Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
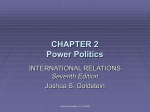
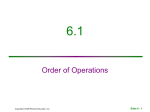
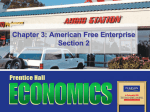
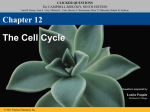
Copyright © 2010 Pearson Education, Inc. Figure 16.8 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Capillary Tyrosines (part of thyroglobulin molecule) Golgi apparatus Rough ER Colloid in lumen of follicle Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 1 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Capillary Tyrosines (part of thyroglobulin molecule) Golgi apparatus Rough ER Iodide (I–) 2 Iodide (I–) is trapped (actively transported in). Colloid in lumen of follicle Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 2 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Capillary Tyrosines (part of thyroglobulin molecule) Golgi apparatus Rough ER Iodide (I–) Iodine 3 Iodide is oxidized to iodine. 2 Iodide (I–) is trapped (actively transported in). Colloid in lumen of follicle Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 3 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Capillary Tyrosines (part of thyroglobulin molecule) 4 Iodine is attached to tyrosine in colloid, forming DIT and MIT. Golgi apparatus Rough ER Iodide (I–) Iodine 3 Iodide is oxidized to iodine. DIT (T2) MIT (T1) Thyroglobulin colloid 2 Iodide (I–) is trapped (actively transported in). Colloid in lumen of follicle Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 4 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Tyrosines (part of thyroglobulin molecule) Capillary 4 Iodine is attached to tyrosine in colloid, forming DIT and MIT. Golgi apparatus Rough ER Iodide (I–) 2 Iodide (I–) is trapped (actively transported in). Iodine 3 Iodide is oxidized to iodine. T4 T3 DIT (T2) MIT (T1) Thyroglobulin colloid 5 Iodinated tyrosines are linked together to form T 3 and T4. Colloid in lumen of follicle Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 5 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Tyrosines (part of thyroglobulin molecule) Capillary 4 Iodine is attached to tyrosine in colloid, forming DIT and MIT. Golgi apparatus Rough ER Iodide (I–) Iodine 3 Iodide is oxidized to iodine. 2 Iodide (I–) is trapped (actively transported in). Lysosome T4 T3 6 Thyroglobulin colloid is endocytosed and combined with a lysosome. Copyright © 2010 Pearson Education, Inc. DIT (T2) MIT (T1) Thyroglobulin colloid 5 Iodinated tyrosines are linked together to form T 3 and T4. Colloid in lumen of follicle Figure 16.9, step 6 Thyroid follicle cells Colloid 1 Thyroglobulin is synthesized and discharged into the follicle lumen. Tyrosines (part of thyroglobulin molecule) Capillary 4 Iodine is attached to tyrosine in colloid, forming DIT and MIT. Golgi apparatus Rough ER Iodine 3 Iodide is oxidized to iodine. 2 Iodide (I–) is trapped (actively transported in). Iodide (I–) Lysosome T4 T3 DIT (T2) MIT (T1) Thyroglobulin colloid 5 Iodinated tyrosines are linked together to form T 3 and T4. T4 T3 T4 T3 6 Thyroglobulin colloid is endocytosed and combined with a lysosome. 7 Lysosomal enzymes cleave T4 and T3 from thyroglobulin colloid and hormones diffuse into bloodstream. Colloid in lumen of follicle To peripheral tissues Copyright © 2010 Pearson Education, Inc. Figure 16.9, step 7 Hypothalamus TRH Anterior pituitary TSH Thyroid gland Thyroid hormones Target cells Copyright © 2010 Pearson Education, Inc. Stimulates Inhibits Figure 16.7 Homeostatic Imbalances of TH • Hyposecretion in adults—myxedema; endemic goiter if due to lack of iodine • Hyposecretion in infants—cretinism • Hypersecretion—Graves’ disease Copyright © 2010 Pearson Education, Inc. Copyright © 2010 Pearson Education, Inc. Figure 16.10 Pharynx (posterior aspect) Thyroid gland Parathyroid glands Chief cells (secrete parathyroid hormone) Oxyphil cells Esophagus Trachea (a) Copyright © 2010 Pearson Education, Inc. Capillary (b) Figure 16.11 Hypocalcemia (low blood Ca2+) stimulates parathyroid glands to release PTH. Rising Ca2+ in blood inhibits PTH release. Bone 1 PTH activates osteoclasts: Ca2+ and PO43S released into blood. Kidney 2 PTH increases 2+ Ca reabsorption in kidney tubules. 3 PTH promotes kidney’s activation of vitamin D, which increases Ca2+ absorption from food. Intestine Ca2+ ions PTH Molecules Copyright © 2010 Pearson Education, Inc. Bloodstream Figure 16.12 Capsule Zona glomerulosa • Medulla • Cortex Cortex Adrenal gland Zona fasciculata Zona reticularis Medulla Kidney Adrenal medulla (a) Drawing of the histology of the adrenal cortex and a portion of the adrenal medulla Copyright © 2010 Pearson Education, Inc. Figure 16.13a Mechanisms of Aldosterone Secretion 1. Renin-angiotensin mechanism: decreased blood pressure stimulates kidneys to release renin, triggers formation of angiotensin II, a potent stimulator of aldosterone release 2. Plasma concentration of K+: Increased K+ directly influences the zona glomerulosa cells to release aldosterone 3. ACTH: causes small increases of aldosterone during stress 4. Atrial natriuretic peptide (ANP): blocks renin and aldosterone secretion, to decrease blood pressure Copyright © 2010 Pearson Education, Inc. Primary regulators Blood volume and/or blood