Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
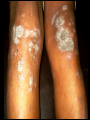
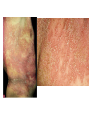
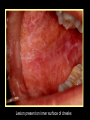
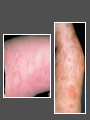
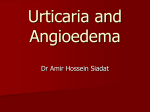
welcome Patient itch/ Itchy Rash-2 Prof. DOULAT RAI BAJAJ Professor & Chairman Dept. of Dermatology Goals of Presentation At the end of presentation you would be able to: 1. Clinically evaluate a patient with itch or itchy rash 2. Make a working diagnosis 3. Manage it at the best Review Last Presentations Evaluation of a patient presenting with itchy rash Aopic Derm, Sebh. Derm. Irritant Contact Dermatitis (ICD) allergic CD, Discoid, LSC, Prurigo, Pompholyx, P.rosea, P. alba, xerotic eczema General Principles of treatment Preventive measures Tasks of Today Psoriasis Lichen Planus Scabies Pediculosis Urticaria Dermatitis herpetiformis PSORIASIS Psoriasis An autoimmune disease characterized by: Well defined, erythematous, plaques Bilateral Symmetrical distribution Silvery scales, varying thickness Predilection for Extensor aspects May be associated Joint involvement Runs a very chronic course with remissions and relapses Auspitz Sign Psoriasis contd…. May occur from infancy to very old age. Mostly b/w ages of 15 & 35 yrs M: F affected equally. Same phenotype in both sexes Koebner Phenomena: Psoriasis may develop @ sites of trauma, e,g, Scratch mark, Injury, Surgical incision, Friction from tight-fitting clothing/obesity Sun burn Kobner Phenomena Etiology: Actual etiology unknown. Predisposing Factors: Genetic Factors Environmental Factors Genetic factors HLA Cw6 Familial occurrence: 14% if one parent affected 41% if both parents affected 06% if one sibling affected 02% when no parent/sibling affected Environmental: Trauma: Dry Physical, Chemical, Electrical, Surgical skin Infections: Streptococcal, HIV Sunlight : may relieve or exacerbate Hypocalcemia: Drugs: Lithium, Antimalarials, β-blockers, NSAIDs, ACEIs, Terbinafine, Ca Chanel Block Withdrawal of corticosteroids Psychogenic factors Smoking, Alcoholism Clinical Types Psoriasis vulgaris Guttate psoriasis Rupoid, Elephantine & ostraceous Unstable psoriasis • Erythrodermic psoriasis • Pustular psoriasis Psoriasis Vulgaris Guttate Psoriasis Generalized shower of small “rain drop” like deep red papules ē fine scaling. Most common form in children. Acute onset: Usually follow 3/4 wks off strept. pharyngitis. Recurrent, b/c of pharyngeal carriage of streptococci. Mainly trunk, sparing face, palms & soles. Management It includes General measures Local therapy Intralesional therapy UV phototherapy Systemic therapy Lasers 5/24/2017 33 GENERAL MEASURES Attention should be paid to general, physical & psychological health. Rest & mild sedation Stress alleviation Stop smoking, alcohol, drugs Spa therapy DIET 5/24/2017 34 Local Therapy Keratolytics: salicylic acid Tar: 2-10% Dithranol: 0.05-4% Corticosteroid Vitamin D analogue: calcipotriol, calcitriol, tacalcitol Vitamin A analogue: Tazarotene Topical tacrolimus 5/24/2017 35 Photo chemotherapy Combination of psoralens & UVA. Moderate to severe psoriasis. It is one of the standard treatment b/c: Effective, long term effect. ORAL 8-MOP = 0.6 mg /kg or 5-MOP UV radiation/laser light 2 hours later UVA dosage depends upon skin type. frequency: 2-4 times weekly (for 15-25 min.). 