Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
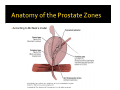
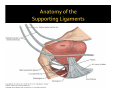
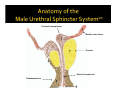
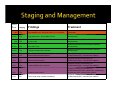
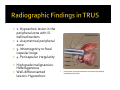
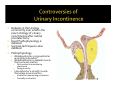
1 Luis Ramos Harvard Medical School BIDMC Department of Radiology Class of 2011 Index Case Relevant Anatomy Basic Facts of Prostate Cancer Menu of Radiologic Tests for the Evaluation and Diagnosis Role of Radical Prostatectomy Discussion of Urinary Incontinence Conclusion CC: Elevated PSA HPI: Mr. SR is a 67 year old male s/p standard radical prostatectomy, s/p salvage radiotherapy one yr later that presents with a rising PSA from 2.4 to 3.7. Pt has been complaining of urinary incontinence, as he wears 4 diapers a day. ROS: Not significant for bone pain, back pain, dysuria, urinary frequency PMH: HTN Hypercholesterolemia Leiomyoma in Gastric esophageal junction Allergies: Penicillin MEDS: Allegra, Hctz, Simvastatin, Detrol, Aleve FH: Sister died of ovarian cancer, mother died of unknown metastatic cancer According to McNeal’s model Proximal Lissosphincter Bladder musculature Prostate Distal Lissosphincter Rhabdosphincter Most common neoplasm among men Incidence: 119 per 100,000 2nd most common cause of death due to cancer 95% of tumors are adenomcarcinomas Primarily arises from peripheral (transition zone) Increased risk: Genetic African American Dietary (High fats) Environmental Hormonal Controversies Traditional screening guidelines PSA levels >10 ng/mL for men age >40 OR Digital rectal exam: Palpable rock hard nodule If any of these found they were sent for TRUS‐guided biopsy Unfortunately, PSA levels never correlated with a reduction in cancer mortality and potentially led to overdiagnosis and overtreatment of otherwise benign tumors New American Urologic Association guidelines as of 2009 included the following changes: 1. PSA testing offered to well‐ informed patients age>40 with a life expectancy >10 years 2a. Routine bone scan is not required 2b. However, bone scans are indicated for the detection of mets following initial treatment of disease 3. CT or MRI may be considered for staging when PSA <20 ng/mL 15yr Recurren ce Survival Staging Findings Treatment T1a Non-palpable tumor; low grade cancer <5% of prostate Observation T1b High grade tumor; >5% prostate involved Radical Prostatectomy/ External Beam Radiation/ Brachytherapy T2a 1 lobe or less Radical Prostatectomy/ External Beam Radiation/ Brachytherapy 60-70% T2b More than 1 lobe Radical Prostatectomy/ External Beam Radiation/ Brachytherapy 20-60% T3a Unilateral Extraprostatic Extension Radical Prostatectomy/ External Beam Radiation/ Brachytherapy 0-10% T3b Bilateral Extraprostatic Extension Hormonal Therapy (Orchioectomy OR LHRH/Antiandrogen) + external beam radiation 0-10% T3c Seminal Vesicle Invasion Hormonal Therapy (Orchioectomy OR LHRH/Antiandrogen) + external beam radiation 0-10% T4a Invades Bladder Neck or Rectum Hormonal Therapy (Orchioectomy OR LHRH/Antiandrogen) + external beam radiation 100% 70-80% 85% 0-10% T4b Invades Levator muscle Hormonal Therapy (Orchioectomy OR LHRH/Antiandrogen) when symptomatic; irradiation for isolated bone pain+ external beam radiation 0-10% M+ Pelvic lymph node or distant metastases Hormonal Therapy (Orchioectomy OR LHRH/Antiandrogen) + external beam radiation Trans‐rectal Ultrasonography Doppler TRUS Endorectal MRI Axial CT Bone Scan Antibody Imaging http://www.upmccancercenters.com/cancer/prostate/b iopsyultrasound.html Borlev et al: Most common diagnostic modality2 Primary role is for tissue diagnosis: 12 core needle biospy Hypoechoic lesions (traditionally) Only 20% of hypoechoic lesions prove to be cancer on biopsy No t recommended for screening Patient Prep: Fleet enema 4 hrs prior to exam Antibiotic (Cephalexin) if biopsy Indications: Elevated PSA or PSA velocity Previous biopsies showing intraepithelial neoplasia (PIN) or small acinar proliferation (ASAP) Contraindications: Elderly or frail men Massively