-tumörsvar vid behandlingen. Även
antalet muterade baser påverkade utfallet, ju fler muterade baser i position
2677, desto högre sannolikhet att få ett bra svar på behandlingen. Andelen T
eller A var också högre i den grupp av patienter som fått en lyckad
behandling.
För att kunna prediktera patientens individuella förmåga att bryta ner
paklitaxel studerade vi inverkan av sekvensvariationer i generna för de
nedbrytande enzymerna, CYP2C8 och CYP3A4, och transportproteinet Pglykoprotein (genen ABCB1) på eliminationen av läkemedlet i kroppen. Vi
utvecklade en metod för att mäta paklitaxelkoncentrationerna i blodet och
använde den för att studera hur snabbt 33 ovarialcancer patienter eliminerade
cytostatikat från blodbanan. Hos dessa patienter bestämde vi förekomsten av
kända genetiska variationer i generna ABCB1, CYP2C8 och CYP3A4 samt
deras CYP3A4 enzymaktivitet i kroppen. Biverkningarna och tumörsvaret vid
behandlingen utvärderades också. Eliminationen av paklitaxel hos dessa
patienter var beroende av vilken bas som fanns i position 2677 i ABCB1genen och förekomsten av den genetiska varianten CYP2C8*3.
Enzymaktiviteten hos CYP3A4 kunde inte påvisas påverka eliminationen av
paklitaxel utan snarare vilket enzym, CYP2C8 eller CYP3A4, som var relativt
dominant i respektive patient. Exponeringen av paklitaxel korrelerade till den
neurologiska påverkan som patienten orsakades av cytostatikat, men kunde
inte korreleras till tumörsvaret vid slutet av cytostatikabehandlingen.
Sammanfattningsvis ger patientens genetiska variationer i ABCB1, men inte
β-tubulin, information om behandlingsutfallet. Genetiska variationer i
CYP2C8 och ABCB1 påverkar patientens förmåga att eliminera paklitaxel och
kan förhoppningsvis användas för att individualisera doserna. Vår
förhoppning är att resultaten i denna avhandling skall kunna användas för att
individualisera och ytterligare förbättra cytostatikabehandlingen vid
ovarialcancer.
PAPERS IN THE PRESENT THESIS
This thesis is based on the following Papers, which will be referred to by their Roman
numerals:
I.
β-Tubulin Mutations in Ovarian Cancer Using Single Strand
Conformation Analysis – Risk of False Positive Results from
Paraffin Embedded Tissues.
Henrik Gréen, Per Rosenberg, Peter Söderkvist, György Horvath, and Curt
Peterson. Cancer Letters 236(1):148-154, 2006.
II.
mdr-1 Single Nucleotide Polymorphisms in Ovarian Cancer Tissue –
G2677T/A Correlates with Response to Paclitaxel Chemotherapy.
Henrik Gréen, Peter Söderkvist, Per Rosenberg, György Horvath, and Curt
Peterson. Clinical Cancer Research 12(3 Pt 1):854-859, 2006.
III.
Measurement of Paclitaxel and its Metabolites in Human Plasma
using Liquid Chromatography / Ion Trap Mass Spectrometry with a
Sonic Spray Ionization Interface.
Henrik Gréen, Karin Vretenbrant, Björn Norlander, and Curt Peterson.
Rapid Communications in Mass Spectrometry 20(14):2183-2189, 2006.
IV.
Pharmacogenetics of Paclitaxel in the Treatment of Ovarian Cancer
– a Pilot Study in Preparation of Individualized Chemotherapy.
Henrik Gréen, Peter Söderkvist, Per Rosenberg, Rajaa A. Mirghani, Per
Rymark, Elisabeth Åvall Lundqvist, and Curt Peterson. Submitted.
ABBREVIATIONS
The most important abbreviations used in
this thesis are listed below:
ABCB1
APCI
APS
ATP
AUC
bp
BSA
CI
CYP
dNTP
dHPLC
ESI
HPLC
LC/MS
mdr-1
MRP
NSCLC
OATP
PCR
P-gp
PPi
RFLP
RR
SNP
SSCA
SSI
TFA
or mdr-1, the gene encoding P-glycoprotein
Atmospheric pressure chemical ionization
Adenosine 5’ phosphosulfate
Adenosine triphosphate
Area under the concentration curve
Base pair
Body surface area
Confidence interval
Cytochrome P450
Deoxynucleotide triphosphate
Denaturing high performance liquid chromatography
Electrospray ionization
High performance liquid chromatography
Liquid chromatography / Mass spectrometry
or ABCB1, the gene encoding P-glycoprotein
Multi drug resistance protein
Non-small cell lung cancer
Organic anion transport protein
Polymerase chain reaction
P-glycoprotein
Pyrophosphate
Restriction fragment length polymorphism
Relative risk
Single nucleotide polymorphism
Single strand conformation analysis
Sonic spray ionization
Trifluoroacetic acid
INTRODUCTION
It is well known that most drug therapies are associated with significant
interindividual variability in their therapeutic effect and adverse drug
reactions. By far the most important factor responsible for these differences is
now recognized to be the genetic variability. Today there are numerous
examples of sequence variations in genes encoding drug-metabolizing
enzymes, drug transporters or drug targets known to affect the treatment
outcome. Although many non-genetic factors such as age, kidney and liver
functions, concomitant therapy, drug interactions, and the nature of the
disease influence the effects of medications, the list of genetic variants that
affect the patients’ response is continuously growing (Daly 2003; Eichelbaum
et al. 2006; Evans & McLeod 2003; Robert et al. 2005; Roses 2000).
Pharmacogenetics is the study of how genetic differences influence the
variability in patients’ responses to drugs (Roses 2000) and this thesis focuses
on the pharmacogenetics of paclitaxel and the methodology for studying
paclitaxel pharmacokinetics.
Individualization of Cancer Chemotherapy
Cancer chemotherapy has from its beginning in the 1940s, improved with
the introduction of new substances such as the anthracyclines in the 1960s,
the platinum complexes in the 1970s and the taxanes in the end of the 1980s.
Even more important, the use of existing agents has become more and more
INTRODUCTION | 15
efficient through the years. The treatment of cancer has gone from daily doses
to intermittent treatment in the 1950s, when Skipper et al. showed that normal
cells recover faster than cancer cells from cytotoxic drug exposure (Skipper et
al. 1964). Combination chemotherapy, where the principle idea is to combine
drugs with different mechanisms of action and dose-limiting toxicities, was
introduced in the 1960s and is still today the gold standard when treating
numerous types of cancer (Devita et al. 1970). A requirement for the
introduction of more effective cancer chemotherapy regimens has also been
improved supportive care such as the improvement of antibiotics, antiemetics,
supply of blood products etc. In later years the identification of disease
specific targets such as the Bcr-Abl tyrosine kinase in chronic myeloid
leukemia and the development of specific inhibitors like imatinib have been
shown to be successful (Druker 2002). However, at the same time as new
chemotherapeutic agents are developed today, it is equally important that
scientists try to improve the use of existing agents in the fight against cancer.
The aim of cancer chemotherapy is rather straightforward; to kill cancer
cells. However, there are relatively small differences between the normal cells
and the neoplastic cells, giving these drugs a narrow therapeutic index in
which the effective dose is not much different from a toxic dose in each
patient. Given the high variability in interindividual response and elimination
it is difficult to design a fixed dose suitable for all patients. A standard dose
can be effective in some patients and toxic in others, or even worse, toxic
without any tumor effect. The standard dosage used in chemotherapy today is
often based on the body surface area (BSA) of the patient, calculated from the
height and weight (Dubois & Dubois 1916). However, the variations in body
surface are far less than the variations in drug metabolizing enzymes, drug
transporters and the variability seen in pharmacokinetic parameters (Felici et
al. 2002).
One of the major causes of failure in chemotherapy in the clinical setting is
the development of drug resistance. Failure of a patient’s tumor to respond to
a specific therapy can be a result of several different mechanisms such as
inability to deliver the drug to the tumor site, low intracellular concentration
of the drug due to efflux pumps, rapid elimination of the drug from the
circulation, etc. (Gottesman 2002). Resistance is, however, a quantitative
problem and experimentally good dose-effect correlations have been shown in
16 | INTRODUCTION
vitro (Liliemark & Peterson 1991). A higher dose would therefore have a
higher probability of killing the most drug-resistant clone in the tumor mass.
The use of high-dose chemotherapy, often in combination with hematopoietic
rescue, has been studied showing an enhanced effect on the early remission of
the tumor but without a benefit on long-term survival (Nieboer et al. 2005;
Rodenhuis 2000). However, the results are from small studies on high risk or
relapsed patients, who have probably already developed resistance to the
chemotherapy. Recently scientists have tried to use dose-escalating regimens
where the dose gradually is increased from course to course as the progression
of side effects is monitored until the maximum tolerated dose is reached (with
an ´acceptable´ degree of toxicity). Unfortunately this is the same principle
used to induce drug resistance in cell lines in vitro and would therefore
probably result in a selection of drug-resistant cell clones. Our belief is that
higher doses, at least for some patients, should be used in the chemonaive
setting and would there probably have a higher impact on the overall survival.
We therefore postulate that the most important course of chemotherapy is
the first, before any exposure to the drug and any selection of drug-resistant
clones. It is highly desirable to a priori evaluate the patients’ predisposition for
toxicity, response and pharmacokinetics of the drug to be able to administer
the most suitable drug at the highest tolerable dose.
Genetic Variations in Drug Metabolizing Enzymes and
Transporters
A genetic polymorphism is defined as the occurrence in the same
population of a sequence variation of which at least two alleles exist at a high
frequency, conventionally above 1% (Lewin 1990; Meyer 2000). Most genetic
polymorphisms involve single base pair (bp) differences and are generally
referred to as single nucleotide polymorphisms, abbreviated SNPs (Kruglyak
& Nickerson 2001).
Genetic polymorphisms affecting pharmacotherapy were first discovered in
the 1950s due to incidental observations during World War II that some
patients or volunteers suffered unpleasant and disturbing adverse effects when
given standard doses of primaquine (Clayman et al. 1952; Hockwald et al. 1952;
Meyer 2000; Meyer 2004). It was later shown that the differences were due to
INTRODUCTION | 17
a genetically determined deficiency of glucose 6-phosphate dehydrogenase in
some individuals (Alving et al. 1956; Meyer 2000).
The sequencing of the human genome has allowed the identification of
thousands of SNPs (Venter et al. 2001), which can play an important role in
the expression level and activity of the corresponding proteins. When these
polymorphisms occur in genes encoding drug metabolizing enzymes or
transporters, it may change the disposition of the drug and, as a result, its
efficacy may be compromised or its toxicity altered. Polymorphisms can also
occur at the level of proteins directly involved in drug action, either when the
protein is the target of the drug or when the protein is involved in the repair
of drug-induced cell damage (Robert et al. 2005).
The largest group of drug metabolizing enzymes is the cytochrome P450s
(CYP), and all genes in the CYP families 1-3 are polymorphic. In the genes
encoding the CYPs, SNP frequencies differ between ethnic groups and the
functional importance of the various alleles also differs. In general, four
phenotypes can be identified: poor metabolizers lacking functional enzyme;
intermediate metabolizers, who are heterozygous for one deficient allele;
extensive metabolizers, who have two normal alleles; and ultrarapid
metabolizers, who have multiple gene copies. For one of the best described
genetic polymorphisms in a drug metabolizing enzyme, CYP2D6, the rate of
metabolism of a drug can differ 1000-fold between phenotypes (IngelmanSundberg 2004).
Transport proteins have an important role in the disposition of and
response to many drugs. Members of the adenosine triphosphate (ATP)binding cassette family (ABC) of membrane transporters are among the most
extensively studied (Brinkmann et al. 2001; Choudhuri & Klaassen 2006;
Evans & McLeod 2003; Marzolini et al. 2004). In the human ABC transport
family, 49 genes have been identified and divided into seven families
(Choudhuri & Klaassen 2006). A member of the ABCB family, P-glycoprotein
(P-gp), is encoded by the ABCB1 gene (also called mdr-1). The ABCB1 gene
contains several polymorphisms that have been shown to affect both the
expression of P-gp as well as the efflux of several drugs (Marzolini et al. 2004).
Genetic variations in genes encoding drug targets (i.e. receptors or cell
cycle proteins) can have a profound impact on drug efficacy and over 25
examples have already been identified. For example, sequence variations in the
18 | INTRODUCTION
gene for the β2-adrenoreceptor affects the response to β2-agonists and the
renoprotective action of angiotensin-converting enzyme inhibitors are
affected by SNPs in the gene for angiotensin-converting enzyme (Evans &
McLeod 2003).
Phenotyping and Genotyping
Most methods for determining a patient’s ability to metabolize or transport
a drug or predict its response utilize phenotyping and/or genotyping of the
involved mechanism (Daly 2004; Linder et al. 1997; Mathijssen & van Schaik
2006). Phenotyping usually involve either the direct measurement of the
enzyme activity in a tissue sample or the use of a probe drug (the metabolism
of which is solely dependent on a specific enzyme) and the subsequent
determination of the substance and metabolites in either plasma or urine for
assessment of the in vivo activity (Daly 2004). Genotyping is the determination
of specific genetic sequence variations, usually functionally important SNPs in
the gene encoding a specific protein (Linder et al. 1997). Phenotyping has the
advantage of the actual estimation of the enzyme activity and for some
methods the in vivo measurement and the overall process of the drug
metabolism. Phenotyping is mainly applicable to polymorphism affecting drug
disposition and not response. Other difficulties with phenotyping are the
usually complicated protocols, risk of adverse drug reactions, incorrect
assessment due to coadministration of drugs and drug-drug interactions (if
this is not what’s to be determined) and confounding effects of the disease
(Linder et al. 1997). Genotyping is now more widely used than phenotyping
and has the advantage that it only has to be performed once and requires a
small amount of DNA-containing material such as blood or saliva. However,
one should always consider the presence of unknown sequence variants that
can affect the activity. Most genotyping methods involve the amplification of
a specific gene segment using a polymerase chain reaction (PCR) with a
subsequent detection of the sequence variant by methods such as PCRrestriction fragment length polymorphism (PCR-RFLP) analysis or single
strand conformation analysis (SSCA) or more specialized and high-throughput
detection methods such as single bp extension, microarrays and
pyrosequencing (Daly 2004).
INTRODUCTION | 19
The method(s) of choice will depend on a number of factors such as the
specific drug studied, the enzyme(s) involved, number of samples, equipment
available, etc., and combining phenotyping and genotyping may be
appropriate for some drugs.
Paclitaxel
In the late 1950s the U.S. National Cancer Institute (NCI) initiated a
program to screen 35,000 plant species for anti-cancer activity. As part of this
program the U.S. Forest Service collected bark from the Pacific yew, Taxus
brevifolia, and shipped it to NCI. Extracts from the bark were found to have
anti-tumor activity and in 1971 the active ingredient was identified as
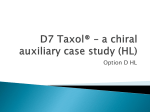
paclitaxel (Wani et al. 1971); Figure 1. When the NCI screening program was
closed in 1981 paclitaxel was the only compound left to be tested in humans
(Stephenson 2002).
Figure 1. The chemical structure of paclitaxel.
In 1979 Susan Horowitz identified paclitaxel’s unique mechanism of action.
Paclitaxel prevents cell division by promoting the assembly of stable
microtubules from α- and β-tubulin heterodimers and inhibiting their
depolymerisation (Schiff et al. 1979). This is an opposite effect to the vinca
alkaloids, which inhibit the polymerization of the microtubule (Rang et al.
1995). The microtubules are part of the cytoskeleton and are involved in
mitosis, cell shape determinations, cell locomotion and movement of
20 | INTRODUCTION
intracellular organelles (Alberts 1994). A typical microtubule lasts for about 10
minutes before it is disassembled and the proteins are used to build a new one
(Goodsell 2000). The cellular target for paclitaxel is β-tubulin (Manfredi et al.
1982) in the microtubule. Exposed cells are arrested in the G2/M-phase of the
cell cycle (Schiff & Horwitz 1980) and eventually the cells undergo apoptosis.
Mechanisms for paclitaxel-induced apoptosis, independent of microtubule
stabilization, have also been suggested, such as a direct phosphorylation of
bcl-2, induction of cytotoxic cytokines and pro-apoptotic proteins in a
concentration-dependent manner (Torres & Horwitz 1998; Wang et al. 2000).
However, the exact mechanisms for paclitaxel-induced cytotoxicity is still not
clear (Zhao et al. 2005).
In the mid-1980s paclitaxel was first tested on humans and the results of
the phase I trial were reported in 1987 (Wiernik et al. 1987). Acute
hypersensitivity reactions caused some delay in the trials, but they were later
attributed to the solvent Cremophor EL. In 1991 NCI started collaborating
with Bristol Myers Squibb for the development of the drug, marketed as
TaxolTM (Stephenson 2002). In 1996, a phase III study showed that survival
time for women with advanced ovarian cancer treated with the first line
paclitaxel-cisplatin combination was extended by 50% over the standard
cisplatin-cyclophosphamide treatment (McGuire et al. 1996). Shortly thereafter
paclitaxel in combination with cisplatin was introduced as the primary
treatment of carcinoma of the ovary in patients with advanced disease or
residual disease after initial surgery.
The Clinical Use of Paclitaxel and Ovarian Cancer
In Sweden today, paclitaxel is primarily used for the treatment of ovarian
cancer, breast cancer, non-small cell lung cancer (NSCLC) and AIDS-related
Kaposi's sarcoma (Läkemedelsindustriföreningen 2006). In this thesis we
focused on the treatment of ovarian cancer. Paclitaxel in combination with
carboplatin is today considered the standard chemotherapy of ovarian cancer
after cytoreductive surgery. Paclitaxel is used in standardized doses according
to body surface area (BSA) although this gives a high variability in drug
concentrations. Carboplatin on the other hand is almost entirely eliminated by
renal excretion and the myelosuppression is proportional to the exposure of
the drug. Therefore the dose of carboplatin is individualized according to
INTRODUCTION | 21
Calvert’s Formula
Carboplatin dose (mg) = AUC x (GFR+25 mL/min)
Calvert’s formula in which the dose depends on the glomerular filtration rate
(GFR) of the patient and the desired exposure of the drug expressed as area
under the concentration curve (AUC) (Alberts & Dorr 1998; Calvert et al.
1989). In Sweden, paclitaxel is usually given at a dose of 175 mg/m2 during a
three-hour infusion followed by a one-hour infusion of carboplatin aiming at
an AUC of 5 or 6 mg*min/mL administered every three weeks for a
minimum of six courses. For paclitaxel alternative infusion periods (1, 3 or 24
hours) and course intervals (every third week or weekly) are being considered,
and especially for patients with poor general conditions, the dose of paclitaxel
is usually reduced to 135 mg/m2. The weekly regimen, where paclitaxel usually
is given at a dose of 80 mg/m2 and carboplatin every third week has been
suggested as a more dose-dense alternative (Marchetti et al. 2002).
The incidence of ovarian cancer is among the highest in the world in North
America, Israel and Scandinavia (Parkin & International Agency for Research
on Cancer 2002). The age standardized incidence rate in Sweden 2004 was
16.6 annual cases per 100,000 females with a median age of diagnosis of 60-64
years (The National Board of Health and Welfare 2005). Ovarian cancer can
be divided into three broad subgroups – epithelial, stromal and germ cell
tumors – each with different clinical behavior. Epithelial ovarian cancer is the
most common, constituting more than 85% of the ovarian cancers (Agarwal
& Kaye 2003). Both the stromal and germ cell ovarian cancers consist of
diverse groups of diagnoses of which most are rare and with different
prognosis (Henriksson et al. 1998). The focus in this thesis will be on the
epithelial ovarian cancers. The epithelial ovarian tumors are characterized
according to FIGO stage (I-IV, subgroups A-C), histology and grade of
differentiation (well-, moderately- or poorly-differentiated). The FIGO staging
is based on findings at the surgery and describes the spread of the disease.
Stage I constitutes tumors localized to the ovaries, while stage II tumors have
spread to the surrounding tissue, stage III to the peritoneal cavity and stage IV
tumors have distant metastases. The tumors are subdivided into the following
histological types: serous, mucinous, clear cell, endometrioid, undifferentiated,
or adenocarcinoma (Heintz et al. 2003). One of the most important prognostic
22 | INTRODUCTION
factors in the treatment of ovarian cancer is the extent to which the initial
surgery reduces the tumor mass. Median survival for patients where the
remaining tumor is larger than 2 cm is 12-16 months as compared to 40-45
months if the tumor is reduced below 2 cm (Mutch 2002). Other important
prognostic factors are FIGO stage (see Table I) and histology where
endometrioid and mucinous histotypes have a better prognosis, whereas
serous and undifferentiated cancers have a worse prognosis (Heintz et al.
2003). However, progression-free survival and overall survival are improved
in all patients by chemotherapy after initial surgery (Agarwal & Kaye 2003).
Table I. Five-year survival and complete
response by FIGO stage.
Complete
5-year
FIGO stage
response
survival
I
94,8 %
82.3 %
II
82,7 %
69.2 %
III
51,7 %
31.6 %
IV
23,5 %
13.4 %
Note: Patients treated in 1996-1998. FIGO Annual
report (Heintz et al. 2003)
First-line chemotherapy with paclitaxel-carboplatin combination given
every three weeks for six courses yields response in about 80% of ovarian
cancer patients (Bolis et al. 2004). However, the median progression-free
survival is only 15 months in these patients, since most relapse (Vasey et al.