5/24/2017 36 Systemic therapy Methotrexate Hydroxyurea Oral retinoids: Etretinate Isotretinoin Acetretin Cyclosporin Systemic steroids. Biological Therapies Methotrexate MOA: Inhibits DNA synthesis by inhibiting DHFR Start ē 7.5-15 mg/wk in single/divided × 3, given 12 hrly over 36 hrs. Inc 2.5 mg every 2-4 wk, Max: 30mg/wk Folic acid supplement 5mg daily (on days without Mtx) Monitor ing : Hepatic, renal & marrow function. Routine liver biopsy. Avoid concurrent therapy ē NSAIDS, sulpha, ASA & Septran b/c they displace MTX from plasma albumin Ciclosporin Antilymphocytic, inhibition of T-lymphos. Start with 2.5 mg/kg BID, for 2 wks. No response to 5mg/kg/day. Use for short courses of 3-4 months. S. E. Renal toxicity. HTN Malignancies: CIN (females), PIN (males), cut.lymphoma Hypertrichosis Gum hyperplasia Biochemical: serum K+, serum uric acid. serum Mg+ Retinoids: Etretinate & Acetretin Synthetic analogues of Vit. A. Acitretin is active metabolite of etretinate, ē ½ life of just 50 hrs VS ≥ 80 days for etretinate. Best results when combined ē UVA (PUVA) Dose: 0.7-1mg/kg/d Protocol: Contraception during & up to 2 yr after stopping Rx. Lipid profile & LFT, CBC ē platelets, Renal profile Lichen planus LICHEN PLANUS A chronic papulosquamous disorder characterized: plane topped Polygonal Purple papules which are highly pruritic Surface may show white lines: Wickham’s Stria Etiology: Exact etiology unknown. Genetic, immunological Plane topped polygonal purple color papules Papules appear in group Size ranges from pinpoint to centimeter SITES Most common sites: wrists, lumbar region & around ankle. May occur any where on body Ankles & shins are the most common sites for hypertrophic LP Hypertrophic lesions around ankle Hypertrophic lesions present on shin MUCOSAL INVOLVEMENT Mucosal lesions very common, mostly seen on buccal mucosa & tongue. White lacy streaks on inner surface of the cheeks, gum margins and lips: a very common finding Mucosal Lesions include White streaks Fixed white patches Ulcerative lesions Streaks of pigmentation LP involving buccal mucosa Lesion present on inner surface of cheeks White streaks present on lips White streaks on tongue Drug Induced LP: COMMON INDUCERS Gold salts β-blockers Antimalarials Thiazide diuretics Frusemide Spironolactone penicillamine LESS COMMON INDUCERS ACEIs Calcium channel blocks Ketoconazole Tetracyclines Phenothiazine CLINICAL & H/P Difference b/w IDIOPATHIC & DRUG induced LP PRESENTATIONS IDIOPATHIC LP Drug Induced lesions Smaller Larger and scally Wickhams striae Usually present Usually absent Alopecia Uncommon Common Residual hyperpigmentation Possible common MM involvement Very common Less common Parakeratosis Not seen common Cystoid in granular layer Very common common TREATMENT TOPICAL STERIODS: Flucinonide 0.05% Clobetasol propionate 0.05% FOR PRURITIS: Promethazine HCL Trimeperazine tartrate Brom-pheneramine maleate TREATMENT SYSTEMIC STEROIDS: Oral prednisolon 15-20mg/d for about 6 wks for severe cases. For cutaneous and erosive LP Acetretin Itraconazole Metronidazole PUVA TREATMENT FOR ORAL LESIONS: Lidocain gel triamcinolone in orabase Corticosteroids lozenges Betamethasone mouth washes Fluticasone propionate spray Oral or systemic CYCLOSPORIN used to treat ulcerative form of LP Scabies Scabies Caused by Sarcoptes scabiei var humanis Acquired through close personal contact (not casual), but may be transmitted through clothing, linen, furniture or towels. Sexual transmission as common as non-sexual Suspect scabies when several members of a family complain of itching Clinical Features: The IP <1 month (max: 2 months) Severe itching: prominent symptom Nocturnal Pruritus first noticed 3-4 wks after primary infection, but occurs sooner after subsequent attacks. May be localized initially to burrow, but later becomes generalized. Burrow is the diagnostic lesion: Multiple straight or Sshaped ridges or dotted lines resembling thread, 5-20 mm long Sites: interdigital webs of hands wrists, anticubital fossae, points of elbow nipples Around the umbilicus, lower