Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
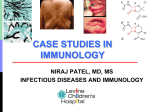
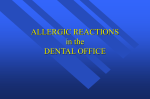
Diagnostic Approach and Treatment of Urticaria and Angiodema: An Update Jonathan A. Bernstein, M.D. Professor of Clinical Medicine Division of Immunology/Allergy Section Conflict of Interest Disclosures: Jonathan A. Bernstein, MD FACAAI, FAAAAI Employment: University of Cincinnati and Bernstein Allergy Group and Clinical Research Financial: CSL Behring; Dyax; Shire; Teva, Viropharma Research: CSL Behring; Dyax; Pharming; Shire; Viropharma, Novartis Legal: Nothing to disclose Organizational: AAAAI; ACAAI; AFI Gifts: Nothing to disclose Other: Editor in Chief Journal of Asthma Objectives: Upon completion of this lecture the participant should be able to: • Identify the differential diagnosis of urticaria and angioedema • Explain the appropriate laboratory evaluation of urticaria and angioedema • Describe the conventional treatment approach for urticaria and angioedema WORLD ALLERGY ORGANIZATION POSITION PAPER DIAGNOSIS AND TREATMENT of URTICARIA AND ANGIOEDEMA: A WORLDWIDE PERSPECTIVE Mario Sánchez-Borges 1, Riccardo Asero 2, Ignacio Ansotegui 3, Ilaria Baiardini 4, Jonathan A. Bernstein 5, G Walter Canonica 4, Richard Gower 6, David A Kahn 7, Allen P Kaplan 8, Connie Katelaris 9, Marcus Maurer 10, Hae Sim Park 11, Paul Potter 12, Sarbjit Saini 13, Paolo Tassinari 14, Alberto Tedeschi 15, Young Min Ye 11, Torsten Zuberbier 10 The Diagnosis and Management of Acute and Chronic Urticaria: 2012 Update Chief Editors Jonathan Bernstein, MD and David Lang, MD Workgroup Contributors Timothy Craig, DO; David Dreyfus, MD; Fred Hsieh, MD; David Khan, MD; Javed Sheikh, MD; David Weldon, MD; and Bruce Zuraw, MD Task Force Reviewers David I. Bernstein, MD; Joann Blessing-Moore, MD; Linda Cox, MD; Richard A. Nicklas, MD; John Oppenheimer, MD; Jay M. Portnoy, MD; Christopher R. Randolph, MD; Diane E. Schuller, MD; Sheldon L. Spector, MD; Stephen A. Tilles, MD; and Dana Wallace, MD Features of Urticaria Raised, pink/erythematous skin lesions that are markedly pruritic; lesions range from a few millimeters to several centimeters in size and may coalesce Evanescent; old lesions go and new ones come over 24 hours leaving no scarring Generally worsened by scratching Any area of the body may be involved; most common areas are the perioral and periorbital regions, tongue, genitalia and extremities Prevalence of Urticaria Estimated to occur in 15-23% of the U.S. population Up to 40% of patients who have chronic urticaria longer than six months will still have urticaria 10 years later Approximately 40% of patients with chronic urticaria have angioedema Prevalence of Urticaria With and Without Angioedema Urticaria Acute urticaria refers to hives lasting less than six weeks; in approximately 15-20% of cases an inciting cause can be identified Chronic urticaria refers to hives lasting longer than 6-8 weeks; identification of a cause is less than 5% Differential Diagnosis: Immunologic Causes More Often Responsible for Acute Urticaria Foods Many drugs Insect stings Transfusion reactions Contactants/Inhalants (rare) Differential Diagnosis: Non-Immunologic Causes More Often Responsible for Chronic Urticaria Physical hives (i.e., dermatographism, pressure, solar, cold…) Hereditary (i.e., cold, heat, vibratory, porphyria, C3b inactivator deficiency…) Vasculitis Neoplasms Infections Endocrine Drugs (i.e., aspirin/NSAIDs-exacerbate hives in up to 30% of cases) Psychologic? More a myth than fact Most CU is Idiopathic • SUMMARY STATEMENT 13: Evaluation of a patient with CU should involve consideration of various possible causes. Most cases do not have an identifiable cause [C] Features of Physical Urticaria Type Age (yrs) Clinical Features Angioedema Diagnostic Test Dermatographism 20-50 Linear lesions No Light stroking of skin; + transfer factor Cold (primary vs. secondary) 10-40 Itchy, pale lesions (5% with cryos) Yes 5-10 minute ice-cube test; + transfer factor Cholinergic (heat bumps) 10-50 Itchy, monomorphic pale or pink lesions Yes Exercise or hot