Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
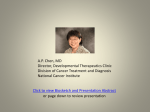
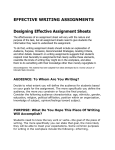
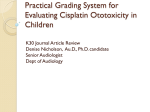
WUSS 2011 - Paper 74961 Analyze This? Supporting Clinical Decisions Graphically When Not Enough Data is Available A Study Case: Challenges in NCI CTCAE Version 4 Grading Sheila Dayog, Genentech, a Member of the Roche Group, South San Francisco, CA ABSTRACT Working with laboratory clinical data is challenging enough, but another challenge has arisen when applying the updated National Cancer Institute Common Terminology Criteria, Version 4.0 for Adverse Events (NCI CTCAE). Version 4.0 incorporates stronger clinical observation into the some of the laboratory grading descriptions, thus removing straight forward range-based numeric algorithms. Additionally, these observations can present themselves a number of ways and the task of programmatic laboratory grade assignment whilst considering these assessments offers challenges. Potential for inconsistent grading exists, possibly leading to incorrect clinical data interpretation. This paper will discuss these challenges, offering the use of SAS® graphics data visualization to assist in identifying any discordant relationships between laboratory grade assignments and the adverse event grades that occur throughout the conduct of an oncology clinical trial. INTRODUCTION An adverse event (AE) is described by the Common Terminology Criteria as “any unfavorable and unintended sign (including an abnormal laboratory finding), symptom, or disease temporally associated with the use of a medical treatment or procedure that may or may not be considered related to the medical treatment or procedure.” Generally speaking, the collection of adverse events is required during the conduct of all phases of an oncology clinical trial. In phase I trials, commonly referred to as “first-in-man” studies, the primary endpoint is entirely based on evaluating adverse events. These events are supported by laboratory evidence in determining a recommended safe dose and the decision is dependent upon the proper evaluation of toxicity levels. As drug development passes from early phase into later-stage development, the overall safety assessments continue to be closely monitored. One of the methods for measuring these assessments is to characterize severity by applying a grading scale developed by the Common Toxicity Criteria by the US National Cancer Institute (NCI CTC). The severity scale ranges from a “mild” event to “death”, categorized 1 thru 5 accordingly. NCI CTCAE VERSION 4.0 CLINICAL DATA CHALLENGES Uncertainty of laboratory grading surfaced when version 4.0 criteria required investigator clinical assessment as input into the overall grade determination. Dependencies upon clinical assessments found in multiple data sources like physical examinations, concomitant medications, adverse events, vital signs, and laboratory results makes programmatic approaches challenging, subject to varying sponsor approaches and inconsistency in overall severity categorization. Interrelating events amongst these data domains is tricky, dependent upon many factors like the overall data collection, the reconciling of the assessment dates within a defined visit window, or the unfortunate consideration of free-text fields which may contain relevant information. The Cancer Therapy Evaluation Program (CTEP) within the NCI reviewed each CTCAE v4.0 term for which the grading scale included a quantitative component. Guidance was put forth, identifying 26 events where investigator input is required. An example of Anemia guidance is listed below, highlighting the areas difficult to programmatically consider. CTCAE v4.0 Term Anemia Grade 1 Grade 2 Grade 3 Hemoglobin (Hgb) <LLN - 10.0 g/dL; <LLN - 6.2 mmol/L; <LLN - 100 g/L Hgb <10.0 8.0 g/dL; <6.2 - 4.9 mmol/L; <100 - 80g/L Hgb <8.0 g/dL; <4.9 mmol/L; <80 g/L; transfusion indicated Grade 4 Lifethreatening consequences; urgent intervention indicated CTCAE v4.0 AE Term Definition A disorder characterized by an reduction in the amount of hemoglobin in 100 ml of blood. Signs and symptoms of anemia may include pallor of the skin and mucous membranes, shortness of breath, palpitations of the heart, soft systolic murmurs, lethargy, and fatigability. Figure 1. CTEP Guidance: CTCAE v4.0 Grading Scales with Numeric Component 1 In noting the highlighted text above, difficulties can occur in relating the partial criteria of “transfusion indicated” in the concomitant medications data collection, for example. Additionally, general signs and symptoms of “pallor of the skin and mucous membranes, lethargy, and fatigability” may or may not be collected in the physical examination data. “Palpitations of the heart” could be recorded in the vital signs collection as tachycardia, cardiac arrhythmia, or in the form of an abnormal ECG assessment. These general characterizations can be easily assessed by the on-site investigator for which all can factor into the overall assignment of grade 4. Applying programmatic algorithms, however, to include these assessments is very difficult. Noted in the above criterion for grade 4, there is simply no numeric algorithm in which to measure the test result. Furthermore, when studying a fairly sick subject population, it is difficult to programmatically ascertain whether the reported assessments are or are not related to the actual adverse event in question. Awareness of these challenges alert programmers to the fact that grading discrepancies exist. Solutions are difficult and are highly dependent upon the overall setup of the data collection and overall reporting. In exploring these