Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
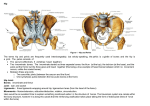
MSK-HIP (Part I) Anatomy and Physical Exam Yibing Li 01/07/2004 Hip Joint The hip joint is a synovial ball and socket joint, formed by the reception of the head of femur into the cavity of acetabulum. It is the largest weight bearing joint in the body and is surrounded by strong ligaments and muscles. Due to high mobility, hip joint pathology can be manifested during weight bearing, ambulation or motion. Hip Bones The ilium, ischium, pubis and femur are the main bones at the hip joints. The ilium, ischium and pubis are fused together to form the pelvis girdle (L+R). Ligaments of the Hip Joints Acetabular labrum forms a complete ring around the head of the femur. Its function is to hold the femoral head in place. The ligament of the head of femur attaches the head of femur to the acetabulum. Ligaments (cont.) There are 3 ligaments that hold the head of femur to the pelvis: 1. Iliofemoral lig.: the strongest ligament; Its function is to prevent hyperextension, abduction and lateral rotation. 2. Pubofemoral lig. : limits abduction 3. Ischiofemoral lig. : limits medial rotation. The Capsule of Hip Joint The articular fibrous capsule extends from the acetabular rim to the intertrochanteric crest forming a sleeve that encloses the hip joint and most of the femoral neck. Hip joint injection Muscles of the hip and thigh Muscles of the Hip & Thigh Inferior Gemelli Obturator Externus Obturator Internus Piriformis Quadratus Femoris Superior Gemelli Gluteal Region (Hip-Joint Stability)Deep Gluteal Region (Hip-Joint Stability)Deep Gluteal Region (Hip-Joint Stability)Deep Gluteal Region (Hip-Joint Stability)Deep Gluteal Region (Hip-Joint Stability)Deep Gluteal Region (Hip-Joint Stability)Deep Ischial Tuberosity Obturator Membrane (external surface) Obturator Membrane (internal surface) Greater Trochanter Femur: Lateral Rotation Greater Trochanter Femur: Lateral Rotation Anterior aspect of the Sacrum Greater Trochanter Greater Trochanter (Superior aspect)Crest Intertrochanteric Femur: Lateral Rotation Femur: Lateral Rotation | Femur: Abduction Ischial Tuberosity (Quadrate Tubercle) Femur: Lateral Rotation Ischial Spine Greater Trochanter Femur: Lateral Rotation Goes through Lesser Sciatic Foramen The big muscle in the gluteal group Directly above the obturator internus Gluteus Minimus Gluteal Region (Hip-Joint Stability)Superficial Gluteal Region (Hip-Joint Stability)Superficial Gluteal Region (Hip-Joint Stability)Superficial Ilium, Sacrum, and Coccyx Outer surface of il eum, between top two gluteal lines Outer surface of Ili um, between bottom two gluteal lines Iliopsoas Thigh, Anterior Lumbar spine and Iliac crest Sartorius Thigh, Anterior Anterior Superior Iliac Spine Tensor Fasciae Latae Proximal femur Vastus Medialis Thigh, Anterior Thigh, AnteriorQuadriceps Femoralis Thigh, AnteriorQuadriceps Femoralis Thigh, AnteriorQuadriceps Femoralis Thigh, AnteriorQuadriceps Femoralis Adductor Brevis Thigh, MedialAdductor Group Pubic Bone Thigh: Adduction Adductor Longus Thigh, MedialAdductor Group Pubic Bone Thigh: Adduction Lateral floor of Femoral Triangle Adductor Magnus Thigh, MedialAdductor Group Pubic Bone Thigh: Adduction | Thigh: Extension Adductor "Hybrid" Muscle Gracilis Thigh, MedialAdductor Group Pubic Bone Pectineus A good spare part; adduction can occur without it. Adductor "Hybrid" Muscle; Floor of the Femoral Triangle Semimembra nosus Thigh, MedialAdductor Group Pubic Bone Long Head: Ischial Tuberosity | Thigh, PosteriorHamstring Short Head: Femur (Linea Muscles Aspera) Thigh, PosteriorHamstring Muscles Ischial Tuberosity NONE | Thigh: Adduction Thigh: Adduction | Hip: Flexion Head of the Fib ula Medial condyle of proximal tibia Hip: Extension; Knee: Flexion Hip: Extension; Knee: Flexion Semitendinos us Thigh, PosteriorHamstring Muscles Medial condyle of proximal tibia Hip: Extension; Knee: Flexion Gluteus Maximus Gluteus Medius Rectus Femoris Vastus Intermedius Vastus Lateralis Biceps Femoris Anterior Inferior Iliac Spine Proximal femur Proximal femur Proximal femur Ischial Tuberosity Gluteal Tuberosity of Femur and Iliotibial Tract Greater Trochanter (Lateral) Greater Trochanter (anterior) Lesser Trochanter of Femur Directly below the obturator internus Hip: Extension Femur: Abduction and medial rotation Femur: Abduction and medial rotation Femur: Flexion at hip Hip: Flexion; Knee: Posteromedial aspect of Extension | Femur: proximal tibia Lateral Rotation Iliotibial Tract Quadriceps Ten don the superior Patella Quadriceps Ten don the superior Patella Quadriceps Ten don the superior Patella Quadriceps Ten don the superior Patella Floor of the Femoral Triangle Knee: Extension Inferolateral base of Femoral Triangle Increases tension of fascia lata and iliotibial tract, esp. when standing upright; holds knee in place Acts on the hip joint; Crucial role in knee stability Knee: Extension Crucial role in knee stability Knee: Extension Crucial role in knee stability Knee: Extension Crucial role in knee stability Hip: Flexion; Femur: Medial Rotation