abdomen Genitilia Gluetal cleft Lesions on glans penis→ Characteristic in males Infants & small children: lesions on palms, soles, head & neck. Generalized urticarial papules, excoriations & eczematous changes common in children Indurated erythematous nodules, most noticeable on male genitalia → more common. Sec: bacterial infection: Impetiginization, furunculosis DIAGNOSIS H/O of pruritis with nocturnal exacerbations. Positive family history. Distribution of lesions In doubtful cases confirm by microscopy Polymerase chain reaction has been employed in difficult diagnostic and atypical cases. Treatment General Measures: Improve general hygiene frequent bathing Trim down nails avoid close contact with active case Observe caution when caring/nursing patient keep personal utensils and towels separate Treat all family members at a time Drugs Topical Treatment is the gold standard & very effective Topical Permethrin 5%: lotions, creams Gamma benzene hexa chloride: Benzyl benzoate Sulphur 10% Malathione: NA Oral Ivermectin: efficacy??? URTICARIA Definition Urticaria characterized by weals: transient, well-demarcated, superficial erythematous or pale swellings of the dermis, usually associated with itching While angioedema is a transient swelling in deep dermis, subcutaneous & submucosal tissue. • Usually painful • Poorly defined • pale or skin colour Urticaria and Angioedema Urticaria Angioedema PATHOGENESIS Urticaria not a single disease: A REACTION PATTERN mediated by HISTAMINE Mast Cells/Basophils play cardinal role. Their activation by various factors/agents/stimuli with subsequent release of MEDIATORS leads to clinical symptoms/signs. Acute urticaria & chronic urticaria are not single entity. Clinically it is useful to d/b the two to make proper clinical decisions. CLASSIFICATION classification According to duration of disease According to clinical features DURATION OF DISEASE Acute urticaria Chronic urticaria ≤ 06 weeks Cause can be found in in approx. 50%; by history Good prognosis ≥ 06 weeks workup indicated often persistent Chronic idiopathic urticaria - subset of chronic urticaria in which workup fails to pinpoint cause; diagnosis by exclusion; not homogeneous. ORDINARY URTICARIA Start as itchy erythematous macules Wheal Pale to pink with surrounding red flare. Duration: few hrs to several days, no sequelae Very itchy but pts. tend to rub rather than scratch Size: few mm to many cms Shape: round ,annular, bizarre. Angio oedema associated ē 50% of cases Sites: face, eye lids lips, ears, neck, hands, feet, genitalia, buccal, tongue, pharynx & larynx Acute ordinary urticaria: ≤ 6 weeks. Types Allergic Non-allergic ALLERGIC URTICARIA (IgE mediated) A reaction B/W an allergen with specific IgE antibody bound to mast cell Common in atopic persons with raised IgE levels Substances causing urticaria Penicillin Cephalosporin Insulin vaccines Blood products Bee and wasp strings Foods causing AU Lobsters, shrimp, crab Milk nuts Fish Beans Potato Carrots Spices Rice Banana Apple Orange Non allergic Acute urticaria from ingested substances may be non-allergic. They are referred to as intolerance reaction. Due to direct histamine release from mast cell Substances causing non allergic urticaria Drugs Aspirin, Other NSAIDs Polymyxin, ciproxin, rifampsin ,vancomycin. Radio contrast media Plasma expanders General anaesthetic agents Infections Epstein bar virus, Hepatitis B virus Strept. sore throat in children Etiology: D/B Acute VS Chronic Acute Urticaria Drugs Foods Chronic Urticaria Physical factors –Cold, heat, solar, pressure Ch. Viral, bacterial, fungal infect chronic yeast infection autoimmune: SLE, DLE, DM, SS Food additives Viral: Hep: A, B, C, EBV Insect bites and