2004). Interestingly, these patients can be re-treated with the same drugs
(paclitaxel-carboplatin) with response rates that are proportional to the
treatment-free interval. Patients who have a treatment-free interval of two
years will have a complete response rate of ~75%, but this falls to 35% for a
treatment-free interval of six to nine months (Gronlund et al. 2001). This
reduced response rate is due to the development of drug resistance and
patients with a progression free interval less than six months is determined
clinically drug resistant. This results in a five-year survival of only 35% in
relapsed patients with advanced ovarian cancer (Goldspiel 1997), despite the
fact that most tumors are chemosensitive during the first-line treatment.
INTRODUCTION | 23
Paclitaxel Pharmacokinetics
Paclitaxel is insoluble in aqueous solution and is therefore formulated in
50% ethanol and 50% Cremophore EL (a polyoxyethylated castor oil
derivative). Approximately 95% of the substance is bound to plasma protein
and the volume of distribution is about 55 L/m2 (Wiernik et al. 1987). After a
3-hour infusion the plasma concentration of paclitaxel is decreased in a
triexponential fashion. The initial phase has a t½ of 10–30 minutes, the second
phase has a t½ of about 1–4 hours and the final elimination t½ is about 8-34
hours (Huizing et al. 1995b). No significant change in pharmacokinetics has
been observed between different courses (Huizing et al. 1997a; Huizing et al.
1997b). For a 3-hour infusion of 175 mg/m2 the AUC ranges from 6 – 30
µmol*h/L and a clearance of 15–36 L/h (Gianni et al. 1995; Huizing et al.
1997a; Huizing et al. 1993; Huizing et al. 1997b; Nakajima et al. 2005; Nakajima
et al. 2006). The pharmacokinetics is nonlinear with a disproportional increase
in AUC and Cmax with an increase in dose (Gianni et al. 1995; Huizing et al.
1997a). The nonlinear pharmacokinetics of paclitaxel has been ascribed to a
saturable elimination (transport) (Sonnichsen et al. 1994) and/or a saturable
distribution (binding) (Karlsson et al. 1999), but also as caused by the micelle
forming vehicle Cremophor El (Sparreboom et al. 1999).
Several pharmacokinetic parameters have been shown to be correlated with
the effect of paclitaxel. Higher plasma concentration and especially the
duration of paclitaxel concentrations above a threshold correlates with the
response to chemotherapy (Huizing et al. 1997a; Huizing et al. 1993; Mielke et
al. 2005a) as well as with the toxicity (Gianni et al. 1995; Huizing et al. 1993;
Mielke et al. 2005b).
Metabolism of Paclitaxel
Paclitaxel is primarily eliminated through hepatic metabolism and biliary
clearance. In the liver paclitaxel is metabolized by two CYP-enzymes. The
formation of 6α-hydroxypaclitaxel is catalyzed by CYP2C8 (Cresteil et al. 1994;
Rahman et al. 1994) and p-3’-hydroxypaclitaxel is formed by CYP3A4 (Cresteil
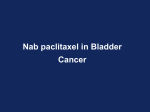
et al. 1994; Harris et al. 1994b). Both metabolites can be further oxidized to 6α, p-3’-dihydroxypaclitaxel by CYP2C8 and CYP3A4, respectively (Sonnichsen
et al. 1995); see Figure 2. The metabolites are less cytotoxic and present in
plasma in lower concentrations than paclitaxel and therefore believed to have
24 | INTRODUCTION
no significant clinical effect on the tumors (Harris et al. 1994a; Kumar et al.
1995; Monsarrat et al. 1993; Sparreboom et al. 1995a). The major part of both
paclitaxel and the metabolites are excreted in the feces, indicating extensive
biliary clearance (Monsarrat et al. 1993; Monsarrat et al. 1998). Total urinary
excretion is ~ 5% and in most patients the fecal excretion is ~ 80% of the
dose (Rowinsky et al. 1990; Walle et al. 1995). The major part of the dose is
excreted as metabolites indicating that CYP2C8 and CYP3A4 are important in
the elimination of paclitaxel. In bile from patients treated with paclitaxel the
most abundant metabolites are 6α-, p-3’-dihydroxypaclitaxel and 6αhydroxypaclitaxel. Paclitaxel and p-3’-hydroxypaclitaxel have also been found
but at a much lower concentration (Harris et al. 1994a; Monsarrat et al. 1993;
Monsarrat et al. 1998).
Paclitaxel
CYP2C8
CYP3A4
6α-hydroxypaclitaxel
p-3’-hydroxypaclitaxel
CYP3A4
CYP2C8
6α-, p-3’-dihydroxypaclitaxel
Figure 2. The metabolism of paclitaxel by CYP2C8 and CYP3A4 in the liver.
CYP2C8 is a major human hepatic P450 enzyme, constituting about 7% of
the total microsomal CYP content in the liver (Totah & Rettie 2005).
Extrahepatic expression of CYP2C8 mRNA has also been detected in the
kidney, intestine, brain, mammory glands, ovaries as well as the adrenal glands
(Klose et al. 1999). Substrates for CYP2C8 include both endogenous
substances such as arachidonic acid and retinoic acid as well as therapeutic
agents, e.g. paclitaxel, ibuprofen, repaglinide, cervastatin and amodiaquine
(Totah & Rettie 2005). The gene for CYP2C8 is located on chromosome
10q24 and consists of 9 exons (Klose et al. 1999). Several SNPs have been
identified in both coding and non-coding regions, some of which correspond
to proteins with reduced enzymatic activity; see Table II (Bahadur et al. 2002;
Dai et al. 2001; Hichiya et al. 2005; Soyama et al. 2002b). CYP2C8*3, expressed
most commonly in Caucasian populations, has a dual amino acid change
INTRODUCTION | 25
Arg139Lys and Lys399Arg (Dai et al. 2001). In vitro the CYP2C8*3 allele has
shown decreased Vmax (Soyama et al. 2001) and activity (Dai et al. 2001) for the
conversion of paclitaxel to 6α-hydroxypaclitaxel but maintains the catalytic
activity towards amiodarone (Soyama et al. 2002a) as compared to the wild
type. Liver microsomes from individuals heterozygous for CYP2C8*3 also
had lower activity as compared to the wild type (Bahadur et al. 2002), although
the activity did overlap and the results could not be reproduced in a smaller
study (Taniguchi et al. 2005). CYP2C8*3 also has a reduced turnover for
arachidonic acid in vitro but CYP2C8*2 which has a reduced paclitaxel activity,
did not (Dai et al. 2001). Both these findings indicate that CYP2C8 exhibits
ligand-dependent polymorphisms probably due to unique binding sites for
different substrates (Totah & Rettie 2005). Altered drug metabolism for
CYP2C8*3 has also been shown in vivo for ibuprofen and repaglinide (GarciaMartin et al. 2004; Niemi et al. 2003).
Table II. CYP2C8 allele nomenclature and altered activity.
Allele
CYP2C8*1B
CYP2C8*1C
CYP2C8*2
CYP2C8*3
CYP2C8*4
CYP2C8*5
CYP2C8*6
CYP2C8*7
CYP2C8*8
CYP2C8*9
CYP2C8*10
CYP2C8 P404A
Nucleotide
change
C-271A
C-370A
A805T
G416A, A1196G
C792G
475 Del A
G511A
C556T
C556G
A740G
G1149T
C1210G
Amino acid
change
I269F
R139K, K399R
I264M
Frame shift
G171S
R186X
R186G
K247R
K383N
P404A
Enzyme
activity 1
Increased Km
Decreased activity
None
None
Decreased
Note: 1 Altered activity for at least one substrate in vivo or in vitro.
In most people, CYP3A4 is the most highly expressed CYP enzyme in the
liver although the interindividual protein expression varies as much as 40-fold
(Lamba et al. 2002; Smith et al. 1998). The enzyme is also expressed in the
lungs, stomach, small intestine, nasal mucosa and colon, of which the
expression in the small intestine is believed to be the most important
extrahepatic expression for drug metabolism (Ding & Kaminsky 2003).
CYP3A4 is involved in conversion of the majority of drugs with known
metabolic pathways. The CYP3A4 activity can be inhibited by e.g. grapefruit
26 | INTRODUCTION
juice or ketoconazole and induced by substances such as barbiturates and St
John’s wort (Whitten et al. 2006). The reason for the CYP3A4 metabolic
versatility is believed to be due to a large active site that permits the binding of
structurally diverse molecules. The enzyme is also known to accommodate
several ligands simultaneously in the active site which may result in enhanced
activity or reduced product formation, depending on the concentration of the
substrate and the nature of the second or third ligand (Anzenbacher &
Anzenbacherova 2001; Lamba et al. 2002). Genetic variability has been
established in the CYP3A4 gene. However, due to the low frequencies and
limited effect of these SNPs on the enzyme expression and catalytic function,
the genetic variations are unlikely to be the major cause of interindividual
differences in CYP3A4 activity (Lamba et al. 2002; Rodriguez-Antona &
Ingelman-Sundberg 2006). The most common allelic variant CYP3A4*1B, A392G in the flanking region (located in the nifedipine response element and
present at ~5% in Caucasians), has been shown to affect the activity and
correlates to lower hydroxylation of quinine and less binding of nuclear
proteins (Lamba et al. 2002; Rodriguez-Antona & Ingelman-Sundberg 2006).
Although several other alleles have been reported, the responsibility of a
particular allele(s) for the variable activity has not yet been established
(Anzenbacher & Anzenbacherova 2001). Due to the inability to determine
the CYP3A4 activity by genotyping, several probes have been proposed for
measurement of CYP3A4 activity in vivo (Kivisto & Kroemer 1997; Masica et
al. 2004; Smith et al. 1998). Classically the erythromycin breath test,
endogenous/exogenous cortisol hydroxylation and midazolam clearance have
been used to assess CYP3A4 activity in vivo. More recently alprazolam,
triazolam and quinine have been validated as CYP3A4 probes (Anzenbacher
& Anzenbacherova 2001; Masica et al. 2004; Mirghani et al. 2003; Smith et al.
1998). Some probes do correlate with each other although for some
comparisons there is only a weak correlation (Kenworthy et al. 1999; Kinirons
et al. 1999; Lown et al. 1995; Masica et al. 2004). Noteworthy is that midazolam
and erythromycin appear to bind to different domains within the active site
and that the CYP3A4 catalyses different types of reactions such as Ndemethylation of erythromycin and the hydroxylation of midazolam and
quinine (Kenworthy et al. 1999; Smith et al. 1998). With respect to anticancer
treatment, the CYP3A4 activity is expected to influence the response to
INTRODUCTION | 27
several drugs such as paclitaxel, docetaxel and imatinib (Green et al. 2006;
Rodriguez-Antona & Ingelman-Sundberg 2006). Docetaxel (an analog to
paclitaxel preferably used in the treatment of breast cancer) is metabolized to
an inactive hydroxymetabolite by CYP3A4. The clearance of docetaxel can be
predicted by CYP3A4 activity measured by the erythromycin breath test and
midazolam clearance and the greatest toxicity was found in patients with the
lowest enzyme activity (Goh et al. 2002; Hirth et al. 2000). Similarly, Yamaoto
et al. individualized docetaxel doses based on CYP3A4 activity measured by
urinary cortisol metabolite concentrations after administration of cortisol and
thereby decreased the pharmacokinetic variability of docetaxel when
compared to BSA-based dosing (Yamamoto et al. 2005).
If and to what extent interindividual variations in enzymatic activity of
CYP2C8 and CYP3A4 are influencing the pharmacokinetics of paclitaxel has
not yet been fully revealed.
Resistance to Paclitaxel
Drug resistance is a major obstacle to successful treatment of cancer
patients and is believed to cause treatment failure and death in more than 90%
of ovarian cancer patients with metastatic disease (Agarwal & Kaye 2003).
Several potential mechanisms have been reported to account for cellular
resistance to paclitaxel including decreased tubulin binding due to sequence
variation (Monzo et al. 2002), alterations in microtubule dynamics (Orr et al.
2003), decreased sensitivity to apoptosis-inducing stimuli (Blagosklonny &
Fojo 1999), and overexpression of the transport protein P-glycoprotein
(Gottesman 2002). Non-cellular mechanism for failure to response can
broadly be divided into two groups: pharmacokinetics and tumor microenvironment. Experimental studies show that, for many cytotoxic agents, the
number of cancer cells killed is proportional to the drug exposure. Inadequate
intratumor drug concentrations due to interindividual differences in
pharmacokinetic variables might therefore explain some cases of lack of
response. These factors include difference in renal clearance (as with
carboplatin), hepatic drug metabolism (CYP2C8 and CYP3A4 for paclitaxel)
and tumor vascularity (Agarwal & Kaye 2003; Iyer & Ratain 1998). The tumor
micro-environment can also affect the tumor response. Hypoxia has been
suggested to be associated with radiosensitivity as well as chemosensitivity,
28 | INTRODUCTION
and cell-cell interaction in vitro has also been shown to correlate to
chemosensitivity (Agarwal & Kaye 2003). This might be due to reduced
proliferation during hypoxia, diminished free-radical production, enhanced
drug detoxification and/or hypoxia-induced factor-1 mediated induction of
survival factors and inhibition of apoptosis (Teicher 1994).
Decreased sensitivity to apoptosis-inducing stimuli
A number of proteins involved in the apoptotic signaling pathways and
pathways downstream of drug-target have been suggested to affect the
resistance to paclitaxel. These include oncogenes such as Ras and Akt, tumorsuppressor genes such as p53 and Pten, whereas others are components of the
apoptotic mechanism such as survivin, Bak and Bcl-2 (Agarwal & Kaye 2003).
Up-regulation of anti-apoptotic Bcl-2 and down-regulation pro-apoptotic
proteins such as Bak have been shown to affect paclitaxel sensitivity in vitro
(Ferlini et al. 2003; Jones et al. 1998; Mano et al. 1999). However, in vivo the
correlation is not obvious and the paclitaxel sensitivity has been shown to be
independent of Bcl-2 and a high as well as a low expression of Bcl-2 has been
found to be a good prognostic factor (Marx et al. 1997; Poelman et al. 2000).
Their exact role in clinical paclitaxel resistance therefore remains to be
defined.
Tubulin Alterations
Tubulin alterations such as changes in tubulin expression and mutations in
the tubulin genes have been suggested as a resistance mechanism for paclitaxel
(Orr et al. 2003). However, the significance of these alterations has yet not
been established mainly due to the existence of several tubulin isoforms,
encoded by a large gene family consisting of both functional and nonfunctional genes with high homology. In humans, six different β-tubulin
isoforms have been identified and are classified as follows (Roman numerals
represent the protein class and Arabic numerals the gene): class I, M40; class
II, β9; class III, β4; class IVa, 5β; class IVb, β2; class VI, β1. The M40 gene
has four exons and encodes a protein, 444 amino acids long. The other
isotypes show similar sequences, but specific regions of variability beyond
amino acid 430 can be used to group the isotypes. The expression of these
isoforms is tissue-dependent, but classes I and IVb are ubiquitously expressed
and class I (gene M40) constitutes the major fraction of the β-tubulin
INTRODUCTION | 29
isoforms (Sullivan & Cleveland 1986). A higher expression of different βtubulin isoforms, mainly classes III and IVa, have been found in paclitaxelresistant cell lines as compared to the parental cell line (Kavallaris et al. 1997;
Nicoletti et al.; Orr et al. 2003). In clinical samples, class III overexpression has
been associated with poor response to chemotherapy although conflicting
results have been published (Ferrandina et al. 2006; Mozzetti et al. 2005;
Nicoletti et al. 2001). Mutations in the β-tubulin genes, especially gene M40,
resulting in tubulin units with different affinity for paclitaxel have also been
suggested as a resistance mechanism. In resistant cell lines, point mutations
have been found at several locations in the β-tubulin gene M40 as well as in
Kα1-tubulin (Giannakakou et al. 2000; Giannakakou et al. 1997; GonzalezGaray et al. 1999; Martello et al. 2003). Several research groups have studied
the presence of tubulin mutations in clinical samples. Monzo et al. (1999)
identified β-tubulin mutations in 33% of patients with non-small-cell lung
cancer, which correlated to poor response to paclitaxel containing therapy
(Monzo et al. 1999). Many groups have attempted to confirm this initial study;
but conflicting results have been reported (Kelley et al. 2001; Kohonen-Corish
et al. 2002; Sale et al. 2002b; Tsurutani et al. 2002). The homology of the
tubulin genes and the questioned accuracy of the original gene sequence for βtubulin M40 (J00314) have made it difficult to draw any decisive conclusions
(Kelley 2002; Monzo et al. 2002; Sale et al. 2002a).
P-glycoprotein and other drug transporters
Alterations in drug influx and efflux due to cell membrane transport
proteins such as P-glycoprotein (P-gp), multidrug resistance protein (MRP),
organic anion transporters (OATP) 1B1 and 1B3 can affect intracellular drug
concentrations and might have an effect on the chemosensitivty to paclitaxel
(see Figure 3).
The uptake of paclitaxel into the cells has been suggested to be either a
diffusion process or mediated by OATP1B1 or OATP1B3, which mediate the
cellular uptake of a large number of structurally diverse endogenous
substances and xenobiotics (Tirona & Kim 2002). The expression of these
transporters is restricted to the basolateral membrane of the hepatocytes.
However, the expression in the ovaries has not been investigated (Konig et al.
2000a; Konig et al. 2000b). OATP1B3 has been shown to mediate the influx
30 | INTRODUCTION
of paclitaxel and suggested to be the a key regulator for hepatic uptake of
paclitaxel (Smith et al. 2005). The gene encoding OATP1B3 (SLCO1B3)
contains several SNPs which affect the transport function of the protein
(Letschert et al. 2004; Tirona & Kim 2002). The effect of these SNPs on the
clearance of paclitaxel remains unclear.
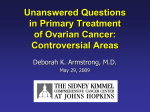
Figure 3. Schematic representation of the transport and metabolism of paclitaxel in the
hepatocyte. The OATP located on the basolateral membrane of the hepatocyte facilitate
the uptake of paclitaxel from the portal circulation. Paclitaxel is metabolized by CYP2C8
and CYP3A4 in the hepatocyte. P-gp mediates the canalicular efflux of paclitaxel and
metabolites from the hepatocytes into the bile.
P-gp is a 170 kDa transport protein encoded by the ABCB1 gene (mdr-1)
and contains 1280 amino acids constituting 12 transmembrane domains and 2
ATP-binding motifs (Figure 5). Cytotoxic drugs of natural origin with very
different chemical structures and mechanisms of action, such as vinca
alkaloids, anthracyclines, epipodophyllotoxins, docetaxel and paclitaxel, can be
extruded by P-gp through the cell membranes of resistant cells and crossresistance occurs (Germann 1996; Gottesman & Pastan 1993). Variable levels
of P-gp have been observed in different multidrug resistant cell lines and an
increased expression of P-gp generally correlates with an increase of drug
resistance (Fujimaki et al. 2002). However, the opposite might not be true due
to the presence of other resistance factors (Sonneveld 2000).
P-gp is also expressed in non-malignant tissue and found in the canalicular
surface of the hepatocytes, the apical surface of proximal tubular cells in the
kidneys, and the brush border surface of enterocytes (Thiebaut et al. 1987).
The localization of P-gp to the liver, kidneys and intestine makes it a major
determinant for absorption, hepatic and renal elimination of several drugs. In
INTRODUCTION | 31
P-gp
P-gp
P-gp
P-gp
Figure 4. Schematic representation of the transport of paclitaxel by P-glycoprotein.
Elimination of paclitaxel from the liver to the bile, from the central nervous system and from
the ovaries as well as the reduced reabsorption of paclitaxel in the small intestine is
believed to be associated with P-gp transport.
addition, P-gp is expressed in the epithelium of the brain choroid plexus (the
blood-cerebrospinal fluid barrier) and on the luminal surface of blood
capillaries of the brain (the blood-brain barrier) as well as other tissues with
blood-tissue barriers such as the placenta, the ovaries, and the testis (Thiebaut
et al. 1987) making it an important protein for the protection of xenobiotic
sensitive organs.
Paclitaxel is a P-gp substrate and the transport function might affect
paclitaxel pharmacokinetics and pharmacodynamics in several ways; see
Figure 4. Overexpression of P-gp on tumor cells resulting in an enhanced
efflux of the drug is a known in vitro resistance mechanism for paclitaxel
(Germann 1996; Gottesman & Pastan 1993). Paclitaxel can also be
transported by the efflux protein MRP-7 but none of the other MRPs has
been shown to transport paclitaxel in vitro (Allen et al. 2000; Hopper-Borge et
al. 2004). Also the basal expression of P-gp has been shown to be important
32 | INTRODUCTION
for the sensitivity to paclitaxel in vitro, and at high drug concentrations the
transport of paclitaxel by P-gp has been shown to be saturable (Allen et al.
2000; Jang et al. 2001). Clinical resistance and poor response to paclitaxel have
also been correlated with a high expression of P-gp in tumors (Kamazawa et
al. 2002; Penson et al. 2004; Yeh et al. 2003) indicating an importance of the
protein in the in vivo environment. P-gp also affects the pharmacokinetics of
paclitaxel. Co-administering a P-gp inhibitor during paclitaxel treatment
results in a decreased clearance of paclitaxel and marked increase in paclitaxel
exposure (Berg et al. 1995). Studies in mice have also shown that P-gp limits
the oral uptake of paclitaxel and that P-gp mediates the direct excretion of the
drug from the systemic circulation via the hepatocytes and bile into the
intestinal lumen as well as the absorption (or re-absorption) of paclitaxel in
the intestine (Sparreboom et al. 1997; van Asperen et al. 1998). Figure 3
illustrates the transport and metabolism of paclitaxel in the hepatocytes.
Paclitaxel penetrates to the cerebrospinal fluid although at very low
concentrations (Gelderblom et al. 2003). The net penetration is dependent on
the P-gp efflux and blocking the transport significantly increases the
concentrations of paclitaxel in the central nervous system (Fellner et al. 2002;
Kemper et al. 2003). In knockout mice (mdr1ab -/-) the penetration of
paclitaxel to the central nervous system increases even further (Kemper et al.
