Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
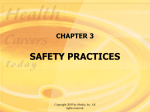
Chapter 16 Lung Abscess EDA PM AFC C RB B A Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. AFC, Air-fluid cavity; RB, ruptured bronchus (and drainage of the liquified contents of the cavity); EDA, early development of abscess; PM, pyogenic membrane. Consolidation (B) and excessive bronchial secretions (C) are common secondary anatomic alterations of the lungs. Slide 1 Copyright © 2006 by Mosby, Inc. Anatomic Alterations of the Lungs Slide 2 Alveolar consolidation Alveolar-capillary and bronchial wall destruction Tissue necrosis Cavity formation Fibrosis and calcification of the lung parenchyma Bronchopleural fistulae Atelectasis Excessive airway secretions and empyema Copyright © 2006 by Mosby, Inc. Etiology Slide 3 Pneumonia caused by aspiration (most common) Klebsiella Staphylococcus Predisposing factors for aspiration Alcohol abuse Seizure disorders General anesthesia Head trauma Cerebrovascular accident Swallowing disorders Copyright © 2006 by Mosby, Inc. Etiology (Less frequent causes) Slide 4 Aerobic organisms Streptococcus pyogenes Klebsiella pneumoniae Escherichia coli On rare occasions Streptococcus pneumoniae Pseudomonas aeruginosa Legionella pneumophila Copyright © 2006 by Mosby, Inc. Etiology (Other organisms that may lead to a lung abscess) Mycobacterium tuberculosis Fungal organisms Slide 5 Histoplasma capsulatum Coccidioides immitis Blastomyces Aspergillus fumigatus Parasites Paragonimus westermani Echinococcus Entamoeba histolytica Copyright © 2006 by Mosby, Inc. Etiology Lung abscess may also develop from: Slide 6 Bronchial obstruction Vascular obstruction Interstitial lung disease Bullae or cysts Penetrating chest wounds Copyright © 2006 by Mosby, Inc. Overview of the Cardiopulmonary Clinical Manifestations Associated with LUNG ABSCESS The following clinical manifestations result from the pathophysiologic mechanisms caused (or activated) by Alveolar Consolidation (see Figure 9-8), and when the abscess is draining, by Excessive Bronchial Secretions (see Figure 9-8)—the major anatomic alterations of the lungs associated with chronic bronchitis (see Figure 16-1). Slide 7 Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Vital signs Slide 8 Increased respiratory rate Increased heart rate, cardiac output, blood pressure Copyright © 2006 by Mosby, Inc. Clinical Data Obtained at the Patient’s Bedside Slide 9 Chest pain/decreased chest expansion Cyanosis Cough, sputum production, and hemoptysis Chest assessment findings Increased tactile and vocal fremitus Dull percussion note Bronchial breath sounds Diminished breath sounds Whispered pectoriloquy Pleural friction rub Copyright © 2006 by Mosby, Inc. Figure 2-11. A short, dull, or flat percussion note is typically produced over areas of alveolar consolidation. Slide 10 Copyright © 2006 by Mosby, Inc. Figure 2-16. Auscultation of bronchial breath sounds over a consolidated lung unit. Slide 11 Copyright © 2006 by Mosby, Inc. Figure 2-19. Whispered voice sounds auscultated over a normal lung are usually faint and unintelligible. Slide 12 Copyright © 2006 by Mosby, Inc. Clinical Data Obtained from Laboratory Tests and Special Procedures Slide 13 Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Expiratory Maneuver Findings Slide 14 FVC FEVT N or FEF25%-75% N or FEF200-1200 N PEFR MVV FEF50% FEV1% N N or N N or Copyright © 2006 by Mosby, Inc. Pulmonary Function Study: Lung Volume and Capacity Findings VT RV FRC TLC N or VC Slide 15 IC ERV RV/TLC% N Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Mild to Moderate Lung Abscess pH Slide 16 Acute alveolar hyperventilation with hypoxemia PaCO2 HCO3 (Slightly) PaO2 Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation 100 90 PaO2 or PaCO2 80 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors 70 60 PaO2 50 40 30 20 10 0 Figure 4-2. PaO2 and PaC02 trends during acute alveolar hyperventilation. Slide 17 Copyright © 2006 by Mosby, Inc. Arterial Blood Gases Severe Lung Abscess Acute ventilatory failure with hypoxemia pH Slide 18 PaCO2 HCO3 (Slightly) PaO2 Copyright © 2006 by Mosby, Inc. Time and Progression of Disease Disease Onset Alveolar Hyperventilation Acute Ventilatory Failure 100 90 Pa02 or PaC02 80 70 Point at which PaO2 declines enough to stimulate peripheral oxygen receptors Point at which disease becomes severe and patient begins to become fatigued 60 50 40 30 20 10 0 Figure 4-7. PaO2 and PaCO2 trends during acute ventilatory failure. Slide 19 Copyright © 2006 by Mosby, Inc. Oxygenation Indices QS/QT DO2 VO2 Normal O2ER Slide 20 C(a-v)O2 Normal SvO2 Copyright © 2006 by Mosby, Inc. Abnormal Laboratory Tests and Procedures Sputum examination Gram-positive organism Slide 21 Streptococcus Anaerobic organisms Peptococcus Peptostreptococcus Bacteroides Fusobacterium Copyright © 2006 by Mosby, Inc. Radiologic Findings Chest radiograph Slide 22 Increased density Cavity formation Cavity with air-fluid levels Fibrosis Pleural effusion Copyright © 2006 by Mosby, Inc. Figure 16-2. Reactivation tuberculosis with a large cavitary lesion containing an air-fluid level in the right lower lobe. Smaller cavitary lesions are seen in other lobes. (From Armstrong P et al: Imaging of diseases of the chest, ed 2, St. Louis, 1995, Mosby.) Slide 23 Copyright © 2006 by Mosby, Inc. General Management of Lung Abscess Respiratory care treatment protocols Slide 24 Oxygen therapy protocol Bronchopulmonary hygiene therapy protocol Hyperinflation therapy protocol Copyright © 2006 by Mosby, Inc. General Management of Lung Abscess Medications and procedures commonly prescribed by the physician Slide 25 Antibiotics Surgery Copyright © 2006 by Mosby, Inc. Classroom Discussion Case Study: Lung Abscess Slide 26 Copyright © 2006 by Mosby, Inc.