Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmacognosy wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
Drug discovery wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Psychopharmacology wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Prescription costs wikipedia , lookup
HIV vaccine wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of non-nucleoside reverse-transcriptase inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Theralizumab wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Discovery and development of HIV-protease inhibitors wikipedia , lookup
SOMJED SAHASITWAT
Indinavir (CRIXIVAN®)
Introduction
AIDS or acquired immune deficiency syndrome allows opportunistic infection
to occur. Most patients die from opportunistic infections. In the beginning this
disease was identified in male homosexuals. But today time HIV infected patients can
be heterosexual or homosexual, male or female, adult or infant, Scientists found that
the cause of this disease is a retrovirus, primarily called LAV (Lymphadenopathyassociated virus) because this virus was identified in patients who have
lymphadenopathy in pre-AIDS conditions and AIDS conditions. Furthermore,
scientists isolated HTLV-3 (human T cell lymphotropic virus, type 3) from many
AIDS patients and they discovered both viruses have the same shape and
propertiesConsequently they renamed the viruses Human Immune Deficiency Virus
(HIV)
Scientists are trying to fight with this disease in many ways. They have
conducted a lot of research about this virus and they have studied the life cycle of
virus. Can produce based on these studies they have produced many chemicals that
interfere with three major pathway of viral life cycle; reverse transcriptase inhibitors;
integrase inhibitors; and is protease inhibitors. The group of protease inhibitors
contains many chemicals such as saquinavir, ritonavir, nelfinavir and indinavir.
Indinavir is the product from Merck. USFDA approved this drug on 1996.
This drug is indicated for the treatment of adults with HIV-1 infection. When doctors
consider some drugs to treat HIV infected patients they want to have adequate
information about the chemicals to guarantee that the patients can take these drugs in
an effective and safe way.
History of CRIXIVAN®
In 1987 AIDS was an acknowledged worldwide epidemic, with an estimated
5-10 million infected, and everyone was looking ways for to treat this disease. Based
on information about the physical structure of HIV, the Merck research team led by
virologist Emilio Emini and biochemist Irving Sigal focused on the protein protease,
Protease is required for viral replication. Sigal had surmised, that inhibiting this
enzyme would prevent the deadly virus from multiplying. This hypothesis was
confirmed by Nancy E.Kohl, a biochemist. Her research showed that if HIV “s
protease enzyme was inhibited, the virus would not spread from cell to cell. This
background research for the Merck team led to the development of CRIXIVAN.
Which was approved by the FDA in 1996.
1
SOMJED SAHASITWAT
What is CRIXIVAN®?
Crixivan® is the trade name of Indinavir sulfate, and it is a protease inhibitor.
I.e. it prevents the protease enzyme from working. HIV protease acts like chemical
scissors. It cuts the raw material for HIV into the specific pieces that are needed to
build a new virus. Protease inhibitors "gum up" these scissors.
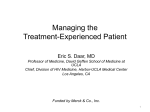
Indinavir sulfate’s molecular formula is C36H47N5O4*H2SO4. It has a
molecular weight of 711.88. It is hygroscopic, crystalline powder and very soluble in
water and in methanol.
Structural formula of Indinavir sulfate
How dose CRIXIVAN® work?
Protease enzymes are proteins that cut other proteins at highly specific
locations. The HIV protease is an aspartyl protease enzyme similar to mammalian
proteases like renin. However, HIV protease activity is unique for HIV proteins,
and in the host there is virtually no cross-reactivity between the HIV protease and
normal human protease gene products. It is this lack of cross-reactivity that gives the
protease inhibitors their outstanding safety profile.
The HIV protease enzyme cleaves polyproteins of the virus into essential
functional protein products during the maturation process of the virion. This critical
process occurs as each new virion buds forth from the membrane of an HIV-infected
cell and continues after the immature virus is released from the cell. If the
2
SOMJED SAHASITWAT
polyproteins are not cleaved, the virus fails to mature and is incapable of infecting a
new cell.
The protease inhibitors are able to inhibit the function of the native protease
enzyme. They exert their inhibitory effect by disabling the enzyme before it can
cleave the gag/pol polyprotein into its essential products. Like a key perfectly fitted to
a lock, the protease inhibitor simply locks up the enzyme, rendering it ineffectual.
.