2003). However, the importance of P-gp function for the neurotoxicity and
the anti-neoplastic effect on brain tumor of paclitaxel remains unclear.
In the late 1980s the first study of the effect and presence of SNPs in the
ABCB1 gene (Figure 5) was presented and some sequence variants showed an
altered resistance phenotype (Kioka et al. 1989). However, it was not until
2000 when Hoffmeyer et al. systematically screened the mdr-1 gene for
sequence variations that the functional consequence of the SNPs were shown
in vivo. This study indicated that the synonymous SNP in exon 26, C3435T,
correlated with the expression level of P-gp in the intestine. Individuals
homozygous for this SNP had lower P-gp expression and showed higher
plasma levels of the P-gp substrate digoxin (Hoffmeyer et al. 2000). The
C3435T SNP affects the mRNA stability and the 3435T allele is correlated to
a lower expression (Wang et al. 2005a). More than 25 SNPs have been
reported for the ABCB1 gene of which more than 20 are in the coding region
(Marzolini et al. 2004; Pauli-Magnus & Kroetz 2004; Sakaeda et al. 2002).
INTRODUCTION | 33
Figure 5. Secondary structure of P-glycoprotein with coding region SNPs (with an allele
frequency of more than 1% in Caucasions). Non-synonymous amino acid changes are
shown as filled balls with the indicated amino acid change and position. Synonymous
changes are shown as encircled balls with the indicated nucleotide change and position in
the mRNA. The ATP binding domains are indicated by the two boxes.
However, most SNPs are present at very low frequencies and there are large
interethnic variations (Marzolini et al. 2004). In Caucasians the SNPs C1236T,
G2677T/A (Ala893Ser/Thr) and C3435T have been studied most frequently
since they have been shown to correlate with the P-gp expression and
phenotype (Hoffmeyer et al. 2000; Tanabe et al. 2001). These three SNPs are
also linked to each other and the effect of one SNP might be difficult to
distinguish from the others (Kroetz et al. 2003). A total of 64 haplotypes have
been described and the two most common are the wild type allele (15% in
Caucasians) and ABCB1*13 containing six sequence variants, three intronic
1236T, 2677T and 3435T (32% in Caucasians) (Kroetz et al. 2003). How these
SNPs affect the transport function of P-gp has not been studied extensively in
vitro (Kim et al. 2001; Kimchi-Sarfaty et al. 2002; Kroetz et al. 2003; Morita et al.
34 | INTRODUCTION
2003). Kimchi-Sarfaty et al. (2002) showed that the wild type P-gp causes a
slightly higher efflux of paclitaxel than cells carrying a plasmid containing the
2677T variant (Kimchi-Sarfaty et al. 2002). However, for most other substrates
such as verapamil, vinblastine, calcein-AM, prazosin, bisantrene, forskolin,
digoxin (0.1 μM) and cyclosporin A the transport was not affected, but only
one concentration was tested for each substrate (Kimchi-Sarfaty et al. 2002;
Kroetz et al. 2003; Morita et al. 2003). Unexpectedly an enhanced efflux has
been reported for digoxin in a very high concentration (50 μM) in cells
expressing the P-gp Ser893 variant (2677T), indicating differences in substrate
specificity for the different variants of P-gp (Kim et al. 2001). For paclitaxel
the SNP G1199T/A (Ser400Ile/Asn) has been shown to affect the sensitivity
of cells expressing the variants. Cells expressing the 1199A variant were more
resistant to paclitaxel than wild type cells, while cells with the 1199T variant
were more sensitive to paclitaxel. The SNP also affected the resistance to
vinblastine, vincristine and doxorubicin, but not topotecan in the same way
(Crouthamel et al. 2006). However, the effect of these SNPs on the response
to paclitaxel and the pharmacokinetics of paclitaxel were not known when this
thesis was initiated.
INTRODUCTION | 35
36 | INTRODUCTION
AIMS OF THE THESIS
The general aim of this thesis was to study the pharmacogenetics of
paclitaxel in preparation for personalized chemotherapy.
Specific aims:
1. To investigate the presence of mutations in the β-tubulin gene M40, as a
potential resistance mechanism, and its correlation to the clinical outcome
of ovarian cancer patients treated with paclitaxel in combination with
carboplatin
2. To evaluate the effects of the single nucleotide polymorphisms G2677T/A
and C3435T in the ABCB1/mdr-1 gene on the response to paclitaxel
treatment in ovarian cancer and establish the allele frequencies of these
SNPs in a Swedish population
3. To develop a method for quantification of paclitaxel and its metabolites in
human plasma
4. To evaluate the effects of sequence variations in the CYP2C8, ABCB1, and
CYP3A4 genes and the CYP3A4 phenotype on the pharmacokinetics of
AIMS OF THE THESIS |37
paclitaxel as well as the toxicity and anti-tumor response during treatment
with paclitaxel in combination with carboplatin
38 | AIMS OF THE THESIS
MATERIAL AND METHODS
Patients
The patients in the present investigation were diagnosed with gynecological
cancer, predominantly epithelial ovarian cancer. A summary of the subjects
and their diagnoses included in the individual papers are presented in Table
III.
Table III. Diagnoses of the patients included.
Paper
I
II
IV
Epithelial
Ovarian
Cancer
40
51
26
Fallopian
Tube
Carcinoma
2
Peritoneal
Cancer
4
Corpus
Uteri
Carcinoma
1
Cervix
Uteri
Carcinoma
1
Ovarian or
Peritoneal
Cancer
1
Total
40
53
33
In Paper I, epithelial ovarian cancer patients were selected from four
patient groups based on their received chemotherapy and the therapeutic
effect. The patients in the first group had been treated with paclitaxel in
combination with carboplatin and achieved a complete response and were
tumor free for at least 18 months. The second group was treated with the
same regimen but had tumor progression during treatment or a relapse within
nine months. The other two groups had the same clinical outcomes as the two
first groups but were treated with non-tubulin affecting chemotherapy. In
MATERIAL AND METHODS | 39
Paper II, a total of 53 patients were included from a biobank at Sahlgrenska
University Hospital, Gothenburg or from the Linköping University Hospital.
Fifty-one were diagnosed with epithelial ovarian cancer and two had fallopian
tube carcinoma; both diagnoses were expected to have the same clinical
response and exclusion of the latter two did not affect the results presented.
In Papers II and IV the patients were treated with paclitaxel 175 mg/m2 in
combination with carboplatin except for a few patients with general poor
condition where the paclitaxel dose was reduced to 135 mg/m2. In Paper IV
the patients were mainly diagnosed with either ovarian cancer or peritoneal
cancer. In rare cases, cancer arises in the peritoneum – the inner lining of the
abdominal cavity. Peritoneal cancer is believed to be very similar to ovarian
cancer both in clinical behaviour, response to treatment and biology. These
patients were therefore included in the same group as the ovarian cancer
patients. Two patients with other diagnoses were included in Paper IV. In this
study the pharmacokinetics was the main objective and as long as the patients
had a gynecological cancer, the diagnosis was not expected to affect the
pharmacokinetics. However, these two patients were excluded from the tumor
response evaluation.
To determine the allele frequencies of investigated SNPs in a reference
population, DNA samples from a regional biobank were used (Paper II and
IV). The biobank consists of DNA from 800 individuals, of which we used
200, living in the southeast region of Sweden (50% males and 50% females).
The individuals had been randomly selected from the Swedish population
register and after informed consent anonymously included in the biobank.
The relationship between the allele frequencies in the reference population
and in the ovarian cancer patients were investigated to determine if the SNPs
in some way correlated to ovarian carcinogenesis.
The regional ethics committee in Linköping approved all the studies
including patient material and written informed consent was obtained from
each patient in Paper IV.
40 | MATERIAL AND METHODS
Methodological Overview
In this section only a brief summary and the principal aspects of the
methods used in this thesis will be presented (Table IV). The details of the
methods are given in the individual Papers.
Table IV. Methods used in this thesis.
Methodology
Single Strand Confirmation Analysis
DNA sequencing
Solid Phase Extraction (SPE)
High Performance Liquid Chromatography (HPLC)
Mass spectrometry
Papers
I
I, II and IV
III and IV
III and IV
III and IV
Single Strand Conformation Analysis
In Paper I, Single Strand Conformation Analysis (SSCA) was used to screen
the β-tubulin gene M40 for mutations. The investigation of unknown
sequence variations in biological samples is a powerful method for the
discovery of individual differences in biological pathways associated with
disease and/or altered drug response. For a long time, manual direct
sequencing was the only available method for detection of genetic variations.
Therefore several methods such as SSCA, denaturating gradient gel
electrophoresis and denaturating High-Performance Liquid Chromatography
(dHPLC) were developed for detection of whether or not a certain DNA
sequence contains sequence variations or not.
In 1989 Orita et al. first presented a polymerase chain reaction (PCR) based
SSCA method as an efficient and sensitive method for the detection of DNA
polymorphisms (Orita et al. 1989). The method is based on the principle that
single-strand DNA molecules take on a specific sequence-dependent
secondary structure under non-denaturating conditions. These secondary
structures results in altered gel mobility for variant single-strand DNA
fragments under non-denaturating conditions, compared to the mobility of
the wild type fragments. In brief, during a PCR reaction the fragments are
labeled using radioactive nucleotides, denaturated and separated on nondenaturating polyacrylamide gels followed by gel drying and autoradiography.
The shifted fragments are then excised and sequenced using conventional
MATERIAL AND METHODS | 41
techniques. The optimal length for the detection of SNPs was found to be
150-200 bp and the results are affected by temperature, gel matrix and ionic
strength of the running buffer. The sensitivity for single nucleotide variations
with SSCA is dependent on these variables and has been reported to be 7095% in unselected samples (Sheffield et al. 1993).
DNA-sequencing
The nucleotide sequence of different genes and PCR-products was
determined by manual sequencing using the dideoxy chain termination
method (Sanger et al. 1977) either using radioactive labeled (Paper I) or
fluorescent labeled nucleotides (Papers II and IV). The determination of
known SNPs in the ABCB1, CYP2C8 and CYP3A4 genes was achieved using
pyrosequencing.
The Sanger sequencing method is based on the incorporation of
dideoxynucleotides and thereby stopping the elongation of the DNA
molecule during PCR. In contrast to deoxynucleotides, dideoxynucleotides
have a hydrogen atom attached to the 3’ carbon atom instead of a
hydroxylgroup which prevents the elongation and thereby terminates the
growing DNA chain (Sanger et al. 1977). By labeling the PCR product with
either radioactive or fluorescent nucleotides the length of the different
terminated DNA chains (usually one reaction for each nucleotide) can be
determined by size separation.
The pyrosequencing technique (Ronaghi et al. 1998) is usually suited for
sequencing of shorter fragments as compared to the Sanger sequencing
method. The principle (see Figure 6) is based on the extension of single
nucleotides using the polymerase reaction and the release of pyrophosphate
(PPi). In brief, a sequencing primer is annealed to a single-strand PCRfragment and deoxynucleotide triphosphates (dNTPs) are added in a userpredefined order. If the nucleotide is complementary to the base on the DNA
strand, the released PPi is converted to ATP by ATP-sulfurylase in the
presence of adenosine 5’ phosphosulfate (APS). The ATP generated will be
used by luciferase to convert luciferin to oxyluciferin during which light is
produced. The light created in the reaction is proportional to the amount of
incorporated nucleotide and detected by a charge coupled device (CCD)
camera. Unincorporated dNTPs and ATP are degraded between each cycle by
42 | MATERIAL AND METHODS
apyrase. The result is displayed in a pyrogram and the height of each peak is
used for the determination of the sequence (see Figure 6). It should be noted
that deoxyadenosine alfa-thio triphosphate (dATPS) is used as a substitute for
the natural deoxyadenosine triphosphate (dATP) which is efficiently used by
the DNA polymerase, but not recognized by the luciferase.
Figure 6. In the pyrosequencing reaction, a DNA polymerase incorporates dNTP if
complementary to the template strand upon release of PPi. Adenosine 5’ phosphosulfate
(APS) and PPi is converted by sulfurylase to ATP, which is used by luciferase to convert
luciferin to oxyluciferin during which light is produced. The light registered by a CCDcamera is displayed in a Pyrogram where the height of the peak is proportional to the
amount of dNTP incorporated.
MATERIAL AND METHODS | 43
Solid Phase Extraction
The preparation of biological samples is an important step in the
quantification of low molecular weight analytes in human plasma. The
objective is to remove macromolecules (e.g. proteins and nucleic acids) prior
to High Performance Liquid Chromatography (HPLC) analysis. Due to the
relatively high content of organic solvents in the mobile phases and the
organic substituents in the stationary phases, macromolecules in the biological
matrix can denaturate and precipitate onto the packing material of the
analytical column leading to increased back-pressure and changes of the
chromatographic separation. The preparation of human plasma samples
usually includes precipitation of macromolecules, liquid-liquid extraction
and/or solid phase extraction (SPE). For the preparation of human plasma
samples prior to quantitative analysis we used a SPE for paclitaxel and its
metabolites.
A SPE procedure normally consists of five steps: sample pre-treatment,
SPE activation and conditioning, sample application, matrix washout and
elution of the analytes. The sample pretreatment usually includes
centrifugation of the sample (to avoid clogging of the SPE column) and pH
adjustment to make the analytes suitable for extraction. Prior to applying the
sample on the SPE column, the cartridge requires activation and conditioning.
Activation means that a proper interface is established between the stationary
phase and the sample solvent, in most cases water. During conditioning of the
column, proper absorption conditions are established. When applying the
sample to the SPE column, the analytes are retained by the stationary phase.
The fraction of plasma matrix bound to the column is washed out as
extensively as possible. Aqueous mobile phases, preferably buffered, should
be used for elimination of proteins. Analytes are then eluted by adding an
organic eluent dependent on the structure and affinity of the substances.
44 | MATERIAL AND METHODS
High Performance Liquid Chromatography
The purpose of all chromatography is basically to separate analytes from
each other and from matrix components. According to the International
Union of Pure and Applied Chemistry (IUPAC), chromatography is a physical
method of separation in which the components to be separated are distributed
between two phases, one of which is stationary (the stationary phase), while
the other (the mobile phase) moves in a definite direction (Ettre 1993). In
High Performance Liquid Chromatography (HPLC), the mobile phase is a
liquid delivered under high pressure to ensure constant flow and reproducible
chromatography, while the stationary phase is packed into a column capable
of withstanding the high pressures necessary. The mobile phase in HPLC may
be water, buffers or organic solvents, either on their own or mixed with one
another. The column materials used today are called microparticulate column
packings and are commonly uniform porous spherical silica particles, with a
diameter of 3 to 5 µm (or smaller). Usually specific chemical groups are bound
to the surface of the silica particle, to produce the bonded phase. A variety of
structures have been developed for HPLC in which hydrocarbon chains of
different lengths e.g. C2, C8, C12 and C18 are the most common. HPLC
methods can be subdivided into normal phase, where the polarity of the
stationary phase is higher than that of the mobile phase, and reverse phase,
where the polarity of the stationary phase is less that of the mobile phase.
Different mechanisms of separation such as ion exchange, absorption, size
exclusion, etc. can be achieved depending on the structure and composition
of the stationary and mobile phases. However, in all cases the separation
occurs if the components of a mixture interact to a different extent with the
Figure 7. Schematic description of an HPLC system.
MATERIAL AND METHODS | 45
mobile and/or stationary phases and therefore take different times to move
from the sample injection to detector (Ardrey 2003; Lindsay et al. 1992).
An HPLC system generally consists of six components (more or less
automated): a pump, a sample injector, a mobile phase, a stationary phase, a
detector and an integration system (see Figure 7). The pump delivers the
mobile phase through the column at a rate of 0.1-5 ml/min depending on the
system using a fixed composition of the mobile phase (isocratic) or a changing
composition (gradient). The injection system consists of a valve and an
injection loop where the sample is introduced either manually or by an autoinjector. When the valve is turned the loop becomes part of the mobile phase
delivering system and the analytes are applied to the column. After passing
through the column the separated solutes are sensed by an in-line detector
and the output of the detector is recorded by a computer for integration. A
number of devices can be used as detectors in HPLC. The function of a
HPLC detector is basically to monitor the analytes emerging from the column.
The signal from the detector should be proportional to characteristics of
either the analytes or the mobile phase. Detectors used in this thesis are UV
detectors, a fluorescence detector and an ion-trap mass spectrometer (MS)
and they will briefly be presented here (Ardrey 2003; Lindsay et al. 1992).
UV detectors
The most popular detector in drug analysis
has been the UV detector (see Figure 8). The
principle is that the mobile phase from the
column is passed through a small flow cell and
the absorbence of the UV radiation passed
through the cell is monitored. The detector
has a wide applicability and it is selective in
the sense that it will only detect those solutes
that absorb UV light such as alkenes,
aromatics etc. The absorption is described by
Lambert-Beer’s law (A=abε) and proportional to the length of the flow cell (a), the
molecular absorptivity (ε) and the concentration of the solute (c) (Lindsay et al. 1992).
46 | MATERIAL AND METHODS
Figure 8. Schematic layout of a
UV detector.
Fluorescence detectors
Many compounds are fluorescent, i.e.
they are able to absorb radiation during
which the molecule enters an excited state.
Subsequently when the molecule returns to
its normal state, some of the energy is
released as light of a higher wavelength
which can be used for detection (see Figure
9). Naturally fluorescent molecules usually
have
conjugated
cyclic
structures.
Fluorescence detectors can be much more
sensitive than UV detectors for favorable
compounds and the detector can be highly
selective since both the optimal excitation
and emission wavelengths can be chosen
(Lindsay et al. 1992).
Figure 9. Schematic layout of a
fluorescence detector.
Mass spectrometry
Mass spectrometry (MS) is a technique designed to separate gas phase ions
according to their mass over charge ratio (m/z). Interest in the combination
of HPLC and MS (i.e. LC/MS) has increased tremendously in analytical
laboratories during the last two decades and has become a routine method in
drug monitoring and clinical pharmacology for both quantitative and
qualitative analysis. The mass spectrometer works with charged molecules, i.e.
ions, and uses electrical and magnetic fields to move the ions from the
position of the formation to the detector. The intensity of the signal is
proportional to the concentration or amount of ions that reaches the detector.
In all MS techniques the mass separation works at high vacuum and the
molecules needs to be ionized before entering the mass spectrometer, making
the performance of the interface between HPLC (liquid system and molecules
at atmospheric pressure) and the mass spectrometer (ionized molecules and
vacuum) of great importance. In general the mobile phase matrix must be
eliminated and analytes must be presented as ions in a gas phase (Ardrey
2003). Several types of interfaces have been developed and today atmospheric
pressure ionization (API) techniques such as electrospray ionization (ESI),
MATERIAL AND METHODS | 47
atmospheric pressure chemical ionization (APCI) and sonic spray ionization
(SSI) are the most commonly used interfaces. In the APCI, the LC eluent is
first vaporized and the analytes are ionized in a gas phase in the presence of a
corona discharge electrode by proton transfer, charge exchange, electron
capture or adduct ion formation (Arinobu et al. 2002). In the ESI interface the
ions are already present in the mobile phase, which is then vaporized using
heat and a charged capillary tip. At the tip of the capillary the surface of the
droplets containing the ionized compound will become charged. Due to
solvent evaporation the density of the charge will increase until there is an
explosion of the droplet and the analyte ions enter into a gas phase (Bakhtiar
& Nelson 2000). The SSI interface is similar to an ESI interface, with the
exception that charged droplets are formed without applying an electric field.
Instead the compounds are ionized using only a very high gas flow (Bjorkman
et al. 2002).
Having produced the ions in the interface they are analyzed in the mass
analyzer by determining the m/z and the relative intensity for each ion. There
are a number of different mass separation devices each with its own
advantages and disadvantages. In brief, they can be divided into: sector
instruments, quadrupole instruments, time-of-flight instruments and ion trap
instruments or combinations of these (Ardrey 2003).
Sector instruments are the simplest form of mass analyzer and use electric
and magnetic fields to bend the flight path of accelerated ions. The radius of
the obtained flight path is dependent on the mass-over-charge ratio which is
the principle of separation.
In quadrupole instruments four rods (or more) are arranged in parallel of
which the opposite two are connected. A voltage consisting of both a radio
frequency and a direct-current component is applied to each pair of rods (the
radio frequency being 180° out of phase for the two pairs) and for a specific
value of these voltages, ions of a particular m/z follow a stable trajectory
through the space between the rods and reach the detector.
The mass analyzer used in Paper III and IV is a quadrupole ion trap,
simply ion trap, and is referred to as a three-dimensional quadrupole
(3DQMS). Similar to a quadrupole it is oscillating potentials and radio
frequencies that can selectively differentiate mass-over-charge ratios. The ion
trap consists of a ring electrode and two end cap electrodes as shown in
48 | MATERIAL AND METHODS
Figure 10. The two end caps are either grounded or biased with DC or AC
potential and the ring electrode operates with a sinusoidal radio frequency
applied to it. After the ions are introduced into the ion trap they follow a
stable but complex trajectory and are trapped inside the mass analyzer until a
radio frequency potential is applied to the ring electrode so that ions are
selectively ejected, depending on the m/z ratio, from the trap towards the
detector (Ardrey 2003).