pressure Other factors K+ in blood Stress Blood pressure and/or blood volume Hypothalamus Kidney Heart CRH Renin Initiates cascade that produces Direct stimulating effect Anterior pituitary Atrial natriuretic peptide (ANP) ACTH Angiotensin II Inhibitory effect Zona glomerulosa of adrenal cortex Enhanced secretion of aldosterone Targets kidney tubules Absorption of Na+ and water; increased K+ excretion Blood volume and/or blood pressure Copyright © 2010 Pearson Education, Inc. Figure 16.14 Homeostatic Imbalances of Aldosterone • Aldosteronism—hypersecretion due to adrenal tumors • Hypertension and edema due to excessive Na+ • Excretion of K+ leading to abnormal function of neurons and muscle Copyright © 2010 Pearson Education, Inc. Homeostatic Imbalances of Glucocorticoids • Hypersecretion—Cushing’s syndrome • Depresses cartilage and bone formation • Inhibits inflammation • Depresses the immune system • Promotes changes in cardiovascular, neural, and gastrointestinal function • Hyposecretion—Addison’s disease • Also involves deficits in mineralocorticoids • Decrease in glucose and Na+ levels • Weight loss, severe dehydration, and hypotension Copyright © 2010 Pearson Education, Inc. Copyright © 2010 Pearson Education, Inc. Figure 16.15 Short-term stress More prolonged stress Stress Nerve impulses Hypothalamus CRH (corticotropinreleasing hormone) Spinal cord Corticotroph cells of anterior pituitary To target in blood Preganglionic sympathetic fibers Adrenal medulla (secretes amino acidbased hormones) Catecholamines (epinephrine and norepinephrine) Short-term stress response 1. Increased heart rate 2. Increased blood pressure 3. Liver converts glycogen to glucose and releases glucose to blood 4. Dilation of bronchioles 5. Changes in blood flow patterns leading to decreased digestive system activity and reduced urine output 6. Increased metabolic rate Copyright © 2010 Pearson Education, Inc. Adrenal cortex (secretes steroid hormones) ACTH Mineralocorticoids Glucocorticoids Long-term stress response 1. Retention of sodium and water by kidneys 2. Increased blood volume and blood pressure 1. Proteins and fats converted to glucose or broken down for energy 2. Increased blood glucose 3. Suppression of immune system Figure 16.16 Glucagon • Major target liver promotes • Glycogenolysis—breakdown glycogen to glucose • Gluconeogenesis—synthesis of glucose from lactic acid and noncarbohydrates • Release of glucose to the blood Copyright © 2010 Pearson Education, Inc. Insulin • Effects of insulin • Lowers blood glucose levels • Enhances membrane transport of glucose into fat and muscle cells • Participates in neuronal development and learning and memory • Inhibits glycogenolysis and gluconeogenesis Copyright © 2010 Pearson Education, Inc. Insulin Action on Cells • Activates a tyrosine kinase enzyme receptor • Cascade leads to increased glucose uptake and enzymatic activities that • Catalyze the oxidation of glucose for ATP production • Polymerize glucose to form glycogen • Convert glucose to fat (particularly in adipose tissue) Copyright © 2010 Pearson Education, Inc. Stimulates glucose uptake by cells Tissue cells Insulin Pancreas Stimulates glycogen formation Glucose Glycogen Blood glucose falls to normal range. Liver Stimulus Blood glucose level Stimulus Blood glucose level Blood glucose rises to normal range. Pancreas Liver Glucose Glycogen Stimulates glycogen Glucagon breakdown Copyright © 2010 Pearson Education, Inc. Figure 16.18 Copyright © 2010 Pearson Education, Inc. Table 16.4 Other Hormone-Producing Structures • Kidneys • Erythropoietin signals production of red blood cells • Renin initiates the renin-angiotensin mechanism • Skin • Cholecalciferol, the precursor of vitamin D • Adipose tissue • Leptin is involved in appetite control, and stimulates increased energy expenditure Copyright © 2010 Pearson Education, Inc. Other Hormone-Producing Structures • Skeleton (osteoblasts) • Osteocalcin prods pancreatic beta cells to divide and secrete more insulin, improving glucose handling and reducing body fat • Thymus • Thymulin, thymopoietins, and thymosins are involved in normal the development of the T lymphocytes in the immune response Copyright © 2010 Pearson Education, Inc. Developmental Aspects • Exposure to pesticides, industrial chemicals, arsenic, dioxin, and soil and water pollutants disrupts hormone function • Sex hormones, thyroid hormone, and glucocorticoids are vulnerable to the effects of pollutants • Interference with glucocorticoids may help explain high cancer rates in certain areas Copyright © 2010 Pearson Education, Inc. Developmental Aspects • Ovaries undergo significant changes with age and become unresponsive to gonadotropins; problems associated with estrogen deficiency begin to occur • Testosterone also diminishes with age, but effect is not usually seen until very old age Copyright © 2010 Pearson Education, Inc. Developmental Aspects • GH levels decline with age and this accounts for muscle atrophy with age • TH declines with age, contributing to lower basal metabolic rates • PTH levels remain fairly constant with age, but lack of estrogen in older women makes them more vulnerable to bone-demineralizing effects of PTH Copyright © 2010 Pearson Education, Inc.