Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Substance dependence wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Moral treatment wikipedia , lookup
Psychological evaluation wikipedia , lookup
Psychiatric and mental health nursing wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Conversion disorder wikipedia , lookup
History of psychiatry wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
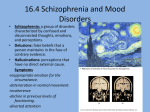
Schizophrenia wikipedia , lookup
History of mental disorders wikipedia , lookup
Abnormal psychology wikipedia , lookup
Social construction of schizophrenia wikipedia , lookup
Sluggish schizophrenia wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Essential guide to the psychiatric history and Mental state examination for CT1s Dr David Middleton ST6, Cambridge 23rd August 2011 General Principles of History Taking • Aim to understand problems/symptoms and effect on life • To put presenting problems into context by enquiring about background history and previous treatment • Is followed by MSE • Enables formulation to be reached • Is therapeutic in itself • Will vary according to setting (MHAA, A&E or OPD) Preparing The Setting • • • • • • Safety Privacy Try to avoid interruptions Arrange seating so sitting at angle to patient Writing materials Box of tissues. Starting the Interview • • • • • • Put patient at ease Introduce yourself and explain role Introduce to anyone who is accompanying patient Inform them about the length of interview Need to take notes Confidentiality Interview Style • Relaxed even if under time pressure • Appropriate eye contact, appear interested • Begin with a general question (e.g. “tell me about your problem”) • Have a systematic but flexible plan – at beginning can be helpful to take a list of headings as prompt • Keep in control. • May need to interrupt: “I’m sorry but I need to move on to other things” “We can come back to this if we have time later” Interview Techniques (1) • Use of open questions where possible, especially at beginning (e.g. “ how is your sleep?”) • Closed questions are useful if time is short (e.g. “is your sleep good?”) • Avoid leading questions (e.g. “You have poor sleep, don’t you?” Interview Techniques (2) • Encourage patient by mirroring their posture, nodding and using phrases such as: “go on…” “tell me more about…..” • Help them talk about painful or embarrassing subjects by being non-judgmental, acknowledging distress and explaining why you are asking: “I can see this is difficult to talk about…” Interview Techniques (3) • Summarise key points to check understanding • As experience grows start to select questions according to emerging diagnostic possibilities and management options. This is becomes more important when time is limited or patient uncooperative • Don’t take words at face value (e.g. “paranoid”) • Pick up non-verbal cues • Watch experienced clinicians and get them to watch you! • Video yourself Interviewing Informants • Always useful and more so if patient is cognitively impaired, patient is concealing information • Gain patient consent • Often best to see patient alone first and then informant • Establish confidentiality (and limits) • Ascertain informants concerns as well as gain information. • May need to help informant if stressed carer (carer assessment) Interviewing patients from other cultures (cultural competency) • Interview patients in first language where possible. May need interpreter. • Using interpreter’s skill. Discuss approach first. Manageable chunks of information. 2nd person, direct translation is most useful. • Distress is shown via different symptoms (e.g. physical rather then psychological symptoms) • Cultural beliefs may include ideas that appear delusional but are culturally acceptable (e.g. witchcraft). Need collateral information. • Treatment expectations may differ Records • Good notes are vital • Record for you, aids formulation • Record for others so history taking does not have to be repeated, as a record of presentation for future clinicians • Patients may request access to them • Life charts may be therapeutic way of recording information together The History (my preferred order!) • • • • • • • • • • Presenting complaint History of presenting complaint Past psychiatric history Past medical history Drug history Family history Personal history Forensic history Social history including drug/alcohol use Premorbid personality Presenting Complaint • Who referred patient and what is their concern/request • Where is patient being seen. • Are they voluntarily present or detained under MHA (which section) • What is their problem, in their own words History of presenting complaint • For each problem describe: Nature Precipitant/stressors Onset, time span, development of symptoms, fluctuations, factors worsening or improving Degree of functional impairment Level of distress Treatments attempted Past Psychiatric History • History of similar or other symptoms in past • Previous diagnosis • History of treatment – include from primary care, counselling, CAMHS, complementary therapy as well as mental health services • Previous hospitalisation, MHA, medications, ECT. • Recovery between episodes • Previous DSH and suicide attempts Past Medical History • Chronology of illness and treatment Drug History • Current medications (including alternative therapies) • Allergies • Check with GP • Ask to bring list to appointment Family History • Parent: age (now or at death), occupation, relationship with patient • Siblings: as above • Psychiatric history in family members (genetic and effect on home life). Substance use, suicide. • Genogram Personal history • • • • • • • • • Mother’s pregnancy, birth Early development, illness Childhood separation, emotional problems Relationships with family members, atmosphere at home Schooling – academic performance and peer relationships. (Bullying, school refusal, shyness, conduct disorders) Qualifications. Further education Occupation(s), work performance Sexual relationships, marriage, children History of abuse (physical, sexual, emotional) in childhood or adulthood Forensic History • Record all offences – convicted or not • Violence/Anger, sexual offences particularly important • Persistent offending • Probation • Relationship to symptoms Social history including drug/alcohol use • • • • Current occupation Working/off work – why? Relationship