stings Complement deficiency Animal dander and latex Malignancies: Lymphoma, leukemia Idiopathic Initial Workup of Urticaria Patient history URTIs: Sore throat, Sinusitis, pharyngitis Arthritis Thyroid disease Cutaneous fungal infections UTI symptoms Travel history (parasitic infection) EBV infectious mononucleosis Insect stings Foods Recent transfusions Recent intake of drugs Physical exam Skin Eyes Ears Throat Lymph nodes Feet Lungs Joints Abdomen Lab: Assessment for Chronic Urticaria Initial tests CBC with differential ESR Urinalysis Tests for selected patients Stool exam. for ova, parasites, giardia Blood chemistry profile Antinuclear antibody titer (ANA) Complement studies: CH50 Cryoproteins Hepatitis B and C Skin prick tests (IgE-reactions) T3, T4, TSH, Thyroid antibodies RAST for specific IgE Treatment: Pharmacologic Options Antihistamines, others First-generation H1 Second-generation H1 Antihistamine/decongestant combinations Tricyclic antidepressants (eg, doxepin) Combined H1 and H2 agents Beta agonists Epinephrine 1:10,000; 0.5-1ml S/C: angioedema, sever acute urticaria Terbutaline Corticosteroids Severe acute urticaria –avoid long-term use –use alternate-day regimen when possible Avoid in chronic urticaria (lowest dose plus antihistamines might be necessary) Miscellaneous PUVA Hydroxychloroquine Thyroxine H1-Receptor Antagonists: Pros and Cons for Urticaria and Angioedema First-generation antihistamines (diphenhydramine, hydroxyzine) Advantages: Rapid onset of action, relatively inexpensive Disadvantages: Sedating, anticholinergic effects Second-generation antihistamines (astemazole, cetirizine, fexofenadine, loratadine) Advantages: No sedation (except cetirizine); no adverse anticholinergic effects Disadvantages: Prolongation of QT interval; ventricular tachycardia (astemizole only) in a patient subgroup Dermatitis Herpetiformis Very pruritic condition Characterized by: crusted, excoriated papules and vesicles. Vesicles very seldom seen Widespread on back of trunk, head, elbows Occur in all age 22 – 55 years Sites : Elbow, knee, shin, scapulae & buttocks Patient may have gastrointestinal symptoms OR systemic signs of gluten sensitivity/CD. Dermatitis herpatiformis Pruritus with Systemic Diseases Systemic Diseases Thyroid: hypothyroidism, hyperthyroidism, Hashimoto’s thyroiditis Ch. Liver Diseases: cirrhosis, CAH, PBC Renal : CRF especially with dialysisis Blood: Anemia, Polycythemia Metabolic: Diabetes, HIV, AIDS Malignancies: lymphoma, leukemia, internal malignancies Characteristic Features There are minimal cutaneous lesions If present; these are non-specific, no predilection for site Mostly there are dry papules broken in centre OR dispersed excoriations S/S of systemic diseases are Dominant in whole clinical picture Some specific features may be seen (next slide) Prognosis depends upon the prognosis of underlying disease Specific features of Systemic Ds Liver Ds: xerosis, diffuse melanosis, red palms, spiders, gynaecomastia(males), edema, icteric Diabetes: xerosis, loose wrinkled skin, acanthosis, skin tags, pyodermas, carbuncles, candida Renal: xerosis, uremic frost, perforating lesions, calcinosis, vasculitic lesions Thyroid: xerosis, alopecia, madarosis, wrinkling in Hypo; general flush, sweaty palms, angiomas, fine atrophic skin in Hyperthyroidism AIDS: prurigo, urticaria, SD, cutaneous & mucosal candida Blood: general pale, lethargic look in anemia, suffused, congested bronze skin in polycythemia THANK YOU Superior doctors prevent the disease Mediocre doctors treat the disease before evident Inferior doctors treat the full-blown disease Huang Dee Nai-Chan. 2600 BC; 1st Chinese Medical Text See This presentation @ www.lumhs.edu.pk/DFHC/html