elevated PSA with abnormal DRE Turkbey et al Drawbacks: ▪ Low sensitivity and specifcity ▪ Small foci are often not visible3 1. Hypoechoic lesion in the peripheral zone with ill‐ defined borders 2. Assymetrical peripheral zone 3. Inhomogenity or focal capsular bulge 4. Pericapsular irregularity High grade malignancies: Heterogeneous Well‐differenianted lesions: Hypoechoic http://www.upmccancercenters.com/cancer/prostate/b iopsyultrasound.html Example 1 http://www.upmccancercenters.com/cancer/prostate/b iopsyultrasound.html Example 2 : http://emedicine.medscape.com/article/457757‐overview Calcifications Right lobe Left Lobe Hypoechoic lesion Hypoechoic lesions near the peripheral zone11 Chronic or Acute Prostatitis Benign Prostate Hypertrophy (although it would more likely appear in the periurethral zone) Prostate carcinoma including adenocarcinoma Endorectal coil Accuracy ranges from 51% to 92% T2 weighted image is the test of choice Medical device used to obtain high quality images in the organs of the pelvis improves cancer detection and staging Indications: Staging of known prostate cancer Guidance for radiation implant placement Contraindications: Incompatible devices Prep NPO 6 hrs prior IM Glucagon to decrease intestinal motility Limited availability of MRI Obese pts may not fit Sensitivity to motion limits uncooperative pts Insensitive to subtle calcifications or small bony fragments T2 weighted image is the test of choice Peripheral zone Prostatitis Infarcts Stromal BPH Low intensity signal in cancer High intensity signal in normal Central zone Low signal intensity normally Cancer is difficult to find in this area DDx of Low intensity in central zone Staging Factors: Direct Extension through12: Tumor capsule (T3a) Periprostatic fat (T3b) Neurovascular bundles (T3b) Seminal Vescicles (T3c) Metastasis to pelvic lymph nodes (M+) Bladder Prostate cancer located in the Periurethral zone Urethra Prostate 4 T2 coronal Purpose is to exclude lymph node mestastases in high risk patients If adenopathy is detected, then CT‐guided biosy is encouraged Sensitivity is low and varied (30‐40%) Indications: Previously detected negative bone scan Stage T3 cancers PSA >20 ng/mL Drawbacks: Poor soft tissue resolution Not widely used Not used routine for follow up Ionizing radiation Overall not helpful 5. http://emedicine.medscape.com/article/379996-media Given his radiologic findings in Endorectal MRI, it was omnious for recurrence Staging T3c Given that he is s/p radical prostatectomy and s/p brachytherapy, Hormonal Therapy would probably be warranted at this time Nerve‐sparing dissection of the apical neck bladder with lymph node dissection Goals: complete removal of the prostate gland along with surrounding tissue Tumor margins as negative as possible Modalities Open approach Laparoscopy Robotic‐Assisted Indications: cT1b and cT27 ▪ T1: Non‐palpable tumor , high grade tumor >5% involved ▪ T2: Tumor involving 1 lobe or less cT3: controversy6 ▪ Unilateral extraprostatic extension7 ▪ Usually involves radiotherapy, Hill 2007 would argue in certain cases it is clinically warranted Loughlin et al Urinary Incontinence Incidence: up to 69%8 Emotionally disturbing Severe morbidity Up to 90% gain function within 24 months depending on which study Patient Age Older men have thinner rhabdomyosphincter Higher BMI Pre‐OP ED Preo‐OP voiding dysnfunction Gleason score Prior TURP Debates in the Urology community over what is the exact etiology of urinary incontinence after radical prostatectomy Exact Pathophysiology is debated Surgical techniques is also debated Pathophysiology ▪ ▪ ▪ Rhabdosphincter vs Lissosphincter according to Koraitim10 Rhabdosphincter is skeletal muscle that surrounds urethra Not involved in maintaining continence Fatigues easily Lissosphincter is smooth muscle that wraps around urethra Involved in maintaining continence Tonically contracted Puboprostatic Ligament sparing surgery Steiner et al 13 Advocates in order to optimize urethral length and leave the anterior support of the urethra Poore et al14 Rapid return to