Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
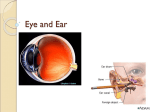
Physiology of Hearing & Equilibrium Dr. Vishal Sharma Parts of hearing apparatus Conductive apparatus: external & middle ear Conducts mechanical sound impulse to inner ear Perceptive apparatus: cochlea Converts mechanical sound impulse into electrical impulse & transmits to higher centers Role of external ear • Collection of sound waves by pinna & conduction to tympanic membrane • Increases sound intensity by 15-20 dB • Cupping of hand behind pinna also increases sound intensity by 15 dB especially at 1.5 kHz. Role of middle ear in hearing • Impedance matching mechanism (step – up transformer or amplifier function) • Preferential sound pressure application to oval window (phase difference by ossicular coupling) • Equalization of pressure on either sides of tympanic membrane (via Eustachian tube) Impedance matching mechanism • When sound travels from air in middle ear to fluid in inner ear, its amplitude is ed by fluid impedance. • Only 0.1 % sound energy goes inside inner ear. • Middle ear amplifies sound intensity to compensate for this loss. Converts sound of low pressure, high amplitude to high pressure, low amplitude vibration suitable for driving cochlear fluids. Hermann von Helmholtz Described impedance matching in 1868 T.M. Catenary lever (curved membrane effect): Sound waves focused on malleus. Magnifies 2 times Ossicular Lever ratio: Length of handle of malleus > long process of incus. Magnifies 1.3 times Surface area ratio (Hydraulic lever): T.M. = 55 mm2 ; Stapes foot plate = 3.2 mm2 Magnifies 17 times Total Mechanical advantage: 2 X 17 X 1.3 = 45 times = 30 – 35 dB Natural Resonance • Property to allow certain sound frequencies to pass more readily to inner ear. • External auditory canal = 2500 – 3000 Hz • Tympanic membrane = 800 - 1600 Hz • Ossicular chain = 500 – 2000 Hz • Range = 500 – 3000 Hz (speech frequency) Preferential sound pressure application (phase difference) • Sound pressure preferentially applied to oval window by ossicular coupling while round window is protected by tympanic membrane • Sound pressure travels to scala vestibuli helicotrema scala tympani round window membrane yields scala media moves up & down movement of hair cells in scala media Preferential sound pressure application (phase difference) • Yielding of round window membrane (push-pull effect) is necessary as inner ear fluids are incompressible • Large tympanic membrane perforation loss of this function (push-push effect) no movement of inner ear fluids Ossicular break + intact T.M. = 55-60 dB loss Ossicular break + T.M. perforated = 45-50 dB loss Transduction of mechanical energy to electrical impulses – Movement of basilar membrane – Shear force between tectorial membrane & hair cells – Cochlear microphonics – Nerve impulses Cochlear hair cells Transducer Mechanism Auditory pathway • Eighth (Auditory) nerve • Cochlear nucleus • Olivary nucleus (superior) • Lateral lemniscus • Inferior colliculus • Medial geniculate body • Auditory cortex Theories of hearing Place / Resonance Theory (Helmholtz, 1857) Perception of pitch depends on selective vibration of specific place on basilar membrane. Telephone Theory (Rutherford, 1886) Entire basilar membrane vibrates. Pitch related to rate of firing of individual auditory nerve fibers. Theories of hearing Volley Theory (Wever, 1949) > 5 KHz: Place theory; <400 Hz: Telephone theory 400 – 5000 Hz: Volley theory Groups of fibres fire asynchronously (volley mechanism). Required frequency signal is presented to C.N.S. by sequential firing in groups of 2 - 5 fibers as each fiber has limitation of 1 Khz. Bekesy’s travelling wave theory Sound stimulus produces a wave-like vibration of basilar membrane starting from basal turn towards apex of cochlea . It increases in amplitude as it moves until it reaches a maximum & dies off. Sound frequency is determined by point of maximum amplitude. High frequency sounds cause wave with maximum amplitude near to basal turn of cochlea. Low frequency sound waves have their maximum amplitude near cochlear apex. Georg von Bekesy Won Nobel prize for his traveling wave theory in 1961 Bekesy’s travelling wave theory Theories of bone conduction Compression theory: skull vibration from sound stimulus vibration of bony labyrinth & inner ear fluids Inertia theory: sound stimulus skull vibration but ear ossicles lag behind due to inertia. Out of phase movement of skull & ear ossicles movement of stapes footplate vibration of inner ear fluids Theories of bone conduction Osseo-tympanic theory: sound stimulus skull vibration but mandible condyle lags behind due to inertia. Out of phase movement of skull & mandible vibration of air in external auditory canal vibration of tympanic membrane Tonndorf’s theory: sound stimulus skull vibration rotational vibration of ear ossicles movement of stapes footplate Physiology of equilibrium Balance of body during static or dynamic positions is maintained by 4 organs: 1. Vestibular apparatus (inner ear) 2. Eye 3. Posterior column of spinal cord 4. Cerebellum Vestibular apparatus Semicircular canals Angular acceleration & deceleration Utricle Horizontal linear acceleration & deceleration Saccule Vertical linear acceleration & deceleration Orientation of semicircular canals Physiology of head movement Head Movement Semicircular canal stimulated Yaw Lateral Pitch Posterior + Superior Roll Superior + Posterior Nystagmus (slow component) Nystagmus (fast component) Semicircular canal stimulated Nystagmus Direction Right Lateral Right horizontal Left Lateral Left horizontal Right Superior Down beating, counter-clockwise Left Superior Down beating, clockwise Right Posterior Up beating, counter-clockwise Left Posterior Up beating, clockwise Vestibulo-ocular reflex (VOR) Movement of head to left left horizontal canal stimulated & right horizontal canal inhibited To keep eyes fixed on a stationary point, both eyes move to right side by stimulating right lateral rectus & left medial rectus muscles Thank You