on on on on Long head crosses both hip and knee joints Cross both hip and knee joints Cross both hip and knee joints; medial to semimembranosus Movements at the Hip 1. Flexion / Extension 2. Adduction / Abduction 3. Lateral (external)Rotation / Medial (internal) Rotation Hip Flexors Iliopsoas (prime hip flexor) Pectineus Sartorius Rectus femoris Pectineus Tensor fsaciae latae Adductor brevis Adductor longus Adductor magnus (anterior head) Rectus femoris P90-iliopsoas P96-pectineus Hip Extensors Gluteus maximus Biceps femoris (long head) Semitendinosus Semimembranosus Adductor magnus (postrior head) P86 P100-101 Hamstring Hip Abductors Gluteus medius Gluteus minimus Tensor fasciae latae Sartorius p87 p88 Hip Adductors Adductor brevis Adductor longus Adductor magnus Gracilis Pectineus p97 p98 p99 Internal Rotators of the Hip Gluteus medius Gluteus minimus Tensor fasciae latae Adductor magnus (anterior head) p91 p89 Physical Exam of the Hip and Pelvis Inspection & Palpation ROM Neurologic exam Special tests Inspection Observe gait Check hip and pelvis area for skin abrasions,abnormal swelling, etc. Check if the anterior superior iliac spines are in the same horizontal plane or tilted pelvis Observe the two discernible dimples to check PSIS for pelvic obliquity Gait Antalgic gait: prolonged double support period, decreased stance phase and step length on the unaffected side to reduce pain and avoid weight bearing on the affected side. Trendelenburg gait (hip abductor weakness) ---uncompensated gait: contralateral pelvic drop. ---compensated: lateral lurch over the affected side.(Tx with cane) Extensor lurch gait(gluteus maximus weakness): secondary to inferior gluteal N.injury or subtrochanteric hip fx. Unable to decelerate the hip flexion moment at heel strike due to hip extensor weakness. To compensate, pt lean upper body backward to keep the center of gravity. Tx with two crutches or canes. Palpation ----Anterior Superior Iliac Spines (ASIS): check pelvic obliquity ----Iliac crest ( gluteus and sartorius muscles originate just below it) ----Greater Trochanter (uneven in congenital hip dislocation or poor-healed hip fx) ----PSIS (lie directly underneath the visible dimples just above the buttocks, check for pelvic obliquity) ----Trochanteric Bursa (have pt lie on the side with hip flexion; If it is inflamed, the area feels boggy and tender to palpation) ROM Flexion: 120 degree Extension: 30 degree Abduction: 45-50 degree Adduction: 0-30 degree External rotation: 35 degree Internal rotation: 45 degree (OA limits internal rotation first) Neurologic Exam Muscle testing: test muscle strength in functional groups. Primary flexor: Iliopsoas (femoral N. L1,2,3) Primary extensors: Gluteus Maximus (inferior gluteus N. S1) Primary adductors: Adductor longus (obturator N. L2,3,4) Primary Abductor: Gluteus medius( superior gluteal N., L5) Sensation testing: for example, dermatomes ( T10-L3) Special Hip Tests 1. Patrick (Fabere) test 2. Thomas test 3. Ober test 4. Trendelenburg test 5. Leg length discrepancy Patrick test This test is to assess Flexion, Abduction, External Rotation Perform with pt supine, passively flex and externally rotate and abduct the hip. Ipsilateral inguinal pain indicates pathology in the hip joint or the surrounding muscles. Contralateral pain occurs in the dysfunctional SI joint. Thomas Test To assess hip flexion contractures Perform the test with the pt supine, flex one hip fully reducing the lumbar spine lordosis, stabilizing the spine and pelvis, extend the opposite hip.A flexion contracture is present if the hip cannot fully extend. The degree of flexion contracture can be done by estimating the angle between the table and pt’s leg. Ober test To test for contraction of the fascia lata. Have pt lie on the side with involved leg uppermost. Abduct the leg as far as possible and flex the knee to 90 degree. If the thigh remains abducted, there may be a contracture of the tensor fascia lata or ITB. Trendelenburg test Test for gluteus medius weakness Perform with the pt standing erect, one foot is raised off the floor, strength of the gluteus medius of the supported side is assessed. A positive test occurs when the pelvis on the unsupported side descends or remains level. Conditions with gluteus medius weakness:--radiculopathies,poliomyelitis,meningomyelocele, fx of the greater trochanter, slipped capital femoral epiphysis, congenital hip dislocation. Leg Length Discrepancy (LLD) Leg Length Discrepancy (LLD) True LLD: measure from ASIS to the medial malleoli. The shortening may be due to fx crossing the epiphyseal plate in children or poliomyelitis. To determine the discrepancy from femur or the tibia: (with pt supine, flex the knees to 90 and place feet flat on the table) If the knee is higher than the other, that tibial is longer ; if one knee projects further anteriorly, then that femur is longer. Leg length discrepancy Apparent LLD: (determine no TLLD first)with pt supine, measure from umbilicus to the medial malleoli. Apparent discrepancy may be caused by pelvic obliquities or flexion or adduction deformity of the hip.