continence in the puboprostatic ligament sparing group (34 vs 57 wks in the control group Deliveliotis et al15 Found no difference in the puboprostatic ligament sparing group, bladder neck preservation or having both procedures in the length of continence recovery Seminal vescicle sparing Hauri et al16 Pelvic nerve transverses rhabdosphincter and supplies smooth muscle (lissosphincter) Reports continence rates of 95% after 6 months in the seminal vescicle spare group versus 85% in controls Given the relapse of Mr. RS does it really matter to discuss urinary incontinence? If we approach as a life of quality issue Should a different surgical approach have been taken? Should puboprostatic ligament sparing and seminal vescicle sparing techniques have been implemented? More fundamentally What might be the relative effectiveness between radical prostatectomy, brachytherapy and external beam radiation? Which approach should be attempted first? Second? Prostate Cancer is a very common neoplasm among men, 2nd deadliest Work up involves changes in PSA or palpable hard rock nodule in the prostate This is followed by TRUS that guides biopsy Hypoechoic lesion in the peripheral zone suggests cancer Hypoechoic lesion in the transition zone suggests BPH If carcinoma is present, Endorectal MRI is used for staging and surgical planning T2 hypointense signal in the peripheral zone suggests carcinoma If contraindications, CT may be used Depending on TNM staging (T1b‐T3a) one may opt for radical prostatectomy, brachytherapy and external beam radiation Radical prostatectomy has side effects that include urinary incontinence Causes of urinary incontinence are debated in the literature Factors: Age, BMI, pre‐op function, s/p TURP Koraitim proposes lissosphincter model as a way to maintain continence Different surgical techniques Olga Brook, MD Gillian Lieberman, MD Maria Levantakis 1. http://www.turbosquid.com/FullPreview/Index.cfm/ID/233868 2. Prostate cancer: diagnosis and staging Nigel Borley, Mark R. Feneley http://www.ultrasound‐images.com/prostate.htm 4. Incremental Value of Multiplanar Cross‐Referencing for Prostate Cancer Staging with Endorectal MRI 3. Imaging techniques for prostate cancer: implications for focal therapy. Baris Turkbey, Peter A. Pinto and Peter L. Choyke 5. http://emedicine.medscape.com/article/379996‐media 6. Radical prostatectomy for clinical T3 disease: expanding indications while optimizing cancer control and quality of life Jennifer R Hill, Samson W Fine, Jingbo Zhang and James A Eastham 7. CURRENT Diagnosis & Treatment: Surgery > Chapter 38. Urology > Tumors of the Genitourinary Tract > Carcinoma of the Prostate > Clinical Findings > Symptoms and Signs > 8. Wei JT, Dunn RL, Marcovich R et al: Prospective assessment of patient reported urinary continenceradical prostatectomy. J Urol 2000; 164:744. 9. Post‐Prostatectomy Urinary Incontinence: A Confluence of 3 Factors Kevin R. Loughlin* and Michaella M. Prasad† 10. The Male Urethral Sphincter Complex Revisited: An Anatomical Concept and its Physiological Correlate Mamdouh M. Koraitim 11. Hypoechoic Rim of Chronically Inflamed Prostate, as Seen at TRUS: Histopathologic Findings Hak Jong Lee, MD,1 Ghee Young Choe, MD,2 Chang Gyu Seong, MD,3 and Seung Hyup Kim, MD4 12. CURRENT Diagnosis & Treatment: Surgery > Chapter 38. Urology > Tumors of the Genitourinary Tract > Carcinoma of the Prostate > Clinical Findings > Symptoms and Signs > 13. Steiner MS: The puboprostatic ligament and the male urethral suspensory mechanism: an anatomic study. Urology 1994; 44: 530. 14. Poore RE, McCullough DL and Jarow JP: Puboprostatic ligament sparing improves urinary continence after radical retropubic prostatectomy. Urology 1998; 51: 67. 15. Deliveliotis C, Protogerou V, Alargof E et al:Radical prostatectomy: bladder neck preservation and puboprostatic ligament sparing— effects on continence and positive margins. Urology 2002;60: 855. 16. John H and Hauri D: Seminal vesicle‐sparing radical prostatectomy: a novel concept to restore early urinary continence. Urology 2000; 55: 820.