status, support networks Pastimes • Alcohol, other substances, tobacco Pattern of use Age at onset Relationship to symptoms Harmful use Psychological dependency Physical dependency Previous detox Patient’s view Premorbid Personality (1) • Hard to assess at one-off interview and collateral information should be sought. • GP may have useful information • Ask patient how others see them/would describe them • Prevailing mood; how they get on with people; deal with stress; hobbies; standards. Premorbid Personality (2) • • • • • • • • • • Impulsive Prone to worry Strict, fussy Seek attention Untrusting, resentful Irritable Sensitive Suspicious Argumentative Lack concern for others Mental State Examination What is the MSE • • • • • “Here and now” record of presentation History will give clues as to likely symptoms Systematic Until more experienced carry out full mental state Be observant but also learn the terminology to describe symptoms/signs • Use conventional headings to structure examination – other colleagues and examiners will expect it MSE • • • • • • • • Appearance and Behaviour Speech Mood Affect Thought Perception Cognition Insight Appearance and Behaviour Describe what you see: • General appearance and behaviour. Striking physical features. Posture. • Physique, clothing, cleanliness, self-care, posture • Eye contact, rapport • Motor activity: agitation, retardation, stuperose (akinesic and mute), abnormal movements (tic, tardive dyskinesia, chorea, stereotypy, catatonic features), mannerism, restlessness • Tearfulness • Distractibility • Disinhibition • “Appears to hear voices…” • Preoccupied Speech • Rate: slow in depression; pressure of speech in mania. • Quantity: reduced (poverty) in depression and chronic schizophrenia; flight of ideas in mania • Volume • Tone/rhythm: should have natural rhythm and intonation • Abnormal language: neologisms, word-finding difficulties Mood Patient description: Sad, happy, on top of the world, worried Accompanying symptoms • Depression: early morning wakening, diurnal variation, anhedonia, loss of appetite, loss of weight, fatigue, loss of concentration. Hopelessness, • Suicidal thoughts, plans, intent • Anxiety: palpitations, dry mouth, sweating, tremor • Elation: Overactivity, excessive self-confidence, reduced sleep, distractibility, increased libido Affect • Your objective description of emotion • Depressed, anxious, fearful, irritable, suspicious, perplexed, elated, angry • Fluctuations: reactivity, lability (mania), blunting (chronic schizophrenia) • Consistent with thoughts/behaviour? Incongruity seen in schizophrenia Thought Content (1) • Preoccupations: thoughts that recur frequently but can be put out of mind • Obsessional thoughts are ideas, images, impulses that repeatedly enter mind in stereotyped form, seen as senseless, distressing, recognised as own thought even if repugnant. • Compulsions are obsessional motor acts, often resulting from obsession, may be attempt to “neutralise” obsession. • “Do you have to keep on repeating the same action which most people would only do once?” Thought Content (2) Delusion is a false, unshakeable, belief that is out of keeping with the patient’s social and cultural background. Primary Delusion: used to be thought diagnostic of schizophrenia. • delusional mood: something going on but not sure what it is • delusional perception: attribution of new meaning to normally perceived object (e.g. traffic light change means chosen to be Messiah) • sudden delusional idea (autochthonous delusion): sudden arrival of fully formed delusion, like a “brain-wave” Thought Content (3) Secondary Delusion: explains another experience such as auditory hallucinations • Mood Congruent • Content: persecution, infidelity, grandiose, hypochondriacal, love, guilt, nihilistic, poverty, reference, infestation. Thought Content (4) • Thought Interference - “loss of boundary with outside world”, usually found in schizophrenia Thought withdrawal: thoughts taken away (link with thought block) Thought insertion: another agency’s thoughts implanted Thought broadcasting: thought’s leaking, escaping, other people know what thinking in unison (not thought echo) • Passivity – humans usually experience actions, thoughts, feelings as under their control but may (usually in schizophrenia) experience them as being under control of another agency Derealisation and Depersonalisation • Depersonalisation - feeling unreal and unable to feel emotion; “as if cut off from world” “watching self” • Derealisation – feeling world is unreal • Can occur in healthy people if tired • Occurs in anxiety, depression, schizophrenia, TLE • Unpleasant and very distressing Perception (1) • Illusion - Misperception of stimulus • Hallucination – Perception experienced in the absence of an external stimulus to the corresponding sense organ. • Can occur in any sensory modality: auditory, visual, olfactory, gustatory, tactile, deep sensation Perception (2) • Hallucinations: Visual: more likely in organic conditions Gustatory: unpleasant taste. In schizophrenia, TLE…may lead to delusion of being poisoned Olfactory: Schizophrenia, organic, TLE…may believe result of gas being pumped into dwelling Tactile: touched, pricked, insects crawling on skin (formication, drug withdrawal/cocaine addiction) Deep Sensation: often in schizophrenia…may be sexual. Auditory Hallucinations • May be noises, whispers, partially organised • 2nd person voices often in psychotic depression Characteristic, but not diagnostic of schizophrenia: • 3rd person discussing • Running commentary • Thought echo (echo de pensee, gedankenlautwerden) Cognition • • • • • • Orientation – time, place and person Attention – digit span Concentration – serial 7’s, WORLD STM – name and address recall after 3 mins LTM – history Frontal Lobe – verbal fluency, similarities/differences, Luria’s three stage task. • General knowledge and intelligence – from interview and PM, events • Can use screening instruments: MMSE or ACE Insight • • • • Awareness of abnormal state of mind Understanding of cause Understanding of benefits of treatment Awareness of effects of not having treatment Useful Reading • Shorter Oxford Textbook of Psychiatry, Gelder, Harrison & Cowen • Cognitive Assessment for Clinicians, 2nd edition, Hodges • Fish’s Clinical Psychopathology, 3rd Edition, Casey & Kelly • Sims’ Symptoms in the Mind, Femi Oyebode