challenges, graphical displays can be useful in quickly identifying where gaps exist. While solutions to this problem are not discussed, the simple identification of areas requiring further scrutiny of the data to better support clinical decision making can be supported. GRAPHIC ILLUSTRATION OF LABORATORY DISCORDANCE All graphics displayed were generated using the SAS® 9.2 ODS Graphics Designer to produce quick and easy results. Additionally, SAS® Graph Template Language (GTL) template code was created, enabling a programmer to reproduce the code outside of the designer interface, allowing for simple reusability. Firstly, let us consider the previous NCI CTCAE Version 3.0 grading scale where clear numeric algorithms were straightforward in application. There are some discrepancies easily noted in the Hemoglobin results for Anemia, but by in large, there is very little discordance between investigator assigned grades and the programmatically calculated grades from the sponsor. These panel graphics were created by utilizing the “add column” function within the Graphics Designer. Other components offering ease of use include drop-and-drag functionality to allow overlay of four plots in total. Figure 2. Illustration of minimal discordance using version 3.0 where clinical input was not required. 2 Next, let us view Hemoglobin results from a protocol mandating the version 4.0 grading scale. This example illustrates strong discordance between the investigative sites who conducts the clinical evaluation of the patient, versus the programmatic laboratory grading assignments from the sponsoring organization. It is not difficult to identify these discrepancies and in fact, all cases assessed by the sponsor were assigned to grade 1. The investigator reported a very different picture, with only two events being reported as a grade 1. The most extreme case is that of the “Life-threatening” grade 4 investigator finding, unable to be replicated by laboratory results alone. Figure 3. Illustration of notable discordance using version 4.0 where clinical input was required. Now that clear discrepancies have been identified, the subject that had the two-point grading difference was quickly identified and further examined. Referring back to the adverse event grading guidance for Anemia (Figure 1.), scrutiny of the clinical assessment data resulted in the following: • Vital signs: The subject did not present with any abnormal vitals signs (e.g., shortness of breath or any indication of heart palpitations). • Concomitant medications or interventional therapy: The subject did receive a blood transfusion; however the reported transfusion administration date fell just outside of the protocol-defined amount of time for which assessments can be considered “related” to the particular adverse event in question. • Life-threatening consequences or urgent interventions: Hospitalization was the action taken in response to this particular event, as indicated in the adverse event data domain. This information may qualify for grade 4 criterion of “urgent intervention indicated”. As this particular data point was not part of the programming algorithm, the resulting sponsor defined “mild” grade 1 differed greatly from the investigators “life-threatening” grade 4 finding. Furthermore, as one may recall from the CTEP guidance on Anemia, it provided no numeric component for grade 4 categorization. In this case, grade 4 laboratory results measuring Hemoglobin make for unlikely sponsor-defined replication of the investigator grade assignment. 3 CONCLUSION Safety data collection is a key component in drug development. Without proper safety assessments and reporting, drug development cannot move forward, ultimately affecting the approval of a safe and efficacious therapeutic. During Phase I clinical trials, dose limiting toxicities are the primary endpoints which reflect the side effects during treatment that are severe enough to prevent an increase in dosage or even halt study drug administration. Decisionmaking to dose escalate are entirely dependent upon the analysis of these safety events. Subsequent maximum tolerated doses are determined which identify safe dosing levels for later-stage development. Without accurate and proper interpretation, clinical decision-making is jeopardized. In recognizing real potential for grading differences, sponsors should be more vigilant in data review. Graphical illustration offers a tool to assist decision making, at the very least, identifying trends where further investigation is warranted. REFERENCES National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0 http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf National Cancer Institute. CTEP Guidance: CTCAE v4.0 Grading Scales with Numeric Component http://evs.nci.nih.gov/ftp1/CTCAE/About.html Rodriguez, Robert N. 2008. "Getting Started with ODS Statistical Graphics in SAS 9.2.” Proceedings of the SAS Global Forum 2008 Conference. Cary, NC: SAS Institute Inc. (Paper 305-2008) ACKNOWLEDGMENTS Many thanks to Mario Widel and Xiangyun Wang for guidance and encouragement. RECOMMENDED READING Kuhfeld, Warren. 2010. Statistical Graphics in SAS®: An Introduction to the Graph Template Language and the Statistical Graphics Procedures. Cary, NC: SAS Institute, Inc. CONTACT INFORMATION Your comments and questions are valued and encouraged. Contact the author at: Sheila Dayog Genentech, A Member of the Roche Group 1 DNA Way South San Francisco, CA 94080 [email protected] SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc. in the USA and other countries. ® indicates USA registration. Other brand and product names are trademarks of their respective companies. 4