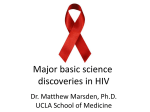
The diagram above shows the virus entering the cell (1), the cell making new
proteins (2-3), the proteins forming a new virus (4) and the cell releasing the new
virus to infect other cells (5). It also shows some steps in the process that can be
interrupted by protease inhibitors and other antiviral drugs (reverse transcriptase
inhibitors) that are taken along with protease inhibitors.
Clinical Pharmacology
Absorption: Indinavir was rapidly absorbed in the fasted state with a time to
peak plasma concentration (Tmax) of 0.8+0.3 hours (mean + S.D.) (n=11). At a
dosing regimen of 800 mg every 8 hours, the steady-state area under the plasma
concentration time curve (AUC) was 30,691+11,407 nM*hour (n=16), and plasma
concentration eight hours post dose (trough) was 251+178 nM (n=16), serum half-life
1.5-2 hours.
Effect of Food on Oral Absorption: Meal with high calories, fat, and protein
(784 kcal, 48.6 g fat, 31.3 g protein) resulted in a 77% + 8% reduction in AUC and an
84% + 7% reduction in Cmax (n=10). Administration with lighter meals resulted in
little or no change in AUC, Cmax or trough concentration. It if you take indinavir on
an empty stomach the drug will get absorbed better it will have a stronger effect.
However, a light meal can be eaten with indinavir, as long as it does not exceed the
limit in any of the following four nutritional areas.
0 to 65 grams of carbohydrate
0 to 5.7 grams of protein
3
SOMJED SAHASITWAT
0 to 2 grams of fat
0 to 301 calories
*Should avoided grapefruit juice it can reduces indinavir blood levels by about 25%
Metabolism: Following a 400 mg dose of 14C-Indinavir, 83+1% (n=4) and
19+3% (n=6) of the total radioactivity was recovered in feces and urine, respectively:
radioactivity due to parent drug in feces and urine was 19.1% and 9.4%, respectively.
The major enzyme metabolite is cytochrome P-450 3A4 indinavir is a worst substrate
for cytochrome P450 than ritonavir.
Elimination: Less than 20% of indinavir is excreted unchanged in urine.
Mean urinary excretion of unchanged drug was 10.4 + 4.9% (n=10) and 12.0 + 4.9%
(n=10) following a single 700 mg and 1000 mg dose, respectively, Indinavir was
rapidly eliminated with a half-life of 1.8 + 0.4 hours (n=10). Significant accumulation
was not observed after multiple dosing at 800 mg every 8 hours.
Problem of protease resistance
HIV replication is an extremely dynamic process, with as many as 1010 new
viral particles being produced every day. We also know that the replication of HIV
reverse transcriptase is a markedly error-prone process. As a result, this high level of
viral turnover results in between 104 and 105 mutations at each site in the HIV
genome each day. It is therefore not surprising that many patients eventually develop
resistance to whatever antiretroviral regimen they have been assigned. Phenotypic and
genotypic resistance has been described for each of the four-protease inhibitors that
have received F.D.A. approval . The mutations that lead to resistance for each of these
protease inhibitors are complex: there are more than 20 sites within the HIV-1
protease gene that have been associated with resistance to these agents (Table 1).
Although each drug in this class selects for a specific, predictable pattern of genotypic
changes, these patterns do overlap -- and where they do, cross-resistance may occur.
Table 1: HIV Resistance to Protease Inhibitors
DRUG
CRITICAL
SECONDARY
MUTATIONS*
MUTATIONS**
Saquinavir
48, 90
10, 36, 63, 71
Ritonavir
82, 84
20, 36, 46, 54, 63, 71, 90
Indinavir
46, 82
10, 20, 24, 32, 54, 63, 71,
84, 90
Nelfinavir
30
46, 63, 71, 88, 90
*Numbers refer to the codon position on the HIV protease gene that has been shown to
be critical for the development of phenotypic resistance to each of the protease
inhibitors.
**The role of these secondary mutations in the development of protease inhibitor
resistance is unclear. Many of these changes may be compensatory and may enhance
the virus's ability to replicate once the critical mutations occur. Furthermore, many of
these observed changes exist as naturally occurring polymorphisms in untreated
patients.
4
SOMJED SAHASITWAT
In the early clinical trials of indinavir, the use of low doses of the drug (less than 2.4
grams/day) resulted in dramatic reductions in plasma HIV RNA levels. Because those
doses were too low to prevent the development of resistance, reductions in viral
burden were transient -- and switching indinavir-resistant patients to higher doses had
no effect on HIV RNA levels.