By passing a pulse of electrons into the ion trap, it is possible to fragment
ions in it. The formed fragment ions can be trapped and then selectively
ejected from the ion trap for detection. This procedure is referred to as MS2
or MS-MS analysis. The processes that constitute an MS2 experiment in an ion
trap can be divided into the following steps: trapping of ions formed in the
interface, isolation of ions to be fragmented (i.e. m/z for the precursor ions)
and ejection of all other ions, collision induced dissociation (CID –
fragmentation) of the precursor ions, and detection of the fragments
produced. The usage of MS2 in mass spectrometry usually increases the peakto-noise ratio and is a useful tool in both qualitative and quantitative analysis.
Figure 10. Schematic layout of an ion trap mass spectrometer.
MATERIAL AND METHODS | 49
Statistics
The statistical analysis in this thesis was performed with EpiInfo 2002 and
the SPSS software package version 11 or higher (SPSS Inc. Chicago, IL, USA).
The allele distributions presented in Papers II and IV were found to be in
Hardy-Weinberg equilibrium using χ2-test. The significance of differences in
nominal data was calculated using generalized Fisher’s exact test (Papers II
and IV). The relative risk (RR) of not responding to treatment with a 95% CI
was calculated when applicable (Paper II). The χ2-test for linear-by-linear
association was used to analyze the significance of trends in different tables.
The Mann-Whitney U-test is a non-parametric test and used to identify
differences between two independent groups (Paper IV). Linear regression
was used when investigating the correlation of two continuous variables
(Paper IV). Kaplan-Meier plot, Log Rank and Breslow tests were used to
visualize and test differences in fractions of patients with progression-free
survival between different genotypes. The P-values for the 2-sided
significance were always presented.
The precision of the LC/MS method was expressed as a coefficient of
variation (CV) at each concentration by calculating the standard deviation as a
percentage of the mean calculated concentrations, while accuracy of the
method was evaluated by expressing the mean calculated concentration as a
percentage of the nominal concentration (Paper III).
50 | MATERIAL AND METHODS
RESULTS AND DISCUSSION
The Scarcity of β-tubulin Mutations in Ovarian Tumors
In Paper I we investigated the presence of mutations in the β-tubulin M40
gene as a potential resistance mechanism for paclitaxel. We investigated all the
exons including the exon/intron boundaries of the gene without finding any
sequence variations in genomic DNA from 40 chemonaive ovarian tumors.
However, in eight samples from paraffin-embedded tumors we found
numerous false positive mutations i.e. the shift was not reproducible in
independent PCRs with original tumor DNA. In the first study of β-tubulin,
Monzo et al. found mutations in about 30% of the patients with NSCLC
(Monzo et al. 1999). The interpretation of these results has been questioned
due to the use of non-specific primers (Hasegawa et al. 2002; Kelley et al.
2001) and, as shown in Paper I, the use of paraffin-embedded tissue might
also explain the high frequency in that material.
Our results in Paper I in ovarian cancer are in accordance with the results
reported by several groups that the mutations in the β-tubulin gene are rare in
clinical samples (Kelley et al. 2001; Kohonen-Corish et al. 2002; Lamendola et
al. 2003; Mesquita et al. 2005; Sale et al. 2002b). Other groups have found
synonymous mutations/polymorphisms in the β-tubulin gene, especially at
codons 180 (GTC>GTT), 195 (AAT>AAC) and 217 (CTG>CTA)
(Hasegawa et al. 2002; Sale et al. 2002b; Tsurutani et al. 2002). Several of these
RESULTS AND DISCUSSION | 51
sequence variations are present in pseudogenes and no correlation to response
was found. It is noteworthy that almost all these sequence variations were
found in Asian, African or Oceanic populations and none in Caucasian
populations which might explain the discrepancies between the studies.
However, we cannot exclude that mutations occur later during the tumor
progression or in other β-tubulin isoforms. In vitro studies in cell lines indicate
that paclitaxel can induce mutations in β-tubulin with altered sensitivity to
paclitaxel as a result (Giannakakou et al. 1997; Gonzalez-Garay et al. 1999;
Wang et al. 2005b), although mutations have not been found in resistant or
relapsed tumors (Lamendola et al. 2003; Mesquita et al. 2005; Sale et al. 2002b).
The scarcity of true somatic mutations as well as non-synonymous
polymorphisms in clinical samples indicate that it is not likely that sequence
variations in the tubulin gene constitute a resistance mechanism to paclitaxel
in human tumors and therefore cannot be used to predict the clinical response
to drugs targeting β-tubulin.
Allele Frequencies of SNPs in ABCB1, CYP2C8 and CYP3A4
in a Swedish Population and in Ovarian Cancer Patients
The allele frequencies of SNPs in ABCB1, CYP2C8 and CYP3A4 were
investigated in a Swedish reference population and ovarian cancer patients
(Table V) to study if the SNPs were correlated to the disease, if there was a
linkage between the sequence variations and if the allele frequencies were
comparable with previous findings. Pyrosequencing was used to detect the
SNPs in paraffin-embedded material, freshly frozen tumors as well as DNA
extracted from blood samples. Pyrosequencing was chosen as a method since
it is a fast method, it gives a short sequence of the PCR-product – confirming
a correct amplification, it gives a quantitative assessment (peak height) of the
analysis, and several SNPs can be run in each reaction. dHPLC was excluded
due to the fact that it only detects heterozygous individuals unless known
PCR products are added and RFLP was not chosen due to the laborious
protocol and the manual evaluation of gels. All the studied SNPs were present
in Hardy-Weinberg equilibrium and there was no difference in the distribution
between healthy volunteers and ovarian cancer patients (although the
CYP2C8 promotor SNPs are borderline cases) or between males and females.
52 | RESULTS AND DISCUSSION
The allele frequencies were in accordance with previous frequencies found in
Caucasian populations (Bahadur et al. 2002; Marzolini et al. 2004; Solus et al.
2004).
Table V. The SNP frequencies in a Swedish population (n=195) and the allele distribution
of the different SNPs in ovarian cancer patients.
Nucleotide
Swedish ref.
Alleles/SNPs
Ovarian Cancer Patients
change
population
n=195
freq. +/- 95% CI
Wild type
Heterozygous
mutated
Homozygous
mutated
T-370G
C-271A
A805T
G416A, A1196G
C792G
475 Del A
G511A
C556T
C556G
C1210G
10% +/- 3,0%
29% +/- 4.5%
0%
11% +/- 3.1%
6,0% +/- 2.4%
0%
0%
0%
0%
0%
21
22
33
27
29
33
33
33
33
33
12
10
0
6
4
0
0
0
0
0
0
1
0
0
0
0
0
0
0
0
A-392G
4,4% +/- 2.0%
30
3
0
G 56%+/- 4.9%
T 42% +/- 4.9%
A 2% +/- 1.5%
T 55 % +/- 4.9%
Paper II: 14
Paper IV: 5
28 G/T
17 G/T 3 G/A
9 T/T 2 T/A
8 T/T
CYP2C81
*1C
*1B
*2
*3
*4
*5
*6
*7
*8
P404A
CYP3A4
*1B
ABCB1
Ex21
G2677T/A
Ex26
C3435T
Paper II: 8
27
18
Paper IV: 4
19
10
1
Note: CYP2C8*1C and *4 were present in a linkage disequilibrium and CYP2C8*1B was present
mutually exclusive of *1C, *3 and *4.
In the ABCB1 gene the G2677T and C3435T were found to be in linkage
disequilibrium (D’ = 0.92, Table VI) in agreement with previous findings
(Marzolini et al. 2004; Pauli-Magnus & Kroetz 2004; Sakaeda et al. 2002).
Table VI. The distribution of ABCB1 SNPs G2677T/A
and C3435T in a Swedish population (n=195).
C3435T
G2677T/A
C/C
T/C
T/T
Σ
G/G
39
20
2
61
G/T
3
59
28
90
T/T
1
0
34
35
G/A
2
3
0
5
T/A
0
4
0
4
A/A
0
0
0
0
Σ
45
86
64
195
RESULTS AND DISCUSSION | 53
Correlations of ABCB1 Genotypes with the Response to
Paclitaxel
In Paper II we showed that the non-synonymous SNP G2677T/A
significantly correlated with the outcome of paclitaxel-carboplatin treatment in
the Swedish ovarian cancer population studied. The 53 patients included in
this study were subdivided according to their response to treatment. Patients
having a complete response and remained relapse-free for at least one year
were considered to be good responders and patients who had progressive
disease during treatment or relapsed within 12 months were considered to be
poor responders to paclitaxel-carboplatin treatment. The probability of
responding was higher for patients who were homozygously mutated for
G2677T/A (T/T or T/A) as compared to patients carrying the wild-type
alleles and heterozygous patients (Figure 11A). Nine of 28 patients with good
response were homozygously mutated as compared to two of 25 patients with
poor response. The fraction of mutated alleles was also higher in the group of
patients with good response (Figure 11B) and there was also an influence of
the number of mutated alleles on the response to paclitaxel-carboplatin
treatment (Figure 11C).
Figure 11. The effect of the ABCB1 SNP G2677T/A on the treatment outcome. A) The
frequency of good response (white) and poor response (black) among homozygously
mutated individuals (T/T or T/A) as compared to the individuals having G/G or G/T at
position 2677 (Fisher’s exact test P=0.04, relative risk (RR) = 1.81, 95% CI: 1.17
<RR<2.79). B) The nucleotide frequencies in the two treatment groups. A significantly
higher fraction of T or A at position 2677 was found in the group of patients that had
responded well to treatment compared to those who responded poorly (Fisher’s exact test
P=0.03, RR = 1.59, 95% CI: 1.03<RR<2.45). C) The gene-dose effect of the number of
variant alleles significantly correlated with the success of paclitaxel treatment (χ2 -test for
linear-by-linear association, P=0.03).
54 | RESULTS AND DISCUSSION
We also investigated the effect of the ABCB1 G2677T/A genotype on the
progression free survival using a Kaplan-Meier analysis (Figure 12). Although
not significant, the curves show a trend in time to progression due to ABCB1
genotype (P = 0.19, log-rank test; P = 0.09, Breslow). The mean time to
progression for the patients with the G/G genotype was 1.2 years, for
heterozygous patients with G/T genotype 1.4 years, and for homozygously
mutated patients (T/T or T/A) the mean time to progression was 2.0 years.
We could not show any effect of the C3435T SNP on the response to
paclitaxel-carboplatin treatment.
Figure 12. The effect of the ABCB1 SNP G2677T/A on progression-free survival.
To our knowledge this was the first study investigating the effect of the
ABCB1 genotype on the success of paclitaxel-carboplatin treatment. Several
other groups had investigated the effect of the ABCB1 genotype on the
response to chemotherapy. Obata et al. investigated the correlation between
the response in 60 advanced ovarian cancer patients and SNPs in ABCB1,
MRP1, MRP2 and LRP (Obata et al. 2006). They found a correlation between
an SNP in exon 17 of MRP1 and the response at the end of chemotherapy
but not to the disease-free survival. No correlation between the ABCB1
genotype and the response was found, although they did not genotype for the
SNP G2677T/A and only 20 of 60 patients received taxane (paclitaxel or
RESULTS AND DISCUSSION | 55
docetaxel) containing chemotherapy. In a study on acute myeloid leukemia
(AML) patients Illmer et al. found that patients wild type for C1236T,
G2677T/A and C3435T had a higher risk of relapse (Illmer et al. 2002). This is
in accordance with our results showing a better prognosis for homozygously
mutated ovarian cancer patients treated with paclitaxel-carboplatin. In
contrast, Kim et al. found that AML patients wild type for ABCB1 G2677T/A
and C3435T had a better prognosis (Kim et al. 2006). The discrepancies
between these two AML studies might be due to ethnic differences in
Caucasians and Koreans as well as the use of different P-gp substrates in the
treatment regimens, idarubicin (Kim et al. 2006) versus daunorubicin and
doxorubicin (Illmer et al. 2002). Most other studies have only investigated the
effect of the C3435T polymorphisms which is linked with G2677T/A as
shown by us and others (Marzolini et al. 2004; Pauli-Magnus & Kroetz 2004;
Sakaeda et al. 2002). It has been proposed that the effect observed when
studying one of the SNPs might be due to the other one (Kroetz et al. 2003),
although the SNPs might be associated with different haplotypes in different
populations. Considering this linkage, our results in Paper II are similar to
those by Jamroziak et al. showing that children with acute lymphoblastic
leukemia carrying C/C in position 3435 had a worse prognosis after
anthracycline-containing treatment (Jamroziak et al. 2004). Kafka et al. also
showed that breast cancer patients homozygously mutated in position 3435
and treated with anthracyclines alone or in combination with taxanes had a
higher probability of complete clinical response (Kafka et al. 2003). The
investigation by Illmer et al., these two studies and our results all suggest that
patients having one or more wild type alleles of the SNPs are at higher risk of
not responding to treatment. In contrast to this, Isla et al. did not find any
association between the C3435T polymorphism, and the response to
docetaxel-cisplatin treatment of NSCLC and Goreva et al. found that patients
homozygously mutated for G2677T/A and C3435T had a higher risk of drug
resistance (Goreva et al. 2003; Isla et al. 2004). However, one should keep in
mind that there might be ethnic differences in the association of these SNPs
to different haplotypes as well as their importance in drug therapy. Different
amino acids at position 893 (Ala, Ser or Thr, nucleotide position 2677) might
have different effects on different drugs and the concentration of the drug
may also be important for the impact of the genetic polymorphism.
56 | RESULTS AND DISCUSSION
After the publication of Paper II two groups have published similar studies,
but with different results (Ludwig & Kupryjanczyk 2006; Marsh et al. 2006).
Marsh et al. assessed the ABCB1 G2677T/A genotype in patients included in
the SCOTROC1 trial, a large and well-defined phase III clinical trial designed
to compare the effects of paclitaxel versus docetaxel in combination with
carboplatin in ovarian cancer (Vasey et al. 2004). Although the paclitaxel
treatment regimens in these studies were similar, there are several differences
between the studies which might explain the discrepancies in the results.
Compared to our national case-referent study in the southern part of Sweden
the SCOTROC1 is an international multicenter study and since our material
was from a biobank we probably have an overrepresentation of large tumors.
We also have a higher proportion of patients with non-radical surgery than
the SCOTROC1 study as well as a higher fraction of patients with FIGO
stage IIIc. It has been shown that a higher percentage of tumors with FIGO
stage IIIc have a gain in the 7q21 region (Partheen et al. 2004), where the
ABCB1 gene is located, which might explain a higher impact of the ABCB1
SNPs in these patients. We assume that Marsh et al., although not stated,
subdivided the SCOTROC1 patients into paclitaxel- and docetaxel-treated
patients because paclitaxel and docetaxel might not be affected in the same
way by these SNPs. In the study by Ludwig et al. they investigated the
distribution of the G2677T/A SNP in Polish ovarian cancer patients with
FIGO stage IIb-IV and poor tumor differentiation (Ludwig & Kupryjanczyk
2006) without finding any association of the T/T genotype to the treatment
response. However, they did find a higher risk of death for these patients
(Cox’s proportional hazards model). There are some differences in the
populations studied in this study as compared to ours. However, the
information given in the letter by Ludwig et al. is scanty and therefore it is
difficult to draw any conclusions. The results in the two studies were also
evaluated in different ways and the number of patients in each response group
in the study by Ludwig et al. is not presented so it is difficult to evaluate the
results.
The polymorphisms of the ABCB1 gene have been investigated in
numerous studies giving conflicting results for several P-gp substrates such as
digoxin, fexofenidine, cyclosporine, and tacrolimus, as well as expression and
function of P-gp (see review by Marzolini et al. 2004). So far, the relevance of
RESULTS AND DISCUSSION | 57
the ABCB1 genotype for different P-gp substrates and for response to
chemotherapy remains elusive and further studies are needed. We believe that
the discrepancies between our relatively small study, the Polish study and the
pharmacogenetic follow-up study of the SCOTROC1 trial may be explained
by differences in the composition and/or subdivision of tumors and/or
patients as well as the different ways of evaluating the results. However, these
three studies show the importance of validating the results of a small pilot
study in larger independent studies as well as the need to use well-defined
populations and evaluation procedures, and that analyses on relatively small
clinical groups may more easily generate statistical significances by chance.
The use of the ABCB1 genotype as a predictor for paclitaxel response is still
elusive and future studies will hopefully clarify the significance of these SNPs.
58 | RESULTS AND DISCUSSION
Quantification of Paclitaxel and its Hydroxymetabolites in
Human Plasma
To investigate the effect of different factors such as genetic variations in
genes encoding drug transporters and metabolic enzymes on the
pharmacokinetics of paclitaxel we needed a method to quantify paclitaxel and
its metabolites in human plasma. The final method used for measurement of
paclitaxel and its metabolites in this thesis is presented in Paper III.
Numerous methods have been developed for the quantification of
paclitaxel in plasma using different techniques such as liquid chromatography
(Theodoridis & Verpoorte 1996), capillary electrophoresis (Hempel et al.
1996), enzyme-linked immunosorbent assay (ELISA) (Svojanovsky et al. 1999)
and radioimmunoassay (Leu et al. 1993). However, it has been suggested that
the preferable technique to measure the concentrations of paclitaxel and its
metabolites is by HPLC with a UV detector, fluorescence detector or mass
spectrometer (Theodoridis & Verpoorte 1996). We therefore started by
developing an extraction method and a HPLC-method for quantification of
paclitaxel and its metabolites in human plasma.
Extraction of paclitaxel from human plasma
Liquid-liquid extraction (LLE) as well as solid-phase extraction (SPE), online (Sparreboom et al. 1995b) and off-line, has been used for sample clean-up
and extraction of paclitaxel from human plasma. For extraction of paclitaxel
from plasma using LLE several organic solvents such as ethyl-acetate,
diethylether, methyl tert-butyl ether and acetonitrile have been used (Andreeva
et al. 1997; Martin et al. 1998; Poon et al. 1996; Sottani et al. 2000; Wang et al.
2003). We investigated the use of LLE for the extraction of paclitaxel and its
metabolites by mixing a number of different organic solvents with plasma,
adding potassium carbonate, centrifugation (4000g, 10min) followed by
freezing. The upper organic level was carefully transferred to a tube,
evaporated to dryness and reconstituted in mobile phase and checked for the
extraction recovery and purity using the HPLC-method described below.
Isopropanol, ethanol, acetonitrile, ethanol/acetonitrile (60/40), acetone,
methyl tert-butyl ether and ethyl-acetate were investigated; however, the
extracts using these solvents were not clean enough for positive identification
RESULTS AND DISCUSSION | 59
of the metabolites and in most cases the recovery was less than 50% for the
metabolites, although the extraction of paclitaxel was satisfactory for some of
the solvents (data not shown). Therefore SPE was tested for the extraction of
paclitaxel and its metabolites. We adopted the SPE method from Huizing et al.
with slight modifications (Huizing et al. 1998; Huizing et al. 1995a). In this
method CN solid-phase columns are used and the plasma samples are
buffered prior to application to the column, washed with buffer, methanol
and hexane before elution with acetonitrile. The recovery of paclitaxel and its
metabolites were originally between 83-117% but lower in Paper III: paclitaxel
range 63-74%, p-3´-hydroxypaclitaxel 65-71%, and 6α-hydroxypaclitaxel 7285%. The difference is most likely due to different batches of SPE-columns as
previously described (Huizing et al. 1998). We also investigated the use of
other stationary phases such as C2, C4, C8, C18, phenyl and NH2. However,
we were not able to get a satisfactory clean-up or a high enough recovery
from these columns. In spite of the batch dependent recoveries of the
substances from the CN columns, we adopted the SPE method by Huizing et
al. 1995a.
Quantification of paclitaxel and metabolites using HPLC
The HPLC-method we developed for the quantification of paclitaxel and
metabolites in plasma were also based on the method by Huizing et al. 1995a
although the mobile phase was changed and docetaxel used as internal
standard. We used a Chromeleon system consisting of a Gynkotek model 480
pump, a Gynkotek Gina 50 auto-sampler and a Gynkotek 340U UV-detector.
The column was an Apex I C8 (150x3 mm 5µm) and the flow of the mobile
phase (acetonitrile/20 mM ammonium acetate pH 5.0 45/55) was 0.7 ml/min.
Fifty µl of the extracted sample was injected on the column. Typical
chromatograms recorded at 227 nm with the corresponding retention times
for each substance are shown in Figure 13. The lower limit of quantification
for this method was 10 ng/ml of paclitaxel and the metabolites in human
plasma (within-day variations <15%). However, after analyzing samples from
the first three patients in Paper IV we concluded that this was not sensitive
enough for the metabolites although the quantification of paclitaxel was
satisfactory. We believed that to evaluate the metabolic pathways and the
influences of the CYP2C8 and the CYP3A4 enzyme activities in the individual
60 | RESULTS AND DISCUSSION
7,5
5
2,5
5
2,5
Rt 6.5 min docetaxel
Rt 7.2 min paclitaxel
7,5
Rt 3.8 min p-3’-hydroxypaclitaxel
10
Intensity (AU)
Intensity (AU)
10
Rt 4.7 min 6α-hydroxypaclitaxel
Spiked plasma
Blank plasma
0
0
-2,5
-2,5
0
2
4
6
Time (min)
8
10
0
2
4
6
8
10
Time (min)
Figure 13. Typical chromatograms for the HPLC method developed during this thesis.
The spiked plasma sample contained 50 ng/ml of each metabolite and 250 ng/ml of
paclitaxel as well as docetaxel. AU – Arbitrary unit, Rt – Retention time.
patient it was important to quantify the metabolites. The concentration of the
metabolites, especially p-3´-hydroxypaclitaxel, was found to be below 10
ng/ml within two to three hours after the end of infusion in some patients.
