Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
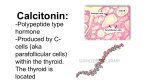
Synthesis of Thyroid Hormones Unlike most endocrine glands, the thyroid gland stores large amounts of some of the hormones it synthesizes. Thyroglobulin is produced and secreted by follicle cells into the lumen of follicles as a colloid. There it undergoes post-translational modification to produce functioning thyroid hormones. Iodide molecules are added to the thyroglobulin precursor to produce the hormones thyroxine and triiodothyronine. Thyroxine is also known as T4 because it contains four atoms of iodine, and triiodothyronine is also known as T3 because it contains three atoms of iodine. In developed countries, the iodide required for hormone synthesis is obtained primarily from iodized salt. However, seafood and plants grown in iodine rich soil at lower elevations also provide the required iodide. Since iodine as a molecule is quite volatile, the food grown in higher elevations (lower atmospheric pressure) lacks sufficient iodine. Iodide ions are actively transported into the follicular lumen from the capillaries by follicle cells. Follicle cells are stimulated to release stored T3and T4 from the lumen into the blood capillaries by thyroid stimulating hormone (TSH), which is produced by the anterior pituitary. Follicle cells also begin synthesizing more T3 and T4 in response to TSH stimulation. A third hormone, calcitonin, is produced by parafollicular cells, or C cells of the thyroid. Calcitonin release is not controlled by TSH, but instead is released when calcium ion concentrations in the blood rise. Calcium ions bind to specific receptor on the C cell and stimulate release of calcitonin. Calcitonin acts primarily in children to lower blood calcium levels when levels get too high. Calcitonin causes decreased tubular reabsorption of Ca2+ in the kidneys, leading to calcium loss in urine. It inhibits bone resorption activity of osteoclasts and calcium absorption in intestine to also reduce plasma calcium levels. It is also suspected to have an indirect effect stimulating osteoblast activity and development. However, in adult humans it appears to play only a minor role in calcium homeostasis because abnormalities in calcitonin production do not appear to be associated with specific plasma calcium imbalances. Research has implicated its role during times of high calcium demands, such as pregnancy and lactation.