The concurrent use of zidovudine appears to reduce the incidence at which
genotypic resistance to indinavir develops. In one well-designed clinical trial, Merck
Study 019, antiretroviral-naïve patients were randomized to receive either ZDV alone,
indinavir alone, or the two drugs in combination. After 24 weeks of treatment,
patients in the two-drug regimen had a relatively low incidence of indinavir resistance
(4 of 22 subjects, or 18%). By contrast, patients on indinavir monotherapy had a
significantly higher incidence of resistance (9 of 21 subjects, or 43%).
Clinical data on the subjects in ACTG 320 who received the triple-drug
combination of indinavir, ZDV, and 3TC suggest that the use of these three agents
may further retard the emergence of indinavir resistance.
5
SOMJED SAHASITWAT
Drugs which should not be taken with indinavir
Some drugs when taken with indinavir they may cause heart or breathing
problems: Seldane® (terfenadine), Hismanal® (astemizole), Propulsid, Halcion, or
Versed.
Rifampin makes indinavir less effective, so they should not be taken together.
Drugs should not taken with indinavir
Antimycobacterial (Anti-TB or antiMAC):
Potential alternatives
clarithromycin (Biaxin)
azithromycin (Zithromax)
ethambutol (Myambutol)
rifampin (Rifadin, others)
Cold and allergy antihistamines:
loratadine (Claritin)
Astemizole® (Hismanal),
terfenadine® (Seldane)
Gastrointestinal:
cisapride (Propulsid)
very limited clinical experience
Drugs requiring dose modification when taken along with indinavir
•
•
•
•
•
Delavirdine : dose reduction of CRIXIVAN to 600 mg, every 8 hrs, because delavirdine inhibits
the metabolism of indinavir.
Didanosine : should take CRIXIVAN at least one 1 hr apart on empty stomach, because
didanosine contains an acidic buffer, that can reduce absorption of indinavir.
Efavirenz : increase the dose of CRIXIVAN to 1000 mg every 8 hrs, because of a 31% and 16%
reduction in AUC and Cmax, of indinavir respectively, as a result of enzyme induction.
Itraconazole and Ketoconazole : reduction of CRIXIVAN dose to 600 mg every 8 hrs, because
itraconazole and ketoconazole inhibits the metabolism of indinavir.
Rifabutin : reduction of rifabutin to half the standard dose and increase of CRIXIVAN to 1000
mg every 8 hrs, because rifabutin decreases the indinavir AUC and indinavir can increase the
rifabutin AUC.
Side effect
Nausea, pain in the abdomen (belly), and headache are the most common side
effects of indinavir therapy. Pain in the side and/or blood in the urine should be
reported to the doctor immediately, because it may signal kidney stones, a serious
problem with the kidneys. Drinking large amounts of water (1.5 liters/24hours) can
6
SOMJED SAHASITWAT
help to avoid these side effects. Sometimes people taking indinavir have abnormal
liver test results even without symptoms.
Some people taking protease inhibitors have had problems with their blood sugar levels, or
have developed diabetes. Symptoms, such as increased thirst, hunger, urination, or weight loss should
be reported to the doctor immediately. People with diabetes who are considering HIV protease inhibitor
therapy should talk with their doctors about carefully monitoring their glucose (blood sugar) level.
Some people with hemophilia type A or B have reported increased bleeding problems. It is
not known whether this is related to indinavir, but these problems should be reported to the doctor
immediately so they can be treated that.
Special population
Hepatic Insufficiency: Patients with mild to moderate hepatic insufficiency and clinical
evidence of cirrhosis demonstrated decreased metabolism of indinavir resulting in approximately 60%
higher mean AUC following a single 400 mg dose (n=12). The half-life of indinavir increased to 2.8 +
0.5 hours. Then dosage of indinavir should be reduced to 600 mg every 8 hours. Indinavir
pharmacokinetics have not been studied in patients with severe hepatic insufficiency
Renal Insufficiency: The pharmacokinetics of indinavir has not been studied in-patients with
renal insufficiency
Pregnancy: Indinavir have category C, There are no adequate and wellcontrolled studies in pregnant woman. Indinavir should be used during pregnancy
only if the potential benefit justifies the potential risk to fetus.