We therefore decided to investigate the use of other detectors. Since paclitaxel
contains several conjugated double bonds we concluded that the substance
might be fluorescent and that fluorescence detection might improve the
sensitivity. The fluorescence of paclitaxel was investigated by registering the
fluorescence intensity from 210-800 nm while the molecule was exposed to
light with a wavelength of 200-290 nm (corresponding to the maximum in the
absorption spectrum of paclitaxel); see Figure 14. Maximum fluorescence
intensity was reached using an excitation wavelength of 230 nm and an
emission wavelength of 310 nm. Replacing the UV detector in the abovementioned system with a Waters 474 fluorescence detector and using the 230
nm for excitation and 310 nm for emission gave us a fluorescence method for
the detection of paclitaxel and metabolites (mobile phase - acetonitrile/20
mM ammonium acetate pH 5.0 42.5/57.5). A chromatogram is shown in
Figure 15. Unfortunately this method resulted in additional peaks in the
chromatogram of which several were interfering with the peaks of our
RESULTS AND DISCUSSION | 61
2000
280
1500
1000
240
500
Excitation wavelenght (nm)
Emission intensity (mV)
2500
200
0
200
400
600
800
Emission wavelength (nm)
Figure 14. Fluorescence spectra of paclitaxel.
analytes. However, the data indicated that the sensitivity for especially p-3´hydroxypaclitaxel improved with the use of a fluorescence detector. We could
then either try to clean up the sample even more, try to change the
chromatography to separate the interfering peaks or use another type of
detector. Due to the difficulties of extracting paclitaxel from human plasma
and the number of interfering peaks we turned to the use of LC/MS.
Spiked plasma
10
10
7,5
7,5
Intensity (AU)
Intensity (AU)
Blank plasma
5
2,5
Rt 5.0 min p-3’-hydroxypaclitaxel
Rt 6.0 min 6α-hydroxypaclitaxel
Rt 8.5 min docetaxel
5
Rt 9.6 min paclitaxel
2,5
0
0
0
5
10
15
Time (min)
20
0
5
10
15
20
Time (min)
Figure 15. Typical chromatograms for the fluorescence method developed during this
thesis. The spiked plasma sample contained 10 ng/ml of each substance. AU –
Arbitrary unit, Rt – Retention time.
62 | RESULTS AND DISCUSSION
Quantification of paclitaxel and metabolites using LC/MS
The available LC/MS system in our lab consists of a LaChrome
chromatograph with a Merck-Hitachi M-8000 LC/MSn (ion trap) equipped
with exchangeable SSI and ESI interfaces. In most previously reported
LC/MS methods, paclitaxel either forms [M+H]+ ions or [M+Na]+ ions. To
form the [M+H]+ ion in the interface, usually an acidic mobile phase is used,
and when the [M+Na]+ ion is desired sodium salts are added. In our method
development we tried to use acidic mobile phases to form the [M+H]+ ion.
However, in our system we could not achieve reproducible formation of the
protonated ion between different batches of acidic mobile phase. The
instability was probably due to the formation of a lower or higher amount of
[M+Na]+. In an effort to stabilize the system, different ions were added to the
mobile phase to push paclitaxel to form other adducts, and those that could
be detected in our system were [M+K]+ (KCl 2 mM/MeOH 30/70),
[M+Na]+ (NaCl 2 mM/MeOH 30/70), and [M+Acetate]- (ammoniumacetate
20 mM/MeOH 30/70). The highest sensitivity of these adducts was reached
with the [M+K]+ ion although the sensitivity for the [M+H]+ ion was higher
than any of the other ions formed, probably due to fragmentation of the latter
in the ion source. In an attempt to stabilize the formation of the [M+H]+ ion
we returned to the use of acidic mobile phases and tried to suppress the
formation of the [M+Na]+ ion by adding crown ethers or trifluoroacetic acid
(TFA). Although TFA caused a decrease of the absolute signal, the signal-tonoise ratio for paclitaxel was increased, and the formation of the [M+Na]+ ion
was suppressed resulting in a stable formation of the [M+H]+ ion. The mobile
phase was optimized for TFA concentration and pH. The MS conditions were
optimized using a continuous infusion of a solution containing paclitaxel
while running the optimized mobile phase components. Both the SSI and ESI
interface was evaluated for the method and the SSI interface was about four
times more efficient in ionizing paclitaxel. We also had the opportunity to test
the ionization on a Perkin Elmer SCIEX equipped with both an ESI and an
APCI interface. In this system, the ESI was more efficient in ionizing
paclitaxel than the APCI interface. The SSI interface was then considered the
best choice. The use of an MS2 method instead of a MS1 method further
increased the sensitivity. The HPLC column was chosen to retain and separate
the analytes since some of them have identical mass-to-charge ratios after
RESULTS AND DISCUSSION | 63
Figure 16. Fragmentation of paclitaxel and its metabolites in our ion trap – mass spectormeter.
fragmentation in the ion trap. The monohydroxymetabolites have the same
molecular mass but they fragment into ions with a different m/z. However, p3’-hydroxypaclitaxel dissociates into fragments with the same m/z as
fragments from paclitaxel and 6α-hydroxypaclitaxel dissociates into fragments
with the same m/z as dihydroxypaclitaxel (Figure 16). To achieve single-peak
mass chromatograms two methods were run in parallel, one for paclitaxel and
dihydroxypaclitaxel and one for the monohydroxymetabolites. A typical
chromatogram of the method is shown in Figure 17. The method was
validated as described in Paper III. The CV for the precision was below 15%
and accuracy was between 83-113% with the exception of the within-day
accuracy for the lowest quality control sample for paclitaxel which was 151%.
The within-day accuracy was then rerun the following three days with
satisfactory result (80%, 103% and 88%) and the between-day accuracy was
93% for this concentration. For most samples re-injection data was also
higher than 100% but this is probably due to a slight increase in concentration
when the sample equilibrates with the atmosphere in the sample vial. Since
there were a lot of quality controls run during the validation of this method a
few analyses did show a fairly high variation. However, this reflects the actual
64 | RESULTS AND DISCUSSION
12
10
8
6
900
800
700
600
500
400
300
4
200
2
100
0
0
0
3
6
Intensity (AU) for paclitaxel
14
1000
- Rt 6.1 min Paclitaxel
16
- Rt 5.1 min 6α-hydroxypaclitaxel
18
- Rt 3.6 min p-3'-hydroxypaclitaxel
Intensity (AU) for the hydroxymetabolites
20
9
Time (min)
Figure 17. Typical chromatograms for the ion trap method presented in Paper III. The
substances were isolated from plasma from an ovarian cancer patient and quantified as 42
ng/ml p-3’-hydroxypaclitaxel, 36 ng/ml 6α-hydroxypaclitaxel and 1440 ng/ml paclitaxel. In
the chromatogram the baseline for the 6α-hydroxypaclitaxel is elevated with 2 arbitrary
units (AU) and that for paclitaxel with 200 AU for illustrative purposes. Note that the peak at
6.1 min in the p-3´-hydroxypaclitaxel chromatogram is from “overspill” of paclitaxel (more
than 100-fold intensity in the correct method) and that the peak at 7.5 min in the 6αhydroxypaclitaxel chromatogram is from the internal standard, which has a 13C fragment
with the same m/z as the metabolite. AU – Arbitrary unit, Rt – Retention time.
precision and accuracy of the method and we felt that since we are running a
method for the quantification of paclitaxel concentrations over a range of 1 to
10,000 and including all the hydroxyl metabolites we needed five quality
control samples for each analyte (although a more stable, reproducible and
sensitive method would (always) have been desirable). Our method (Paper III)
for quantification of paclitaxel and metabolites in human plasma is to our
knowledge the first reported method using an ion trap mass spectrometer
with an SSI interface and TFA as a suppressor of paclitaxel Na-adduct
formation. The advantage of the method is the high sensitivity, the
quantification of paclitaxel and its metabolites; a drawback is the spiking of
RESULTS AND DISCUSSION | 65
the chromatograms which is discussed in the paper and led to reanalysis of
some samples.
The method presented in Paper III however suited our purposes for the
quantification of paclitaxel and its metabolites in plasma. The concentration
of paclitaxel and its hydroxymetabolites was determined in more than 450
human plasma samples used in Paper IV. The lowest concentration of
paclitaxel found in samples taken 24 hours after the end of paclitaxel infusion
was 17 ng/ml and the lowest measured concentration of p-3’hydroxypaclitaxel was 0.75 ng/ml although this metabolite was not detectable
in some samples. Considering the performance of the method presented in
Paper III the quantification of paclitaxel, the findings in Paper IV concerning
the exposure and clearance of paclitaxel should be valid.
66 | RESULTS AND DISCUSSION
Correlations of Paclitaxel Pharmacokinetics to ABCB1,
CYP2C8, CYP3A4 Genotypes and CYP3A4 Phenotype
In Paper IV we investigated the effects of CYP3A4, CYP2C8 and ABCB1
sequence variations and the CYP3A4 activity in vivo on the pharmacokinetics
and clinical effects of paclitaxel in the treatment of ovarian cancer. A total of
33 ovarian cancer patients were included and assessed for their individual
capacity to eliminate paclitaxel. Genotyping of SNPs in the CYP3A4,
CYP2C8 and ABCB1 genes was done by pyrosequencing and the CYP3A4
activity in vivo was assessed using quinine as a probe drug. The patients were
monitored for response during the chemotherapy as well as for adverse drug
reactions, especially neurological toxicity, evaluated as Nscore (Cassidy et al.
1998) and the patients’ own rating of their discomfort due to neurological
adverse reactions.
The results presented in Paper IV indicate that the clearance of paclitaxel is
correlated to the SNPs G2677T/A in ABCB1 and CYP2C8*3. Patients
heterozygous for G/A in position 2677 in the ABCB1 gene had a significantly
higher clearance (median 26.0 L/h) compared to patients carrying the wildtype G/G alleles (median 18.9 L/h) or patients homozygously T/T mutated
(median 17.4 L/h); however, no significant difference could be shown
compared to the G/T heterozygous patients (median 21.1 L/h) (Figure 18A).
We also found indications that CYP2C8*3 and CYP3A4*1B correlated with
the clearance of paclitaxel, although not statistically significant. To further
investigate this, we stratified the data according to the ABCB1 SNP
G2677T/A; however, the only combination where the number of patients was
high enough for statistical analysis (n>2) was the combination of 2677G/T
and CYP2C8*1/*1 versus 2677G/T and CYP2C8*1/*3. Patients carrying the
2677G/T and CYP2C8*1/*3 alleles had a significantly lower clearance of
paclitaxel (median 14.7 L/h) than patients carrying the 2677G/T and
CYP2C8*1/*1 alleles (median 22.8 L/h) (Figure 18B). The clearance of
paclitaxel did not correlate to the genotypes ABCB1 C3435T, CYP2C8*1B,
CYP2C8*1C or CYP2C8*4, nor to the CYP3A4 enzyme activity in vivo.
RESULTS AND DISCUSSION | 67
Figure 18. The influence of the ABCB1 G2677T/A and CYP2C8*3 SNPs on the clearance
of paclitaxel. A) The clearance of paclitaxel due to the ABCB1 genotype in position 2677.
B) The effect of CYP2C8*3 on the clearance of paclitaxel is shown for patients with the
ABCB1 genotype 2677G/T.
A low CYP3A4 enzyme activity in vivo correlated with a high AUC0-24h for
6α-hydroxypaclitaxel (R = 0.671 , P < 0.001, data not shown), indicating that
in patients with low CYP3A4 activity a higher proportion of paclitaxel is
converted by CYP2C8 or that the elimination of 6α-hydroxypaclitaxel is
decreased. A lower CYP3A4 enzyme activity in vivo also correlated to a higher
ratio of the AUC0-24h for 6α-hydroxypaclitaxel divided by AUC0-24h for p-3’hydroxypaclitaxel (6α-OH-pac/p-3’-OH-pac) (R = 0.525, P = 0.002, data not
shown). This indicates that the CYP3A4 enzyme activity in vivo influences
which pathway, CYP2C8 or CYP3A4, is relatively more dominant in each
patient. CYP2C8*1C also correlated with a higher 6α-OH-pac/p-3’-OH-pac
ratio (P = 0.048, data not shown), although no other pharmacokinetic
parameter investigated was affected by this SNP.
Patients having the combination 2677G/T and CYP2C8*1/*3 had a higher
AUC0-24h for 6α-hydroxypaclitaxel in plasma than CYP2C8 wild-type patients
(SNP combination 2677G/T and CYP2C8*1/*1) (P = 0.032, data not
68 | RESULTS AND DISCUSSION
shown), which is in contradiction to the lower clearance for these patients. A
high CYP3A4 enzyme activity in vivo correlated to a low AUC0-24h for p-3’hydroxypaclitaxel (R = 0.354, P = 0.051, data not shown). Both these findings
indicate that a high enzyme activity for the metabolizing enzymes is correlated
with a low concentration of the metabolite in plasma, which is difficult to
explain. However, the metabolism mainly occurs in the liver and the
metabolites are believed to be directly eliminated via the bile (Gianni et al.
1995), so the plasma concentration might not reflect the metabolite formation
in the liver. Gianni et al. reported that measured metabolite concentrations
represent an overflow at times of relative saturation or blockage of biliary
elimination (Gianni et al. 1995). We therefore speculate that if paclitaxel, at
times of low enzymatic elimination, is saturating the biliary elimination of the
metabolites, then these substances would be present at a higher concentration
in plasma when we have a low clearance of paclitaxel. The saturation effect
has also been suggested by others (Nakajima et al. 2005). None of the other
genotypes could be correlated to the AUC0-24h for either of the metabolites.
In one investigation of the influence of genetic variations on the
pharmacokinetics of paclitaxel, Yamaguchi et al. found that ovarian cancer
patients having the ABCB1 genotype -129T/C, 1236C/C and 2677A/A had
the highest clearance and the lowest AUC of paclitaxel (Yamaguchi et al.
2006). This is in agreement with our results in Paper IV showing that patients
carrying 2677G/A had the highest clearance. However, Nakajima et al. did not
find an association between the ABCB1 genotype (T-129C, C1236T,
G2677T/A and C3435T) and the clearance of paclitaxel, although they found
that patients mutated in position 3435 had a higher AUC for p-3’hydroxypaclitaxel compared to the wild-type patients (Nakajima et al. 2005).
Nor did Sissung et al. find an association between the genotype of ABCB1 and
the pharmacokinetics of paclitaxel. However, like our study and the others
mentioned, this is a small study and the statistics approach significance (P =
0.18) for the correlation between G2677T/A and C3435T and the AUC of
paclitaxel (Sissung et al. 2006). A correlation has also been found between
altered metabolite ratios and the haplotype CYP3A4*16B as compared to
wild-type (Nakajima et al. 2006). CYP3A4*1B was not found in the material
and no difference in paclitaxel clearance was found between the CYP3A4
haplotypes. This is similar to our results, where we found a correlation
RESULTS AND DISCUSSION | 69
between CYP3A4 activity in vivo and the 6α-OH-pac/p-3’-OH-pac ratio, but
no correlation to the clearance of paclitaxel. Due to the scarcity of CYP2C8
SNPs in a Japanese population (Hichiya et al. 2005), neither of these Japanese
studies found a high enough number of variant CYP2C8 alleles for a statistical
analysis. A larger study done in a Caucasian population investigated the
clearance of unbound paclitaxel in cancer patients receiving paclitaxel as an
i.v. infusion for 1, 3 or 24 h at doses of 80-225 mg/m2 (Henningsson et al.
2005). Although they found a high interindividual variation in clearance of
unbound paclitaxel (10-fold), no statistically significant association was
observed between the pharmacokinetics of paclitaxel and any genotype
investigated (CYP2C8*2, CYP2C8*3, CYP2C8*4, CYP3A4*3, CYP3A5*3C
and ABCB1 C3435T). This is in contradiction to our findings concerning a
reduced elimination of paclitaxel in patients heterozygous for CYP2C8*3.
Most in vitro studies as well as findings for repaglinide (Niemi et al. 2003) and
ibuprofen (Garcia-Martin et al. 2004) suggest that CYP2C8*3 can affect the
pharmacokinetics of its substrates. The differences between our study and the
results presented by Henningsson et al. might be due to the use of a wide
range of dosages and infusion times, since the SNPs might have different
impacts at different concentrations of paclitaxel, although their study has the
advantage of measurement of unbound paclitaxel. We also found an impact of
the ABCB1 G2677T/A SNP, which Henningsson et al. did not genotype for,
and we had to stratify the data accordingly to evaluate the effect of
CYP2C8*3.
In summary, it seems as if the genotype of ABCB1, especially G2677T/A,
plays a role in the pharmacokinetics of paclitaxel. CYP2C8*3 also seems to be
important, although the effect might be blurred by other genotypes. We might
also speculate that it is important to evaluate the SNPs at each dosage and
infusion period, and that multiple pathways are involved, which leads to the
need for larger studies where the SNPs can be stratified or the usage of
multivariate analysis would be possible. Our study is small and we therefore
consider it a pilot study and the results need to be confirmed in larger patient
populations.
In Paper IV we found that patients with the ABCB1 genotype 2677G/A
had the highest clearance. These patients would then be expected to receive
the lowest exposure of paclitaxel and thereby the lowest anti-tumor effect. In
70 | RESULTS AND DISCUSSION
Paper II we found that patients carrying the T/A combination were good
responders. No G/A heterozygous patients were found in Paper II and no
patients with the T/A combination were found in Paper IV. The results
concerning the A-alleles in Paper II and Paper IV might be in contradiction to
each other, however, the only allele in common is the A-variant and the
effects might be influenced by the other allele. The effect might also be
dependent on the ABCB1 haplotypes in these patients or an association to
SNPs in other genes. In Paper IV patients carrying the T/T alleles had the
lowest clearance of paclitaxel as compared to the other genotypes, although
the difference was not statistically significant. These patients would then be
expected to have the highest exposure of paclitaxel and a high anti-tumor
activity, which would be in accordance with the higher response found in
Paper II. However, the correlation to the response might be due to an
influence both at the tumor site as well as an effect on the pharmacokinetics.
It is also likely that both the response and the pharmacokinetics of paclitaxel
are influenced by other factors.
Correlations between Paclitaxel Exposure, Response and
Genotypes of ABCB1, CYP2C8 and CYP3A4
In the prospective study (Paper IV) the toxicity was monitored in the
patients using the CTC scale version 2 and 23 patients underwent a more
extensive evaluation of the neurotoxicity both as Nscore (Cassidy et al. 1998)
and the patients’ own rating of their inconvenience. The tumor response was
evaluated as normalized CA-125 value prior to the fourth course of
chemotherapy and at the end of chemotherapy according to the RECISTcriteria.
The severity of the neurotoxicity at the final course of chemotherapy was
correlated with the AUC0-24h for paclitaxel as shown in Figure 19B (R = 0.48,
P = 0.02). No significant correlation could be found at first tumor evaluation,
after course 3 or 4, although there is a positive coefficient of the slope; see
Figure 19A (R = 0.24, P = 0.263). The inconvenience of the neurological
adverse events as evaluated by the patients’ own rating significantly correlated
to the exposure of paclitaxel at the first tumor evaluation but not at the final
course of chemotherapy (Figure 20). The motor neuropathy was increased in
RESULTS AND DISCUSSION | 71
Figure 19. Correlation between the exposure of paclitaxel (AUC0-24h) and the severity of
the neurotoxicity as evaluated using Nscore at A) the first tumor evaluation (course 3 or 4)
and at B) the final course of chemotherapy.
patients heterozygous for CYP2C8*3 (P = 0.034, data not shown). The
hematological toxicity was also associated with the CYP2C8*3 genotype,
especially the leukocytes (P = 0.067), neutrophils (P = 0.086) and platelets (P
= 0.02, see Table VII). Half of the CYP2C8*3 heterozygous patients (n = 3)
suffered extremely high hematological toxicity while the other half (n = 3) had
a minor effect on their blood counts as shown in Table VII. Whether this is
Figure 20. Correlation between the paclitaxel exposure (AUC0-24h) and the patients’ own
rating of their inconveniences due to neurological adverse effects at A) the first tumor
evaluation (course 3 or 4) and at B) the final course of chemotherapy.
72 | RESULTS AND DISCUSSION
related to the lower clearance of paclitaxel for these patients, a predisposition
of hematological toxicity or just occurred by chance could not be established.
Previous studies have found a correlation between a high paclitaxel exposure
and low blood counts (Gianni et al. 1995; Huizing et al. 1993). Although not
significant, patients with ABCB1 G2677T/A wild type seemed to have less
sensory neuropathy compared to patients with heterozygous or homozygous
mutations (P = 0.186, data not shown). For other adverse effects registered
using the CTC scale no linear correlations could be found between genotype
and toxicity.
Table VII. The distribution of haematological toxicity using the CTC grade in
patients carrying the CYP2C8*3 allele as compared to the rest of the patients.
Leukocyte
Toxicity
Grade 0
Grade 1
Grade 2
Grade 3
Grade 4
P = 0.067
CYP2C8*3 Neutrophile CYP2C8*3 Platelet
*1/*1 *1/*3 toxicity
*1/*1 *1/*3 toxicity
8
1
12
4
1
3
0
0
1
2
Grade 0
Grade 1
Grade 2
Grade 3
Grade 4
P = 0.086
4
4
6
7
5
3
0
0
0
3
Grade 0
Grade 1
Grade 2
Grade 3
Grade 4
P = 0.020
CYP2C8*3
*1/*1 *1/*3
15
10
1
0
0
2
1
2
1
0
In accordance with our results, Mielke et al. showed that the neurotoxicity is
associated with high paclitaxel exposure, especially the total exposure of the
drug (Mielke et al. 2005b). Neuropathy has also been shown to correlate to the
genotype of ABCB1. Patients wild type for C3435T did not develop
neuropathy as fast as other patients (Sissung et al. 2006). Although we did not
evaluate the neurotoxicity in the same way, we found a slight indication that
patients wild type for G2677T/A have less neurotoxicity than others. Since
the two SNPs are linked, this might be an indication of the involvement of
ABCB1 in the development of neurotoxicity after paclitaxel chemotherapy.