shower; + transfer factor Pressure 20-50 Large painful or itchy lesions No Dermographometer; application of pressure to skin or Sand bag test 15 lb weight for 15 minutes Solar 20-50 Itchy pale or red swelling Yes Irradiation by a solar simulator;+ transfer factor sitesearch: exact match: © 2002 by DermIS - Dermatology Information System O X X X X O O sitesearch: exact match: © 2002 by DermIS - Dermatology Information System Familial Cold Urticaria (aka. Familial Cold Autoinflammatory Syndrome) Autosomal dominant Characterized by episodic urticaria, arthralgias, fever and conjunctivitis after exposure to cold Same genetic locus on chromosome 1q44 as Muckle-Wells syndrome (an autosomal dominant periodic fever syndrome associated with hives and sensorineural hearing loss) Cryopyrin gene preferentially expressed in families with this disorder; significant homology to the Nod2 gene implicated in Crohn’s disease Hoffman HM, et.al. Nat Genet 2001; 29:301-5. lesion description opaleness owheal opurpura opale red opolycyclic additional description Urticarial Vasculitis: Features That Differentiate It From CIU Feature Chronic urticaria Urticarial vasculitis Wheal duration <24 hr >24 hr (not always true) Purpura/pain/hyperpigmentation No Yes Systemic signs Usually none Yes Laboratory findings Usually normal Increased WSR, Acute Phase Reactants; Decreased C3/C4 Leukocytoclasia or extravasation of RBCs No Yes Response to antihistamines Yes Sometimes Chronic Urticaria: The Evaluation History and Physical Examination 1. Onset (e.g. timing of symptoms with any change in medication or other exposures). 2. Frequency, duration, severity, and localization of wheals and itching. 3. Dependence of symptoms on the time of day, day of the week, season, menstrual cycle, or other pattern. 4. Known precipitating factors of urticaria (e.g. physical stimuli, exertion, stress, food, medications). 5. Relation of Urticaria to Occupation and leisure activities. 6. Associated angioedema, systemic manifestations (headache, joint pain, gastrointestinal symptoms, etc.) 7. Known allergies, intolerances, infections, systemic illnesses or other possible causes. 8. Family history of urticaria and atopy. 9. Degree of impairment of quality of life. 10. Response to prior treatment. 11. General physical examination. Laboratory Evaluation • Routine evaluation: There is no consensus regarding the appropriate tests which should routinely be performed for patients with CU without atypical features by history or physical exam. • Commonly performed tests are: • CBC with differential • Sedimentation rate and/or C-reactive protein. • Some clinicians routinely perform: • Chemistry panel • Hepatic panel • TSH • Anti-microsomal antibodies, anti-thyroglobulin antibodies Evaluation (Cont.) Possible additional evaluation warranted by elements of history or physical exam which would make these tests appropriate: Functional autoantibody assay (for autoantibodies to FcεRIά) and/or autologous serum or plasma skin testing Complement system: e.g. C3, C4, and CH50 Stool analysis for ova and parasites H. pylori workup (limited experimental evidence to recommend this) Hepatitis B and C workup Chest radiograph and/or other imaging studies Antinuclear antibody (ANA) Rheumatoid factor Cryoglobulin levels Serologic and/or skin testing for immediate hypersensitivity Physical challenge tests Skin biopsy Urinalysis Recommendations on Specific Tests • Testing not indicated on routine basis – Autoimmune serology (SS #15) – Testing for H pylori or celiac disease (SS #19) – Thyroid Autoantibodies (SS #30) – CU Autoantibody Tests (SS #31) – Skin Biopsy (SS #34) – Hypersensitivity Testing (e.g. skin testing) (SS # 35) • Retrospective study to investigate the proportion of abnormal test results in patients with CU leading to a change in management and in outcomes of care • 356 CU pts seen at Cleveland Clinic Tarbox JA et al. Ann Allergy Asthma Immunol 2011;107:239 –243. 17% of 1,872 ordered tests were abnormal Tarbox JA et al. Ann Allergy Asthma Immunol 2011;107:239 –243. 1/356 (0.28%) benefitted from testing! 