Antiretroviral
Drug
FDA
Pregnancy
Category*
Saquinavir
Indinavir
B
C
Ritonavir
B
Placental
Passage
[Newborn:
Maternal
Drug Ratio]
Unknown
Yes (rats)
("Significant"
in rats, low in
rabbits)
Yes (rats)
[mid-term
fetus, 1.15;
late-term fetus,
7
long-term
Animal
Carcinogenicity
Studies
Rodent Teratogen
Not completed
Not completed
Negative
Negative (but
extra ribs in rats)
Not completed
Negative (but
cryptorchidism in
rats)+
SOMJED SAHASITWAT
Nelfinavir
B
0.15-0.64]
Unknown
Not completed
Negative
* FDA Pregnancy Categories are:
A - Adequate and well-controlled studies of pregnant women fail to demonstrate a risk to the
fetus during the first trimester of pregnancy (and there is no evidence of risk during later trimesters);
B - Animal reproduction studies fail to demonstrate a risk to the fetus and adequate but wellcontrolled studies of pregnant women have not been conducted;
C - Safety in human pregnancy has not been determined, animal studies are either positive for
fetal risk or have not been conducted, and the drug should not be used unless the potential benefit
outweighs the potential risk to the fetus;
D - Positive evidence of human fetal risk based on adverse reaction data from investigational
or marketing experiences, but the potential benefits from the use of the drug in pregnant women may
be acceptable despite its potential risks;
X - Studies in animals or reports of adverse reactions have indicated that the risk associated
with the use of the drug for pregnant women clearly outweighs any possible benefit.
** Despite certain animal data showing potential teratogenicity of ZDV when near-lethal
doses are given to pregnant rodents, considerable human data are available to date indicating that the
risk to the fetus, if any, is extremely small when given to the pregnant mother beyond 14 weeks
gestation. Follow-up for up to 6 years of age for 734 infants born to HIV-infected women who had in
utero exposure to ZDV has not demonstrated any tumor development.(93) However, no data is
available on longer follow-up for late effects.
+ These effects seen at only at maternally toxic doses.
Nursing Mothers: Studies in lactating rats have demonstrated that indinavir is excreted in
milk. Although it is not known whether indinavir is excreted in human milk, there exists the potential
for adverse effects from indinavir in nursing infants. Mothers should be instructed to discontinue
nursing if they are receiving indinavir.
Overdose
There have been more reports of acute or chronic human overdosage (up to 23
times the recommended total daily dose of 2400 mg) with indinavir. The most
commonly reported symptoms were renal (e.g., nephrolithiasis, flank pain, hematuria)
and gastrointestinal (e.g., nausea, vomiting, diarrhea).
It is not known whether indinavir is dialyzable by peritoneal or hemodialiysis.
Dosage and administration
Recommended dosage of indinavir is 800 mg orally every 8 hours. Must be
taken at intervals of 8 hours. For optimal absorption, it should be administered
without food but with water 1 hour before or 2 hours after a meal. To ensure adequate
hydration, it is recommended that the patient drink at least 1.5 liters (approximately
48 ounces) of liquids during the course of 24 hours.
8
SOMJED SAHASITWAT
Storage
Store in a tightly closed container at room temperature, 15-30oC. Protect from
moisture.
Conclusion
Indinavir is an antiretroviral drug that inhibits the protease action. It should be
used in combination therapy with other antiretroviral drugs to pospone the occurrence
resistance. Indinavir should be administered at optimal therapeutic doses as
subobtimal doses of drugs can promote the development of high-level protease
resistance. When it is used with others drugs in drugs interactions should be
considerd. To diminish severe side effect such as nephrolithiasis the patient should
drink of least 1.5 litter of liquids each day.
The advantages of indinavir are when treat in triple combination with ZDV
and 3TC consequence maintained viral load at undetectable levels, providing durable
suppression in 68% of patients for three years. And this triple combination therapy
slowed HIV disease prgression or death by 50% over zidovudine (ZDV) (or stavudine
(d4t)) + lamivudine (3TC). Indinavir has few significant drug interactions with most
other drugs frequently prescribed for HIV patients. And has been shown to be
generally well tolerated, which may assist compliance. Indinavir is the only protease
inhibitor requiring at least three viral mutations before resistance can emerge.
References
1) http://www.crixivan.com
2) FDA Protease inhibitors Backgrounder.htm
3) ATIS Guidelines for the Use of Antiretroviral Agents in HIV-Infected
Adults and Adolescents.htm
4) Simple Facts Sheets protease inhibitors.htm
5) Simple Facts Sheets indinavir (Crixivan).htm
6) Drug prescription from MERCK &CO., INC., Elkton, U.S.A.
9
SOMJED SAHASITWAT
10