In Paper IV we could not find a correlation between the tumor response
and the genotypes of ABCB1, CYP2C8 or CYP3A4, although we found a
correlation in Paper II where patients homozygously mutated in G2677T/A
in the ABCB1 gene had a higher probability of responding to chemotherapy.
The discrepancy between the studies might be due to the different ways of
evaluating the response in the Papers, i.e. response at the end of
chemotherapy using the RECIST criteria and CA-125 values as compared to
RESULTS AND DISCUSSION | 73
progression-free survival. The study presented in Paper IV also included
about half the number of patients in the response analysis as compared to
Paper II and in the latter the significance only reaches the level of P < 0.05. It
is noteworthy that in Paper II only primary treated patients were included
while patients included in Paper IV were both previously treated and nontreated patients. However, in Paper IV we found a slight indication that wild
type patients had less neurotoxicity than other patients which might be an
indication of a higher P-gp transport in the blood-brain barrier and an
indication of the same mechanism as in Paper II.
In contradiction to the neurotoxic response, we found no correlation
between the AUC0-24h of paclitaxel and the tumor response. Previous studies
have shown a correlation of paclitaxel exposure and overall survival in
NSCLC patients (Huizing et al. 1997a) as well as the response at the end of
chemotherapy in advanced cancers (Mielke et al. 2005a). However, considering
that in Paper IV only a small number of patients (n=29) were eligible for
response analysis, including both previously non-treated and treated patients,
as mentioned above, and the impact of carboplatin, the significance might be
lost for the evaluation of the tumor response.
In summary, it seems as if the SNP G2677T/A in the ABCB1 gene
correlates to the pharmacokinetics of the drug as well as the response.
CYP2C8*3 seems to correlate with a lower clearance of paclitaxel in
accordance with in vitro findings although the clinical effect has not been as
clearly established. The exposure of paclitaxel also correlates to the
neurotoxicity after paclitaxel containing chemotherapy.
74 | RESULTS AND DISCUSSION
CONCLUSIONS
Based on the results from Papers I-IV, the following conclusions can be
drawn:
-
-
-
Mutations and polymorphisms in the β-tubulin gene M40 are rare,
especially in Caucasians, and unlikely to be a clinically relevant
resistance mechanism. In the original article concerning sequence
variations in the β-tubulin gene, a high frequency of mutations were
found which correlated to response. The results from our study show
that the use of paraffin-embedded material might explain the high
incidence of mutations in that study.
The SNP G2677T/A in the ABCB1 gene correlate to the response
evaluated one year after the end of paclitaxel-carboplatin
chemotherapy. The probability of responding to treatment is higher in
homozygously mutated patients (T/T or T/A) and there is a dosedependent influence from the number of mutated alleles on the
response to paclitaxel treatment. The G2677T/A SNP may be
important for the function of P-glycoprotein and resistance to
paclitaxel and provide useful information for individualized therapy.
The SNPs G2677T and C3435T in the ABCB1 gene are present in
linkage disequilibrium.
CONCLUSIONS | 75
-
-
-
-
A sensitive LC/MS method using a sonic spray ionization interface and
an ion trap mass spectrometer was developed for the simultaneous
quantification of paclitaxel and its hydroxymetabolites in human
plasma. The mobile phase contains TFA as a suppressor of Napaclitaxel ion formation in favor of the protonated ion which increases
the sensitivity and stabilizes the ionization. The method covers a wide
concentration range of paclitaxel suitable for the quantification of the
substances in clinical studies.
The SNPs G2677T/A in ABCB1 and CYP2C8*3 influence the
clearance of paclitaxel. This indicates that a patient’s individual
pharmacokinetics of paclitaxel might be predicted by determining the
genotype of ABCB1 and CYP2C8. The SNP G2677T/A in ABCB1
gene correlates to the pharmacokinetics of paclitaxel as well as the
response of paclitaxel containing treatment, indicating its importance in
paclitaxel pharmacogenetics. The correlation of CYP2C8*3 with a
lower clearance is in accordance with the in vitro activity of this enzyme
variant.
The exposure of paclitaxel correlates to the neurotoxicity as evaluated
by both Nscore and the patients’ own rating of their inconvenience due
to neurological adverse reactions.
The CYP3A4 enzyme activity in vivo did not affect the clearance of
paclitaxel but rather the metabolite pattern. A low CYP3A4 enzymatic
activity was correlated to a high 6α-hydroxypaclitaxel concentration
indicating a lower elimination of this metabolite or that a higher
fraction of paclitaxel was converted by CYP2C8.
76 | CONCLUSIONS
FUTURE ASPECTS
Pharmacogenetics and individualized treatment/medicine is expected to
become more and more important in the future as a way to improve and
predict the outcome of chemotherapy. Hopefully the findings in this thesis
will be part of the basic studies for individualization of paclitaxel-carboplatin
chemotherapy. The results presented here show that patients’ individual
elimination of paclitaxel might be predicted by determining the genotype of
ABCB1 and CYP2C8, which might be important parameters for
individualization of the paclitaxel dose. The studies also show that some
patients have a higher probability of responding to treatment and will benefit
from the regimen, while others might benefit from other chemotherapeutic
agents.
From our findings and other studies of β-tubulin mutations, we can
conclude that they are rare and probably not a clinically relevant resistance
mechanism and would probably not need any future investigation. On the
other hand the correlation of the ABCB1 genotype and the response to
paclitaxel-carboplatin chemotherapy needs to be further clarified. It would
probably be beneficial to investigate the distribution of SNPs in the ABCB1
gene in material from a larger uniformly treated population with a welldefined protocol for response evaluation to validate or rule out the ABCB1
genotype as a predictor of paclitaxel response. Hopefully these investigations
would not only include the SNPs studied in our report but others like
FUTURE ASPECTS | 77
G1199T/A in ABCB1 (which in vitro correlates to the resistance of paclitaxel)
and CYP2C8*3, which affect the clearance of the drug, as well as variations in
other genes to identify a “gene-profile” for patients that will benefit from
paclitaxel chemotherapy.
The quantification of paclitaxel and its metabolites in plasma would
probably be improved by an extraction method with a higher extraction ratio
and a more sensitive MS-instrument, the former being a matter of time and
the latter of money. However, the method developed suited our purposes for
the quantification of the substances in the pharmacogenetic study of
paclitaxel’s pharmacokinetics.
The correlation of the clearance of paclitaxel and the ABCB1 and CYP2C8
genotypes needs to be confirmed in an independent and larger
pharmacokinetic study. Hopefully this will lead to the development of
individualized dosage of paclitaxel. However, prior to that one needs to
establish a suitable target exposure and validate the impact of different
genotypes on the clearance and elimination of paclitaxel. It has previously
been suggested that a concentration of more than 50 nM of paclitaxel for at
least 20 hours or 100 nM for 15 hours is correlated to a good response to
paclitaxel-carboplatin treatment, although this has to be confirmed in future
studies. How much and in what way each genotype influences the clearance
and elimination of paclitaxel needs to be established using pharmacokinetic
modeling of data from clinical studies such as our pharmacokinetic
investigation. It will probably be possible to use physiologically based models
to construct a method for dose determination, where different variables can
be estimated both from physiological data from the patients such as weight
and height as well as SNP data from validated genotypes influencing the
elimination. However, there is still a long way to go before we can
individualize the dose of paclitaxel. Hopefully our studies will be a part of the
basic studies for this field of research.
78 | FUTURE ASPECTS
ACKNOWLEDGEMENTS
The studies in this thesis were conducted at the Division of Clinical
Pharmacology, Department of Medicine and Care, Faculty of Health Sciences,
Linköping University, Linköping, Sweden.
During the course of a project like this a great number of people have
made invaluable contributions both towards the work itself and in creating an
environment where it has been both possible to work and enjoy living in
moments of both triumph and disappointment. Despite my best intentions an
acknowledgement can never be more than a modest token of the gratitude
and esteem which I truly feel towards all those who have made this work
possible.
I wish to take the opportunity to express my sincere appreciation and
gratitude to all who contributed to this thesis, especially:
My supervisor, Professor Curt Peterson, for taking me under your wings
and letting me become one of your PhD student. For your outstanding
supervision, endless support, encouragement and for always taking the time to
discuss problems both large and small.
Professor Peter Söderkvist, my co-supervisor, for all the “genetic”
support, methodological and scientific discussions.
ACKNOWLEDGEMENTS | 79
The real patient doctor Per Rosenberg, my second co-supervisor, for
introducing me to the world of gynecological oncology, willingness to discuss
research and for making this thesis possible.
Malin Lindqvist, my officemate and (former) Phd student colleague for
fruitful discussions about anything and everything, a growing friendship and
not hitting me to many times going out and in of the office.
Björn Norlander for all the help with chromatography and for always
being there for me when I needed somebody to discuss methodology with. I
hope your new “occupation” will be as fruitful and enjoyable as possible for
you! You’re the best!
My new office-mate, Karin Skoglund, for putting up with me as a
supervisor and all the controls during your first project, for help with all the
other small lab projects and for all the discussions in the office.
Kourosh Lotfi, a good friend and colleague, for the time in Nice and for
our mutual effort in the quest for new knowledge and wild game.
Anna Fyrberg, Britt Sigfridsson, Anna-Lena Zackrisson and Gunilla
Graffner for a friendly atmosphere in the lab and all the help over the years.
Björn Carlsson and Maria Kingbäck, my fellow mass spectrometrists, for
all the time we’ve spent together disassembling and assembling the LC/MS.
Anita Thunberg for all the help with economic and administrative
matters, efficiently and swiftly as always.
All the rest of the staff and students at the Division of Clinical
Pharmacology – I hope I’ll have more time to help you with your computer
and technical problems in the future.
Martin Fransson, Ingemar Rundquist, Thomas Walz, Troels
Bergmann and Professor Kim Brøsen for present and future collaboration.
80 | ACKNOWLEDGEMENTS
My co-authors, Per Rymark, Karin Vretenbrant, György Horvath,
Rajaa Mirghani, and last but not least special thanks to Elisabeth ÅvallLundqvist for excellent reviews of both study design and manuscript as well
as scientific discussions.
Mats Borén and Johan Hurtig – for being good friends. I’ve always
enjoyed our scientific, non-scientific and “most-certainly” non-scientific
discussions in the sauna, in the stream, in the boat or over a barbeque.
All the research nurses who participated in the studies: Dagmar Gutemark
and Britt-Lena Staberg in Linköping, Susanne Skarps in Västerås, Ninni
Petersson and Anne Brandt in Stockholm, who monitored the patients,
cared about the study and took care of all the blood samples and a lot of
paperwork.
I am extremely lucky to have such a wonderful family that has supported
me during these years and I would therefore express my enormous gratitude
to them:
My parents, Ingvor and Krister Gréen, for their unconditional support
and endless encouragement to pursue new knowledge.
My one and only true love, Anna, for your endless love and encouragement
through rough times and tender moments. Our two children, Julia and
Linnea, for their endless and unconditional love. For always having time to
play with dad and hugging him when coming home from work and for their
aid in pushing the buttons on dad’s computer.
The studies presented in this thesis have financially been supported by the
Swedish Cancer Society, Gunnar Nilsson’s Cancer Foundation, the County
Council in Östergötland, the Anna Cederberg Foundation, Lions Foundation,
the Foundation for Strategic Research, Graduate School of Biomedical
Research and Faculty of Health Sciences, Linköping University.
ACKNOWLEDGEMENTS | 81
REFERENCES
Agarwal, R. and Kaye, S. B. (2003) Ovarian cancer: strategies for overcoming
resistance to chemotherapy. Nat Rev Cancer, 3: 502-516.
Alberts, B. (1994) Molecular biology of the cell. New York, Garland.
Alberts, D. S. and Dorr, R. T. (1998) New Perspectives on an Old Friend: Optimizing
Carboplatin for the Treatment of Solid Tumors. Oncologist, 3: 15-34.
Allen, J. D., Brinkhuis, R. F., van Deemter, L., Wijnholds, J., and Schinkel, A. H.
(2000) Extensive contribution of the multidrug transporters P-glycoprotein and Mrp1
to basal drug resistance. Cancer Res, 60: 5761-5766.
Alving, A. S., Carson, P. E., Flanagan, C. L., and Ickes, C. E. (1956) Enzymatic
deficiency in primaquine-sensitive erythrocytes. Science, 124: 484-485.
Andreeva, M., Niedmann, P. D., Binder, L., Armstrong, V. W., Meden, H., Binder, M.,
and Oellerich, M. (1997) A simple and reliable reverse-phase high-performance
liquid chromatographic procedure for determination of paclitaxel (taxol) in human
serum. Ther Drug Monit, 19: 327-332.
Anzenbacher, P. and Anzenbacherova, E. (2001) Cytochromes P450 and metabolism of
xenobiotics. Cell Mol Life Sci, 58: 737-747.
Ardrey, R. E. (2003) Liquid chromatography-mass spectrometry : an introduction. New
York, J. Wiley.
Arinobu, T., Hattori, H., Seno, H., Ishii, A., and Suzuki, O. (2002) Comparison of SSI
with APCI as an interface of HPLC-mass spectrometry for analysis of a drug and its
metabolites. Journal of the American Society for Mass Spectrometry, 13: 204-208.
82 | REFERENCES
Bahadur, N., Leathart, J. B., Mutch, E., Steimel-Crespi, D., Dunn, S. A., Gilissen, R.,
Houdt, J. V., Hendrickx, J., Mannens, G., Bohets, H., Williams, F. M., Armstrong,
M., Crespi, C. L., and Daly, A. K. (2002) CYP2C8 polymorphisms in Caucasians
and their relationship with paclitaxel 6alpha-hydroxylase activity in human liver
microsomes. Biochem Pharmacol, 64: 1579-1589.
Bakhtiar, R. and Nelson, R. W. (2000) Electrospray ionization and matrix-assisted laser
desorption ionization mass spectrometry: Emerging technologies in biomedical
sciences. Biochemical Pharmacology, 59: 891-905.
Berg, S. L., Tolcher, A., O'Shaughnessy, J. A., Denicoff, A. M., Noone, M., Ognibene,
F. P., Cowan, K. H., and Balis, F. M. (1995) Effect of R-verapamil on the
pharmacokinetics of paclitaxel in women with breast cancer. J Clin Oncol, 13: 20392042.
Bjorkman, H. T., Edlund, P.-O., and Jacobsson, S. P. (2002) Sonic spray ionization
interface for liquid chromatography-mass spectrometry. Analytica Chimica Acta,
468: 263-274.
Blagosklonny, M. V. and Fojo, T. (1999) Molecular effects of paclitaxel: myths and
reality (a critical review). Int J Cancer, 83: 151-156.
Bolis, G., Scarfone, G., Polverino, G., Raspagliesi, F., Tateo, S., et al. (2004) Paclitaxel
175 or 225 mg per meters squared with carboplatin in advanced ovarian cancer: a
randomized trial. J Clin Oncol, 22: 686-690.
Brinkmann, U., Roots, I., and Eichelbaum, M. (2001) Pharmacogenetics of the human
drug-transporter gene MDR1: impact of polymorphisms on pharmacotherapy. Drug
Discov Today, 6: 835-839.
Calvert, A. H., Newell, D. R., Gumbrell, L. A., O'Reilly, S., Burnell, M., Boxall, F. E.,
Siddik, Z. H., Judson, I. R., Gore, M. E., and Wiltshaw, E. (1989) Carboplatin
dosage: prospective evaluation of a simple formula based on renal function. J Clin
Oncol, 7: 1748-1756.
Cassidy, J., Paul, J., Soukop, M., Habeshaw, T., Reed, N. S., Parkin, D., and Kaye, S. B.
(1998) Clinical trials of nimodipine as a potential neuroprotector in ovarian cancer
patients treated with cisplatin. Cancer Chemother Pharmacol, 41: 161-166.
Choudhuri, S. and Klaassen, C. D. (2006) Structure, function, expression, genomic
organization, and single nucleotide polymorphisms of human ABCB1 (MDR1),
ABCC (MRP), and ABCG2 (BCRP) efflux transporters. Int J Toxicol, 25: 231-259.
REFERENCES | 83
Clayman, C. B., Arnold, J., Hockwald, R. S., Yount, E. H., Jr., Edgcomb, J. H., and
Alving, A. S. (1952) Toxicity of primaquine in Caucasians. J Am Med Assoc, 149:
1563-1568.
Cresteil, T., Monsarrat, B., Alvinerie, P., Treluyer, J. M., Vieira, I., and Wright, M.
(1994) Taxol metabolism by human liver microsomes: identification of cytochrome
P450 isozymes involved in its biotransformation. Cancer Res, 54: 386-392.
Crouthamel, M. H., Wu, D., Yang, Z., and Ho, R. J. (2006) A novel MDR1 G1199T
variant alters drug resistance and efflux transport activity of P-glycoprotein in
recombinant Hek cells. J Pharm Sci, 95: 2767-2777.
Dai, D., Zeldin, D. C., Blaisdell, J. A., Chanas, B., Coulter, S. J., Ghanayem, B. I., and
Goldstein, J. A. (2001) Polymorphisms in human CYP2C8 decrease metabolism of
the anticancer drug paclitaxel and arachidonic acid. Pharmacogenetics, 11: 597-607.
Daly, A. K. (2003) Pharmacogenetics of the major polymorphic metabolizing enzymes.
Fundam Clin Pharmacol, 17: 27-41.
Daly, A. K. (2004) Development of analytical technology in pharmacogenetic research.
Naunyn Schmiedebergs Arch Pharmacol, 369: 133-140.
Devita, V. T., Jr., Serpick, A. A., and Carbone, P. P. (1970) Combination chemotherapy
in the treatment of advanced Hodgkin's disease. Ann Intern Med, 73: 881-895.
Ding, X. and Kaminsky, L. S. (2003) Human extrahepatic cytochromes P450: function
in xenobiotic metabolism and tissue-selective chemical toxicity in the respiratory and
gastrointestinal tracts. Annu Rev Pharmacol Toxicol, 43: 149-173.
Druker, B. J. (2002) Perspectives on the development of a molecularly targeted agent.
Cancer Cell, 1: 31-36.
Dubois, D. and Dubois, E. (1916) A formula to estimate the approximate surface area if
height and weight be known. Arch Intern Med, 17: 863-871.
Eichelbaum, M., Ingelman-Sundberg, M., and Evans, W. E. (2006) Pharmacogenomics
and individualized drug therapy. Annu Rev Med, 57: 119-137.
Ettre, L. S. (1993) Nomenclature for chromatography. Pure & Appl. Chem., 65: 819872.
Evans, W. E. and McLeod, H. L. (2003) Pharmacogenomics--drug disposition, drug
targets, and side effects. N Engl J Med, 348: 538-549.
Felici, A., Verweij, J., and Sparreboom, A. (2002) Dosing strategies for anticancer
drugs: the good, the bad and body-surface area. Eur J Cancer, 38: 1677-1684.
Fellner, S., Bauer, B., Miller, D. S., Schaffrik, M., Fankhanel, M., Spruss, T., Bernhardt,
G., Graeff, C., Farber, L., Gschaidmeier, H., Buschauer, A., and Fricker, G. (2002)
84 | REFERENCES
Transport of paclitaxel (Taxol) across the blood-brain barrier in vitro and in vivo. J
Clin Invest, 110: 1309-1318.
Ferlini, C., Raspaglio, G., Mozzetti, S., Distefano, M., Filippetti, F., Martinelli, E.,
Ferrandina, G., Gallo, D., Ranelletti, F. O., and Scambia, G. (2003) Bcl-2 downregulation is a novel mechanism of paclitaxel resistance. Mol Pharmacol, 64: 51-58.
Ferrandina, G., Zannoni, G. F., Martinelli, E., Paglia, A., Gallotta, V., Mozzetti, S.,
Scambia, G., and Ferlini, C. (2006) Class III beta-tubulin overexpression is a marker
of poor clinical outcome in advanced ovarian cancer patients. Clin Cancer Res, 12:
2774-2779.
Fujimaki, S., Funato, T., Harigae, H., Fujiwara, J., Kameoka, J., Meguro, K., Kaku, M.,
and Sasaki, T. (2002) Quantitative analysis of a MDR1 transcript for prediction of
drug resistance in acute leukemia. Clin Chem, 48 (6 Pt 1): 811-817.
Garcia-Martin, E., Martinez, C., Tabares, B., Frias, J., and Agundez, J. A. (2004)
Interindividual variability in ibuprofen pharmacokinetics is related to interaction of
cytochrome P450 2C8 and 2C9 amino acid polymorphisms. Clin Pharmacol Ther,
76: 119-127.
Gelderblom, H., Baker, S. D., Zhao, M., Verweij, J., and Sparreboom, A. (2003)
Distribution of paclitaxel in plasma and cerebrospinal fluid. Anticancer Drugs, 14:
365-368.
Germann, U. A. (1996) P-glycoprotein--a mediator of multidrug resistance in tumour
cells. Eur J Cancer, 32A: 927-944.
Giannakakou, P., Poy, G., Zhan, Z., Knutsen, T., Blagosklonny, M. V., and Fojo, T.
(2000) Paclitaxel selects for mutant or pseudo-null p53 in drug resistance associated
with tubulin mutations in human cancer. Oncogene, 19: 3078-3085.
Giannakakou, P., Sackett, D. L., Kang, Y. K., Zhan, Z., Buters, J. T., Fojo, T., and
Poruchynsky, M. S. (1997) Paclitaxel-resistant human ovarian cancer cells have
mutant beta- tubulins that exhibit impaired paclitaxel-driven polymerization. J Biol
Chem, 272: 17118-17125.