1 patient with hypothyroidism with normal TSH and elevated microsomal AB responded to higher dose thyroxine Tarbox JA et al. Ann Allergy Asthma Immunol 2011;107:239 –243. Diagnostic Testing in CU • SUMMARY STATEMENT 29: After a thorough history and physical examination, no diagnostic testing may be appropriate for some patients with CU; however, limited routine lab testing may be performed to exclude underlying causes. Targeted lab testing based on clinical suspicion is appropriate. Extensive routine testing for exogenous and rare causes of CU, or immediate hypersensitivity skin testing for inhalants or foods, is not warranted. Routine laboratory testing in patients with CU, whose history and physical examination lacks atypical features, rarely yields clinically significant findings.[C] Conventional Therapy of Chronic Urticaria Antihistamines in Chronic Urticaria • Nearly all symptoms of urticaria are primarily mediated by H1-receptors located on nerves and endothelial cells • H1 antagonists mainstay of therapy for most all chronic urticaria International Consensus Meeting on Urticaria • “The recommended first line treatment is new generation, nonsedating H1antihistamines.” • level of evidence: high quality • strength of recommendation: strong Allergy 2009;64:1427-43. High Dose Antihistamines in CU • Cetirizine: conflicting studies • Fexofenadine: no difference between 60 mg, 120 mg and 240 mg twice a day • Desloratadine – 20 mg > 5 mg in cold urticaria • Levocetirizine and desloratadine – Higher doses better Kavosh ER, Khan DA. Am J Clin Dermatol 2011 Dec 1;12(6):361-76. High Dose Antihistamines in CU Staevska M, Popov T et al. J Allergy Clin Immunol 2010;125:676-82. Response to Antihistamines in CU • Study of 390 urticaria patients from general dermatology or urticaria clinics, majority of which had CU • 297 had evaluable treatment outcomes with antihistamines – 58% had good response – 20% had partial relief – 22% had no benefit • More likely to have physical urticaria or NSAID exacerbated CU Humphreys F et al. Br J Derm 1998: 138: 635-638. Antihistamine Resistance in CU • Definition – Fail despite high doses of antihistamines – Unable to tolerate higher doses of antihistamines Systemic Corticosteroids in CU • Systemic corticosteroids are frequently used in patients with CU refractory to antihistamine therapy • No controlled trials have demonstrated the efficacy of systemic corticosteroids in CU • “systemic corticosteroids should be avoided for longterm treatment of CU, since dosages necessary to suppress symptoms are usually high with significant adverse effects” (International Consensus Meeting on Urticaria) Allergy 2009;64:1427-43. Alternative Agents in Urticaria • Alternative agents for CU are therapies used for patients failing conventional (i.e. antihistamine) therapy • Alternative agents have a variety of mechanisms • • • • Antiinflammatory Immunosuppressant Immunomodulatory other Evidence for Alternative Therapies in CU • Overall the evidence for most alternative therapies is weak • Few agents have well designed randomized placebo-controlled studies • Most studies have small number of participants Khan DA. In: Maibach HI, Gorouhi F ed. Evidence Based Dermatology 2nd ed. 2011 Natural Course/Prognosis of Chronic Urticaria Kozel MM, et.al. J Am Acad Dermatol 2001;45:387-91 220 adults with chronic urticaria were followed prospectively for 1-3 years at the University of Amsterdam After one year, 35% were free of all symptoms and 30% had decreased symptoms 47% of patients with CIU had spontaneous remission over 3 years compared to only 16% who had a component of physical urticaria Conclusion: Prognosis for spontaneous remission of chronic urticaria is reasonable with the exception of the subgroup with a physical component Conclusions • • • • Chronic Urticaria and/or Angioedema is common A thorough history and physical exam is essential Should consider a broad differential diagnosis The initial laboratory evaluation of patients should be limited unless history dictates otherwise • Outcomes are variable but generally good if appropriate evaluation and treatment algorithms are followed