Gianni, L., Kearns, C. M., Giani, A., Capri, G., Vigano, L., Lacatelli, A., Bonadonna,
G., and Egorin, M. J. (1995) Nonlinear pharmacokinetics and metabolism of
paclitaxel and its pharmacokinetic/pharmacodynamic relationships in humans. J Clin
Oncol, 13: 180-190.
Goh, B. C., Lee, S. C., Wang, L. Z., Fan, L., Guo, J. Y., Lamba, J., Schuetz, E., Lim, R.,
Lim, H. L., Ong, A. B., and Lee, H. S. (2002) Explaining interindividual variability
REFERENCES | 85
of docetaxel pharmacokinetics and pharmacodynamics in Asians through
phenotyping and genotyping strategies. J Clin Oncol, 20: 3683-3690.
Goldspiel, B. R. (1997) Clinical overview of the taxanes. Pharmacotherapy, 17: 110S125S.
Gonzalez-Garay, M. L., Chang, L., Blade, K., Menick, D. R., and Cabral, F. (1999) A
beta-tubulin leucine cluster involved in microtubule assembly and paclitaxel
resistance. J Biol Chem, 274: 23875-23882.
Goodsell, D. S. (2000) The molecular perspective: microtubules and the taxanes. Stem
Cells, 18: 382-383.
Goreva, O. B., Grishanova, A. Y., Mukhin, O. V., Domnikova, N. P., and Lyakhovich,
V. V. (2003) Possible prediction of the efficiency of chemotherapy in patients with
lymphoproliferative diseases based on MDR1 gene G2677T and C3435T
polymorphisms. Bull Exp Biol Med, 136: 183-185.
Gottesman, M. M. (2002) Mechanisms of cancer drug resistance. Annu Rev Med, 53:
615-627.
Gottesman, M. M. and Pastan, I. (1993) Biochemistry of multidrug resistance mediated
by the multidrug transporter. Annu Rev Biochem, 62: 385-427.
Green, H., Skoglund, K., Rommel, F., Bertilsson, L., and Lotfi, K. (2006) Influence of
CYP3A4 activity on imatinib response in patients with chronic myeloid leukemia.
11th Congress of the european hematology association, Amsterdam, The
Netherlands, pp. 63.
Gronlund, B., Hogdall, C., Hansen, H. H., and Engelholm, S. A. (2001) Results of
reinduction therapy with paclitaxel and carboplatin in recurrent epithelial ovarian
cancer. Gynecol Oncol, 83: 128-134.
Harris, J. W., Katki, A., Anderson, L. W., Chmurny, G. N., Paukstelis, J. V., and
Collins, J. M. (1994a) Isolation, structural determination, and biological activity of 6
alpha- hydroxytaxol, the principal human metabolite of taxol. J Med Chem, 37: 706709.
Harris, J. W., Rahman, A., Kim, B. R., Guengerich, F. P., and Collins, J. M. (1994b)
Metabolism of taxol by human hepatic microsomes and liver slices: participation of
cytochrome P450 3A4 and an unknown P450 enzyme. Cancer Res, 54: 4026-4035.
Hasegawa, S., Miyoshi, Y., Egawa, C., Ishitobi, M., Tamaki, Y., Monden, M., and
Noguchi, S. (2002) Mutational analysis of the class I beta-tubulin gene in human
breast cancer. Int J Cancer, 101: 46-51.
86 | REFERENCES
Heintz, A. P., Odicino, F., Maisonneuve, P., Beller, U., Benedet, J. L., Creasman, W. T.,
Ngan, H. Y., and Pecorelli, S. (2003) Carcinoma of the ovary. Int J Gynaecol Obstet,
83 Suppl 1: 135-166.
Hempel, G., Lehmkuhl, D., Krumpelmann, S., Blaschke, G., and Boos, J. (1996)
Determination of paclitaxel in biological fluids by micellar electrokinetic
chromatography. J Chromatogr A, 745: 173-179.
Henningsson, A., Marsh, S., Loos, W. J., Karlsson, M. O., Garsa, A., Mross, K., Mielke,
S., Vigano, L., Locatelli, A., Verweij, J., Sparreboom, A., and McLeod, H. L. (2005)
Association of CYP2C8, CYP3A4, CYP3A5, and ABCB1 polymorphisms with the
pharmacokinetics of paclitaxel. Clin Cancer Res, 11: 8097-8104.
Henriksson, R., Friberg, S., and Ringborg, U. (1998) Onkologi. Stockholm, Liber.
Hichiya, H., Tanaka-Kagawa, T., Soyama, A., Jinno, H., Koyano, S., et al. (2005)
Functional characterization of five novel CYP2C8 variants, G171S, R186X, R186G,
K247R, and K383N, found in a Japanese population. Drug Metab Dispos, 33: 630636.
Hirth, J., Watkins, P. B., Strawderman, M., Schott, A., Bruno, R., and Baker, L. H.
(2000) The effect of an individual's cytochrome CYP3A4 activity on docetaxel
clearance [see comments]. Clin Cancer Res, 6: 1255-1258.
Hockwald, R. S., Arnold, J., Clayman, C. B., and Alving, A. S. (1952) Toxicity of
primaquine in Negroes. J Am Med Assoc, 149: 1568-1570.
Hoffmeyer, S., Burk, O., von Richter, O., Arnold, H. P., Brockmoller, J., Johne, A.,
Cascorbi, I., Gerloff, T., Roots, I., Eichelbaum, M., and Brinkmann, U. (2000)
Functional polymorphisms of the human multidrug-resistance gene: multiple
sequence variations and correlation of one allele with P- glycoprotein expression and
activity in vivo. Proc Natl Acad Sci U S A, 97: 3473-3478.
Hopper-Borge, E., Chen, Z. S., Shchaveleva, I., Belinsky, M. G., and Kruh, G. D.
(2004) Analysis of the drug resistance profile of multidrug resistance protein 7
(ABCC10): resistance to docetaxel. Cancer Res, 64: 4927-4930.
Huizing, M. T., Giaccone, G., van Warmerdam, L. J., Rosing, H., Bakker, P. J., et al.
(1997a) Pharmacokinetics of paclitaxel and carboplatin in a dose-escalating and
dose-sequencing study in patients with non-small-cell lung cancer. The European
Cancer Centre. J Clin Oncol, 15: 317-329.
Huizing, M. T., Keung, A. C., Rosing, H., van der Kuij, V., ten Bokkel Huinink, W. W.,
Mandjes, I. M., Dubbelman, A. C., Pinedo, H. M., and Beijnen, J. H. (1993)
REFERENCES | 87
Pharmacokinetics of paclitaxel and metabolites in a randomized comparative study in
platinum-pretreated ovarian cancer patients. J Clin Oncol, 11: 2127-2135.
Huizing, M. T., Rosing, H., Koopmans, F. P., and Beijnen, J. H. (1998) Influence of
Cremophor EL on the quantification of paclitaxel in plasma using high-performance
liquid chromatography with solid-phase extraction as sample pretreatment. J
Chromatogr B Biomed Sci Appl, 709: 161-165.
Huizing, M. T., Sparreboom, A., Rosing, H., van Tellingen, O., Pinedo, H. M., and
Beijnen, J. H. (1995a) Quantification of paclitaxel metabolites in human plasma by
high- performance liquid chromatography. J Chromatogr B Biomed Appl, 674: 261268.
Huizing, M. T., van Warmerdam, L. J., Rosing, H., Schaefers, M. C., Lai, A.,
Helmerhorst, T. J., Veenhof, C. H., Birkhofer, M. J., Rodenhuis, S., Beijnen, J. H.,
and ten Bokkel Huinink, W. W. (1997b) Phase I and pharmacologic study of the
combination paclitaxel and carboplatin as first-line chemotherapy in stage III and IV
ovarian cancer. J Clin Oncol, 15: 1953-1964.
Huizing, M. T., Vermorken, J. B., Rosing, H., ten Bokkel Huinink, W. W., Mandjes, I.,
Pinedo, H. M., and Beijnen, J. H. (1995b) Pharmacokinetics of paclitaxel and three
major metabolites in patients with advanced breast carcinoma refractory to
anthracycline therapy treated with a 3-hour paclitaxel infusion: a European Cancer
Centre (ECC) trial. Ann Oncol, 6: 699-704.
Illmer, T., Schuler, U. S., Thiede, C., Schwarz, U. I., Kim, R. B., Gotthard, S., Freund,
D., Schakel, U., Ehninger, G., and Schaich, M. (2002) MDR1 gene polymorphisms
affect therapy outcome in acute myeloid leukemia patients. Cancer Res, 62: 49554962.
Ingelman-Sundberg, M. (2004) Pharmacogenetics of cytochrome P450 and its
applications in drug therapy: the past, present and future. Trends Pharmacol Sci, 25:
193-200.
Isla, D., Sarries, C., Rosell, R., Alonso, G., Domine, M., et al. (2004) Single nucleotide
polymorphisms and outcome in docetaxel-cisplatin-treated advanced non-small-cell
lung cancer. Ann Oncol, 15: 1194-1203.
Iyer, L. and Ratain, M. J. (1998) Pharmacogenetics and cancer chemotherapy. Eur J
Cancer, 34: 1493-1499.
Jamroziak, K., Mlynarski, W., Balcerczak, E., Mistygacz, M., Trelinska, J., Mirowski,
M., Bodalski, J., and Robak, T. (2004) Functional C3435T polymorphism of MDR1
88 | REFERENCES
gene: an impact on genetic susceptibility and clinical outcome of childhood acute
lymphoblastic leukemia. Eur J Haematol, 72: 314-321.
Jang, S. H., Wientjes, M. G., and Au, J. L. (2001) Kinetics of P-glycoprotein-mediated
efflux of paclitaxel. J Pharmacol Exp Ther, 298: 1236-1242.
Jones, N. A., Turner, J., McIlwrath, A. J., Brown, R., and Dive, C. (1998) Cisplatin- and
paclitaxel-induced apoptosis of ovarian carcinoma cells and the relationship between
bax and bak up-regulation and the functional status of p53. Mol Pharmacol, 53: 819826.
Kafka, A., Sauer, G., Jaeger, C., Grundmann, R., Kreienberg, R., Zeillinger, R., and
Deissler, H. (2003) Polymorphism C3435T of the MDR-1 gene predicts response to
preoperative chemotherapy in locally advanced breast cancer. Int J Oncol, 22: 11171121.
Kamazawa, S., Kigawa, J., Kanamori, Y., Itamochi, H., Sato, S., Iba, T., and Terakawa,
N. (2002) Multidrug resistance gene-1 is a useful predictor of Paclitaxel-based
chemotherapy for patients with ovarian cancer. Gynecol Oncol, 86: 171-176.
Karlsson, M. O., Molnar, V., Freijs, A., Nygren, P., Bergh, J., and Larsson, R. (1999)
Pharmacokinetic models for the saturable distribution of paclitaxel. Drug Metab
Dispos, 27: 1220-1223.
Kavallaris, M., Kuo, D. Y. S., Burkhart, C. A., Regl, D. L., Norris, M. D., Haber, M.,
and Horwitz, S. B. (1997) Taxol-resistant epithelial ovarian tumors are associated
with altered expression of specific beta-tubulin isotypes. J Clin Invest, 100: 12821293.
Kelley, M. J. (2002) RESPONSE: Re: Genetic Analysis of the -Tubulin Gene, TUBB,
in Non-Small-Cell Lung Cancer. J Natl Cancer Inst, 94: 777.
Kelley, M. J., Li, S., and Harpole, D. H. (2001) Genetic analysis of the beta-tubulin
gene, TUBB, in non-small-cell lung cancer. J Natl Cancer Inst, 93: 1886-1888.
Kemper, E. M., van Zandbergen, A. E., Cleypool, C., Mos, H. A., Boogerd, W.,
Beijnen, J. H., and van Tellingen, O. (2003) Increased penetration of paclitaxel into
the brain by inhibition of P-Glycoprotein. Clin Cancer Res, 9: 2849-2855.
Kenworthy, K. E., Bloomer, J. C., Clarke, S. E., and Houston, J. B. (1999) CYP3A4
drug interactions: correlation of 10 in vitro probe substrates. Br J Clin Pharmacol,
48: 716-727.
Kim, D. H., Park, J. Y., Sohn, S. K., Lee, N. Y., Baek, J. H., Jeon, S. B., Kim, J. G.,
Suh, J. S., Do, Y. R., and Lee, K. B. (2006) Multidrug resistance-1 gene
REFERENCES | 89
polymorphisms associated with treatment outcomes in de novo acute myeloid
leukemia. Int J Cancer, 118: 2195-2201.
Kim, R. B., Leake, B. F., Choo, E. F., Dresser, G. K., Kubba, S. V., Schwarz, U. I.,
Taylor, A., Xie, H. G., McKinsey, J., Zhou, S., Lan, L. B., Schuetz, J. D., Schuetz, E.
G., and Wilkinson, G. R. (2001) Identification of functionally variant MDR1 alleles
among European Americans and African Americans. Clin Pharmacol Ther, 70: 189199.
Kimchi-Sarfaty, C., Gribar, J. J., and Gottesman, M. M. (2002) Functional
characterization of coding polymorphisms in the human MDR1 gene using a vaccinia
virus expression system. Mol Pharmacol, 62: 1-6.
Kinirons, M. T., O'Shea, D., Kim, R. B., Groopman, J. D., Thummel, K. E., Wood, A.
J., and Wilkinson, G. R. (1999) Failure of erythromycin breath test to correlate with
midazolam clearance as a probe of cytochrome P4503A [see comments]. Clin
Pharmacol Ther, 66: 224-231.
Kioka, N., Tsubota, J., Kakehi, Y., Komano, T., Gottesman, M. M., Pastan, I., and
Ueda, K. (1989) P-glycoprotein gene (MDR1) cDNA from human adrenal: normal Pglycoprotein carries Gly185 with an altered pattern of multidrug resistance. Biochem
Biophys Res Commun, 162: 224-231.
Kivisto, K. T. and Kroemer, H. K. (1997) Use of probe drugs as predictors of drug
metabolism in humans. J Clin Pharmacol, 37: 40S-48S.
Klose, T. S., Blaisdell, J. A., and Goldstein, J. A. (1999) Gene structure of CYP2C8 and
extrahepatic distribution of the human CYP2Cs. J Biochem Mol Toxicol, 13: 289295.
Kohonen-Corish, M. R., Qin, H., Daniel, J. J., Cooper, W. A., Rivory, L., McCaughan,
B., Millward, M. J., and Trent, R. J. (2002) Lack of beta-tubulin gene mutations in
early stage lung cancer. Int J Cancer, 101: 398-399.
Konig, J., Cui, Y., Nies, A. T., and Keppler, D. (2000a) Localization and genomic
organization of a new hepatocellular organic anion transporting polypeptide. J Biol
Chem, 275: 23161-23168.
Konig, J., Cui, Y., Nies, A. T., and Keppler, D. (2000b) A novel human organic anion
transporting polypeptide localized to the basolateral hepatocyte membrane. Am J
Physiol Gastrointest Liver Physiol, 278: G156-164.
Kroetz, D. L., Pauli-Magnus, C., Hodges, L. M., Huang, C. C., Kawamoto, M., Johns,
S. J., Stryke, D., Ferrin, T. E., DeYoung, J., Taylor, T., Carlson, E. J., Herskowitz, I.,
Giacomini, K. M., and Clark, A. G. (2003) Sequence diversity and haplotype
90 | REFERENCES
structure in the human ABCB1 (MDR1, multidrug resistance transporter) gene.
Pharmacogenetics, 13: 481-494.
Kruglyak, L. and Nickerson, D. A. (2001) Variation is the spice of life. Nat Genet, 27:
234-236.
Kumar, G., Ray, S., Walle, T., Huang, Y., Willingham, M., Self, S., and Bhalla, K.
(1995) Comparative in vitro cytotoxic effects of taxol and its major human
metabolite 6 alpha-hydroxytaxol. Cancer Chemother Pharmacol, 36: 129-135.
Lamba, J. K., Lin, Y. S., Schuetz, E. G., and Thummel, K. E. (2002) Genetic
contribution to variable human CYP3A-mediated metabolism. Adv Drug Deliv Rev,
54: 1271-1294.
Lamendola, D. E., Duan, Z., Penson, R. T., Oliva, E., and Seiden, M. V. (2003) beta
tubulin mutations are rare in human ovarian carcinoma. Anticancer Res, 23: 681-686.
Letschert, K., Keppler, D., and Konig, J. (2004) Mutations in the SLCO1B3 gene
affecting the substrate specificity of the hepatocellular uptake transporter OATP1B3
(OATP8). Pharmacogenetics, 14: 441-452.
Leu, J. G., Chen, B. X., Schiff, P. B., and Erlanger, B. F. (1993) Characterization of
polyclonal and monoclonal anti-taxol antibodies and measurement of taxol in serum.
Cancer Res, 53: 1388-1391.
Lewin, B. (1990) Genes IV. Oxford, Oxford Univ. Press.
Liliemark, J. and Peterson, C. (1991) Pharmacokinetic optimisation of anticancer
therapy. Clin Pharmacokinet, 21: 213-231.
Linder, M. W., Prough, R. A., and Valdes, R., Jr. (1997) Pharmacogenetics: a laboratory
tool for optimizing therapeutic efficiency. Clin Chem, 43: 254-266.
Lindsay, S., Barnes, J., and Thames Polytechnic (1992) High performance liquid
chromatography : analytical chemistry by open learning. Chichester, Wiley on
behalf of Thames Polytechnic.
Lown, K. S., Thummel, K. E., Benedict, P. E., Shen, D. D., Turgeon, D. K., Berent, S.,
and Watkins, P. B. (1995) The erythromycin breath test predicts the clearance of
midazolam. Clin Pharmacol Ther, 57: 16-24.
Ludwig, A. H. and Kupryjanczyk, J. (2006) Does MDR-1 G2677T/A Polymorphism
Really Associate with Ovarian Cancer Response to Paclitaxel Chemotherapy? Clin
Cancer Res, 12: 6204.
Läkemedelsindustriföreningen (2006) FASS : förteckning över humanläkemedel.
Stockholm, Läkemedelsindustriföreningen (LIF).
REFERENCES | 91
Manfredi, J. J., Parness, J., and Horwitz, S. B. (1982) Taxol binds to cellular
microtubules. J Cell Biol, 94: 688-696.
Mano, Y., Kikuchi, Y., Yamamoto, K., Kita, T., Hirata, J., Tode, T., Ishii, K., and
Nagata, I. (1999) Bcl-2 as a predictor of chemosensitivity and prognosis in primary
epithelial ovarian cancer. Eur J Cancer, 35: 1214-1219.
Marchetti, P., Urien, S., Cappellini, G. A., Ronzino, G., and Ficorella, C. (2002) Weekly
administration of paclitaxel: theoretical and clinical basis. Crit Rev Oncol Hematol,
44 Suppl: S3-13.
Marsh, S., King, C. R., McLeod, H. L., Paul, J., Gifford, G., and Brown, R. (2006)
ABCB1 2677G>T/A genotype and paclitaxel pharmacogenetics in ovarian cancer.
Clin Cancer Res, 12: 4127; author reply 4127-4129.
Martello, L. A., Verdier-Pinard, P., Shen, H. J., He, L., Torres, K., Orr, G. A., and
Horwitz, S. B. (2003) Elevated levels of microtubule destabilizing factors in a Taxolresistant/dependent A549 cell line with an alpha-tubulin mutation. Cancer Res, 63:
1207-1213.
Martin, N., Catalin, J., Blachon, M. F., and Durand, A. (1998) Assay of paclitaxel
(Taxol) in plasma and urine by high-performance liquid chromatography. J
Chromatogr B Biomed Sci Appl, 709: 281-288.
Marx, D., Binder, C., Meden, H., Lenthe, T., Ziemek, T., Hiddemann, T., Kuhn, W.,
and Schauer, A. (1997) Differential expression of apoptosis associated genes bax and
bcl-2 in ovarian cancer. Anticancer Res, 17: 2233-2240.
Marzolini, C., Paus, E., Buclin, T., and Kim, R. B. (2004) Polymorphisms in human
MDR1 (P-glycoprotein): recent advances and clinical relevance. Clin Pharmacol
Ther, 75: 13-33.
Masica, A. L., Mayo, G., and Wilkinson, G. R. (2004) In vivo comparisons of
constitutive cytochrome P450 3A activity assessed by alprazolam, triazolam, and
midazolam. Clin Pharmacol Ther, 76: 341-349.
Mathijssen, R. H. and van Schaik, R. H. (2006) Genotyping and phenotyping
cytochrome P450: perspectives for cancer treatment. Eur J Cancer, 42: 141-148.
McGuire, W. P., Hoskins, W. J., Brady, M. F., Kucera, P. R., Partridge, E. E., Look, K.
Y., Clarke-Pearson, D. L., and Davidson, M. (1996) Cyclophosphamide and cisplatin
compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian
cancer. N Engl J Med, 334: 1-6.
Mesquita, B., Veiga, I., Pereira, D., Tavares, A., Pinto, I. M., Pinto, C., Teixeira, M. R.,
and Castedo, S. (2005) No significant role for beta tubulin mutations and mismatch
92 | REFERENCES
repair defects in ovarian cancer resistance to paclitaxel/cisplatin. BMC Cancer, 5:
101.
Meyer, U. A. (2000) Pharmacogenetics and adverse drug reactions. Lancet, 356: 16671671.
Meyer, U. A. (2004) Pharmacogenetics - five decades of therapeutic lessons from
genetic diversity. Nat Rev Genet, 5: 669-676.
Mielke, S., Sparreboom, A., Behringer, D., and Mross, K. (2005a) Paclitaxel
pharmacokinetics and response to chemotherapy in patients with advanced cancer
treated with a weekly regimen. Anticancer Res, 25: 4423-4427.
Mielke, S., Sparreboom, A., Steinberg, S. M., Gelderblom, H., Unger, C., Behringer, D.,
and Mross, K. (2005b) Association of Paclitaxel pharmacokinetics with the
development of peripheral neuropathy in patients with advanced cancer. Clin Cancer
Res, 11: 4843-4850.
Mirghani, R. A., Ericsson, O., Tybring, G., Gustafsson, L. L., and Bertilsson, L. (2003)
Quinine 3-hydroxylation as a biomarker reaction for the activity of CYP3A4 in man.
Eur J Clin Pharmacol, 59: 23-28.
Monsarrat, B., Alvinerie, P., Wright, M., Dubois, J., Gueritte-Voegelein, F., Guenard,
D., Donehower, R. C., and Rowinsky, E. K. (1993) Hepatic metabolism and biliary
excretion of Taxol in rats and humans. J Natl Cancer Inst Monogr, 15: 39-46.
Monsarrat, B., Chatelut, E., Royer, I., Alvinerie, P., Dubois, J., Dezeuse, A., Roche, H.,
Cros, S., Wright, M., and Canal, P. (1998) Modification of paclitaxel metabolism in a
cancer patient by induction of cytochrome P450 3A4. Drug Metab Dispos, 26: 229233.
Monzo, M., Rosell, R., Sanchez, J. J., Lee, J. S., O'Brate, A., Gonzalez-Larriba, J. L.,
Alberola, V., Lorenzo, J. C., Nunez, L., Ro, J. Y., and Martin, C. (1999) Paclitaxel
resistance in non-small-cell lung cancer associated with beta-tubulin gene mutations.
J Clin Oncol, 17: 1786-1793.
Monzo, M., Taron, M., and Rosell, R. (2002) Re: Genetic analysis of the beta-tubulin
gene, TUBB, in non-small-cell lung cancer. J Natl Cancer Inst, 94: 774-776;
discussion 777.
Morita, N., Yasumori, T., and Nakayama, K. (2003) Human MDR1 polymorphism:
G2677T/A and C3435T have no effect on MDR1 transport activities. Biochem
Pharmacol, 65: 1843-1852.
Mozzetti, S., Ferlini, C., Concolino, P., Filippetti, F., Raspaglio, G., Prislei, S., Gallo,
D., Martinelli, E., Ranelletti, F. O., Ferrandina, G., and Scambia, G. (2005) Class III
REFERENCES | 93
beta-tubulin overexpression is a prominent mechanism of paclitaxel resistance in
ovarian cancer patients. Clin Cancer Res, 11: 298-305.
Mutch, D. G. (2002) Surgical management of ovarian cancer. Semin Oncol, 29: 3-8.
Nakajima, M., Fujiki, Y., Kyo, S., Kanaya, T., Nakamura, M., Maida, Y., Tanaka, M.,
Inoue, M., and Yokoi, T. (2005) Pharmacokinetics of paclitaxel in ovarian cancer
patients and genetic polymorphisms of CYP2C8, CYP3A4, and MDR1. J Clin
Pharmacol, 45: 674-682.
Nakajima, Y., Yoshitani, T., Fukushima-Uesaka, H., Saito, Y., Kaniwa, N., et al. (2006)
Impact of the haplotype CYP3A4*16B harboring the Thr185Ser substitution on
paclitaxel metabolism in Japanese patients with cancer. Clin Pharmacol Ther, 80:
179-191.
Nicoletti, M. I., Valoti, G., Giannakakou, P., Zhan, Z., Kim, J. H., Lucchini, V.,
Landoni, F., Mayo, J. G., Giavazzi, R., and Fojo, T. (2001) Expression of betatubulin isotypes in human ovarian carcinoma xenografts and in a sub-panel of human
cancer cell lines from the NCI-Anticancer Drug Screen: correlation with sensitivity
to microtubule active agents. Clin Cancer Res, 7: 2912-2922.
Nieboer, P., de Vries, E. G., Mulder, N. H., and van der Graaf, W. T. (2005) Relevance
of high-dose chemotherapy in solid tumours. Cancer Treat Rev, 31: 210-225.
Niemi, M., Leathart, J. B., Neuvonen, M., Backman, J. T., Daly, A. K., and Neuvonen,
P. J. (2003) Polymorphism in CYP2C8 is associated with reduced plasma
concentrations of repaglinide. Clin Pharmacol Ther, 74: 380-387.
Obata, H., Yahata, T., Quan, J., Sekine, M., and Tanaka, K. (2006) Association between
single nucleotide polymorphisms of drug resistance-associated genes and response to
chemotherapy in advanced ovarian cancer. Anticancer Res, 26: 2227-2232.
Orita, M., Suzuki, Y., Sekiya, T., and Hayashi, K. (1989) Rapid and sensitive detection
of point mutations and DNA polymorphisms using the polymerase chain reaction.
Genomics, 5: 874-879.
Orr, G. A., Verdier-Pinard, P., McDaid, H., and Horwitz, S. B. (2003) Mechanisms of
Taxol resistance related to microtubules. Oncogene, 22: 7280-7295.
Parkin, D. M. and International Agency for Research on Cancer (2002) Cancer
incidence in five continents. Lyon, International agency for research on cancer.
Partheen, K., Levan, K., Osterberg, L., Helou, K., and Horvath, G. (2004) Analysis of
cytogenetic alterations in stage III serous ovarian adenocarcinoma reveals a
heterogeneous group regarding survival, surgical outcome, and substage. Genes
Chromosomes Cancer, 40: 342-348.
94 | REFERENCES
Pauli-Magnus, C. and Kroetz, D. L. (2004) Functional implications of genetic
polymorphisms in the multidrug resistance gene MDR1 (ABCB1). Pharm Res, 21:
904-913.
Penson, R. T., Oliva, E., Skates, S. J., Glyptis, T., Fuller, A. F., Jr., Goodman, A., and
Seiden, M. V. (2004) Expression of multidrug resistance-1 protein inversely
correlates with paclitaxel response and survival in ovarian cancer patients: a study in
serial samples. Gynecol Oncol, 93: 98-106.
Poelman, S. M., Adeyanju, M. O., Robertson, M. A., Recant, W. M., Karrison, T.,
Fleming, G. F., Olopade, O. I., and Conzen, S. D. (2000) Human breast cancer
susceptibility to paclitaxel therapy is independent of Bcl-2 expression. Clin Cancer
Res, 6: 4043-4048.
Poon, G. K., Wade, J., Bloomer, J., Clarke, S. E., and Maltas, J. (1996) Rapid screening
of taxol metabolites in human microsomes by liquid chromatography/electrospray
ionization-mass spectrometry. Rapid Commun Mass Spectrom, 10: 1165-1168.
Rahman, A., Korzekwa, K. R., Grogan, J., Gonzalez, F. J., and Harris, J. W. (1994)
Selective biotransformation of taxol to 6 alpha-hydroxytaxol by human cytochrome
P450 2C8. Cancer Res, 54: 5543-5546.
Rang, H. P., Dale, M. M., and Ritter, J. M. (1995) Pharmacology. Edinburgh, Churchill
Livingstone.
Robert, J., Morvan, V. L., Smith, D., Pourquier, P., and Bonnet, J. (2005) Predicting
drug response and toxicity based on gene polymorphisms. Crit Rev Oncol Hematol,
54: 171-196.
Rodenhuis, S. (2000) The status of high-dose chemotherapy in breast cancer.
Oncologist, 5: 369-375.
Rodriguez-Antona, C. and Ingelman-Sundberg, M. (2006) Cytochrome P450
pharmacogenetics and cancer. Oncogene, 25: 1679-1691.
Ronaghi, M., Uhlen, M., and Nyren, P. (1998) A sequencing method based on real-time
pyrophosphate. Science, 281: 363, 365.
Roses, A. D. (2000) Pharmacogenetics and the practice of medicine. Nature, 405: 857865.
Rowinsky, E. K., Cazenave, L. A., and Donehower, R. C. (1990) Taxol: a novel
investigational antimicrotubule agent. J Natl Cancer Inst, 82: 1247-1259.
Sakaeda, T., Nakamura, T., and Okumura, K. (2002) MDR1 genotype-related
pharmacokinetics and pharmacodynamics. Biol Pharm Bull, 25: 1391-1400.
REFERENCES | 95
Sale, S., Oefner, P. J., and Sikic, B. I. (2002a) Re: genetic analysis of the beta-tubulin
gene, TUBB, in non-small-cell lung cancer. J Natl Cancer Inst, 94: 776-777;
discussion 777.
Sale, S., Sung, R., Shen, P., Yu, K., Wang, Y., Duran, G. E., Kim, J.-H., Fojo, T.,
Oefner, P. J., and Sikic, B. I. (2002b) Conservation of the Class I {beta}-Tubulin
Gene in Human Populations and Lack of Mutations in Lung Cancers and Paclitaxelresistant Ovarian Cancers. Mol Cancer Ther, 1: 215-225.
Sanger, F., Nicklen, S., and Coulson, A. R. (1977) DNA sequencing with chainterminating inhibitors. Proc Natl Acad Sci U S A, 74: 5463-5467.
Schiff, P. B., Fant, J., and Horwitz, S. B. (1979) Promotion of microtubule assembly in
vitro by taxol. Nature, 277: 665-667.
Schiff, P. B. and Horwitz, S. B. (1980) Taxol stabilizes microtubules in mouse
fibroblast cells. Proc Natl Acad Sci U S A, 77: 1561-1565.
Sheffield, V. C., Beck, J. S., Kwitek, A. E., Sandstrom, D. W., and Stone, E. M. (1993)
The sensitivity of single-strand conformation polymorphism analysis for the
detection of single base substitutions. Genomics, 16: 325-332.
Sissung, T. M., Mross, K., Steinberg, S. M., Behringer, D., Figg, W. D., Sparreboom,
A., and Mielke, S. (2006) Association of ABCB1 genotypes with paclitaxel-mediated
peripheral neuropathy and neutropenia. Eur J Cancer.
Skipper, H., Schabel, J., and Wilcox, W. (1964) Experimental evaluation of potential
anticancer agents XIII: on the criteria and kinetics associated with 'curability' of
experimental leukemia. Cancer Treatment Reports, 55: 1-111.
Smith, D. A., Abel, S. M., Hyland, R., and Jones, B. C. (1998) Human cytochrome
P450s: selectivity and measurement in vivo. Xenobiotica, 28: 1095-1128.
Smith, N. F., Acharya, M. R., Desai, N., Figg, W. D., and Sparreboom, A. (2005)
Identification of OATP1B3 as a high-affinity hepatocellular transporter of paclitaxel.
Cancer Biol Ther, 4: 815-818.
Solus, J. F., Arietta, B. J., Harris, J. R., Sexton, D. P., Steward, J. Q., McMunn, C.,
Ihrie, P., Mehall, J. M., Edwards, T. L., and Dawson, E. P. (2004) Genetic variation
in eleven phase I drug metabolism genes in an ethnically diverse population.
Pharmacogenomics, 5: 895-931.
Sonneveld, P. (2000) Multidrug resistance in haematological malignancies. J Intern
Med, 247: 521-534.
96 | REFERENCES
Sonnichsen, D. S., Hurwitz, C. A., Pratt, C. B., Shuster, J. J., and Relling, M. V. (1994)
Saturable pharmacokinetics and paclitaxel pharmacodynamics in children with solid
tumors. J Clin Oncol, 12: 532-538.
Sonnichsen, D. S., Liu, Q., Schuetz, E. G., Schuetz, J. D., Pappo, A., and Relling, M. V.
(1995) Variability in human cytochrome P450 paclitaxel metabolism. J Pharmacol
Exp Ther, 275: 566-575.
Sottani, C., Turci, R., Micoli, G., Fiorentino, M. L., and Minoia, C. (2000) Rapid and
sensitive determination of paclitaxel (Taxol(R)) in environmental samples by highperformance liquid chromatography tandem mass spectrometry. Rapid Commun
Mass Spectrom, 14: 930-935.
Soyama, A., Hanioka, N., Saito, Y., Murayama, N., Ando, M., Ozawa, S., and Sawada,
J. (2002a) Amiodarone N-deethylation by CYP2C8 and its variants, CYP2C8*3 and
CYP2C8 P404A. Pharmacol Toxicol, 91: 174-178.
Soyama, A., Saito, Y., Hanioka, N., Murayama, N., Nakajima, O., Katori, N., Ishida, S.,
Sai, K., Ozawa, S., and Sawada, J. I. (2001) Non-synonymous single nucleotide
alterations found in the CYP2C8 gene result in reduced in vitro paclitaxel
metabolism. Biol Pharm Bull, 24: 1427-1430.
Soyama, A., Saito, Y., Komamura, K., Ueno, K., Kamakura, S., Ozawa, S., and Sawada,
J. (2002b) Five Novel Single Nucleotide Polymorfisms in the CYP2C8 Gene, One of
which Induces a Frame-shift. Drug Metabol Pharmacokin, 17: SNP7 (374) - SNP310
(377).
Sparreboom, A., Huizing, M. T., Boesen, J. J., Nooijen, W. J., van Tellingen, O., and
Beijnen, J. H. (1995a) Isolation, purification, and biological activity of mono- and
dihydroxylated paclitaxel metabolites from human feces. Cancer Chemother
Pharmacol, 36: 299-304.
Sparreboom, A., van Asperen, J., Mayer, U., Schinkel, A. H., Smit, J. W., Meijer, D. K.,
Borst, P., Nooijen, W. J., Beijnen, J. H., and van Tellingen, O. (1997) Limited oral
bioavailability and active epithelial excretion of paclitaxel (Taxol) caused by Pglycoprotein in the intestine. Proc Natl Acad Sci U S A, 94: 2031-2035.
Sparreboom, A., van Tellingen, O., Nooijen, W. J., and Beijnen, J. H. (1995b)
Determination of paclitaxel and metabolites in mouse plasma, tissues, urine and
faeces by semi-automated reversed-phase high-performance liquid chromatography.
J Chromatogr B Biomed Appl, 664: 383-391.
Sparreboom, A., van Zuylen, L., Brouwer, E., Loos, W. J., de Bruijn, P., Gelderblom,
H., Pillay, M., Nooter, K., Stoter, G., and Verweij, J. (1999) Cremophor EL-
REFERENCES | 97
mediated alteration of paclitaxel distribution in human blood: clinical
pharmacokinetic implications. Cancer Res, 59: 1454-1457.
Stephenson, F. (2002) A Tale of Taxol. Research in Review, 12: 16.
Sullivan, K. F. and Cleveland, D. W. (1986) Identification of conserved isotypedefining variable region sequences for four vertebrate beta tubulin polypeptide
classes. Proc Natl Acad Sci U S A, 83: 4327-4331.
Svojanovsky, S. R., Egodage, K. L., Wu, J., Slavik, M., and Wilson, G. S. (1999) High
sensitivity ELISA determination of taxol in various human biological fluids. J Pharm
Biomed Anal, 20: 549-555.
Tanabe, M., Ieiri, I., Nagata, N., Inoue, K., Ito, S., Kanamori, Y., Takahashi, M.,
Kurata, Y., Kigawa, J., Higuchi, S., Terakawa, N., and Otsubo, K. (2001) Expression
of P-glycoprotein in human placenta: relation to genetic polymorphism of the
multidrug resistance (MDR)-1 gene. J Pharmacol Exp Ther, 297: 1137-1143.
Taniguchi, R., Kumai, T., Matsumoto, N., Watanabe, M., Kamio, K., Suzuki, S., and
Kobayashi, S. (2005) Utilization of human liver microsomes to explain individual
differences in paclitaxel metabolism by CYP2C8 and CYP3A4. J Pharmacol Sci, 97:
83-90.
Teicher, B. A. (1994) Hypoxia and drug resistance. Cancer Metastasis Rev, 13: 139168.
The National Board of Health and Welfare Cancer Incidence in Sweden 2004. In: K.
Asplund and M. Rosén (eds.), Official Statistics of Sweden. Stockholm, 2005.
Theodoridis, G. and Verpoorte, R. (1996) Taxol analysis by high performance liquid
chromatography: A review. Phytochemical Analysis, 7: 169-184.
Thiebaut, F., Tsuruo, T., Hamada, H., Gottesman, M. M., Pastan, I., and Willingham,
M. C. (1987) Cellular localization of the multidrug-resistance gene product Pglycoprotein in normal human tissues. Proc Natl Acad Sci U S A, 84: 7735-7738.
Tirona, R. G. and Kim, R. B. (2002) Pharmacogenomics of organic anion-transporting
polypeptides (OATP). Adv Drug Deliv Rev, 54: 1343-1352.
Torres, K. and Horwitz, S. B. (1998) Mechanisms of Taxol-induced cell death are
concentration dependent. Cancer Res, 58: 3620-3626.
Totah, R. A. and Rettie, A. E. (2005) Cytochrome P450 2C8: substrates, inhibitors,
pharmacogenetics, and clinical relevance. Clin Pharmacol Ther, 77: 341-352.
Tsurutani, J., Komiya, T., Uejima, H., Tada, H., Syunichi, N., Oka, M., Kohno, S.,
Fukuoka, M., and Nakagawa, K. (2002) Mutational analysis of the beta-tubulin gene
in lung cancer. Lung Cancer, 35: 11-16.
98 | REFERENCES
Walle, T., Walle, U. K., Kumar, G. N., and Bhalla, K. N. (1995) Taxol metabolism and
disposition in cancer patients. Drug Metab Dispos, 23: 506-512.
van Asperen, J., van Tellingen, O., van der Valk, M. A., Rozenhart, M., and Beijnen, J.
H. (1998) Enhanced oral absorption and decreased elimination of paclitaxel in mice
cotreated with cyclosporin A. Clin Cancer Res, 4: 2293-2297.
Wang, D., Johnson, A. D., Papp, A. C., Kroetz, D. L., and Sadee, W. (2005a) Multidrug
resistance polypeptide 1 (MDR1, ABCB1) variant 3435C>T affects mRNA stability.
Pharmacogenet Genomics, 15: 693-704.
Wang, L. Z., Goh, B. C., Grigg, M. E., Lee, S. C., Khoo, Y. M., and Lee, H. S. (2003) A
rapid and sensitive liquid chromatography/tandem mass spectrometry method for
determination of docetaxel in human plasma. Rapid Commun Mass Spectrom, 17:
1548-1552.
Wang, T. H., Wang, H. S., and Soong, Y. K. (2000) Paclitaxel-induced cell death:
where the cell cycle and apoptosis come together. Cancer, 88: 2619-2628.
Wang, Y., O'Brate, A., Zhou, W., and Giannakakou, P. (2005b) Resistance to
microtubule-stabilizing drugs involves two events: beta-tubulin mutation in one
allele followed by loss of the second allele. Cell Cycle, 4: 1847-1853.
Wani, M. C., Taylor, H. L., Wall, M. E., Coggon, P., and McPhail, A. T. (1971) Plant
antitumor agents. VI. The isolation and structure of taxol, a novel antileukemic and
antitumor agent from Taxus brevifolia. J Am Chem Soc, 93: 2325-2327.
Vasey, P. A., Jayson, G. C., Gordon, A., Gabra, H., Coleman, R., Atkinson, R., Parkin,
D., Paul, J., Hay, A., and Kaye, S. B. (2004) Phase III randomized trial of docetaxelcarboplatin versus paclitaxel-carboplatin as first-line chemotherapy for ovarian
carcinoma. J Natl Cancer Inst, 96: 1682-1691.
Venter, J. C., Adams, M. D., Myers, E. W., Li, P. W., Mural, R. J., et al. (2001) The
sequence of the human genome. Science, 291: 1304-1351.
Whitten, D. L., Myers, S. P., Hawrelak, J. A., and Wohlmuth, H. (2006) The effect of St
John's wort extracts on CYP3A: a systematic review of prospective clinical trials. Br
J Clin Pharmacol, 62: 512-526.
Wiernik, P. H., Schwartz, E. L., Strauman, J. J., Dutcher, J. P., Lipton, R. B., and
Paietta, E. (1987) Phase I clinical and pharmacokinetic study of taxol. Cancer Res,
47: 2486-2493.
Yamaguchi, H., Hishinuma, T., Endo, N., Tsukamoto, H., Kishikawa, Y., Sato, M.,
Murai, Y., Hiratsuka, M., Ito, K., Okamura, C., Yaegashi, N., Suzuki, N., Tomioka,
Y., and Goto, J. (2006) Genetic variation in ABCB1 influences paclitaxel
REFERENCES | 99
pharmacokinetics in Japanese patients with ovarian cancer. Int J Gynecol Cancer, 16:
979-985.
Yamamoto, N., Tamura, T., Murakami, H., Shimoyama, T., Nokihara, H., Ueda, Y.,
Sekine, I., Kunitoh, H., Ohe, Y., Kodama, T., Shimizu, M., Nishio, K., Ishizuka, N.,
and Saijo, N. (2005) Randomized pharmacokinetic and pharmacodynamic study of
docetaxel: dosing based on body-surface area compared with individualized dosing
based on cytochrome P450 activity estimated using a urinary metabolite of
exogenous cortisol. J Clin Oncol, 23: 1061-1069.
Yeh, J. J., Hsu, W. H., Wang, J. J., Ho, S. T., and Kao, A. (2003) Predicting
chemotherapy response to paclitaxel-based therapy in advanced non-small-cell lung
cancer with P-glycoprotein expression. Respiration, 70: 32-35.
Zhao, J., Kim, J. E., Reed, E., and Li, Q. Q. (2005) Molecular mechanism of antitumor
activity of taxanes in lung cancer (Review). Int J Oncol, 27: 247-256.
100 | REFERENCES