Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
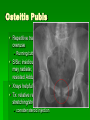
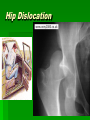
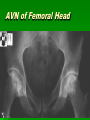
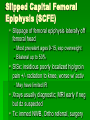
Hip, Pelvis and Thigh Problems: Anatomy, Evaluation and Management Kevin deWeber, MD, FAAFP Director, Sports Medicine Fellowship USUHS Family Medicine (credits to LTC Erik A. Dahl MD for some slides) Objectives Review pertinent hip, pelvis and thigh anatomy Describe clinical presentation of injuries Review best examination techniques for the hip Briefly outline treatment for common conditions Hip Examination Anatomy History Physical Examination Radiology and Laboratory BONY ANATOMY Hip Capsule Ligaments Iliopsoas bursa Bursae Trochanteric bursa Between the greater trochanter and ITB Ischial bursa Between the ischial tuberosity and the overlying gluteus muscle Iliopsoas bursa Between the iliopsoas tendon and the lesser trochanter, extending upward into the iliac fossa beneath the iliacus muscle Largest bursa in the body Hip - Anatomy Multiaxial ball & socket joint Acetabulum 1/2 sphere Femoral head 2/3 sphere Strong ligaments & capsule Maximally stable History Age infancy: congenital hip dysplasia 3-12 year old boys: Legg-Calve-Perthes, SCFE, acute synovitis middle age & elderly: osteoarthritis Mechanism of injury land on outside hip land on knee repetitive loading History Pain details location snapping progression of symptoms exacerbating factors alleviating factors Weakness Occupation, Sport Observation Gait Posture Balance Limb position shortened, adducted, medially rotated abducted, laterally rotated shortened, laterally rotated Leg shortening Inspection Pelvic unleveling (iliac crest levels) Pelvic rotation (PSIS levels) If asymmetric, measure leg lengths Leg Length Measurements Eyeball method Measurement method Anterior Palpation Iliopsoas bursa Posterior Palpation Sciatic nerve palpation Range of Motion: pearls Quick screen w/ Log-roll IR/ER: pain may be from intra-articular fracture, synovitis, or infection Decreased IR: First plane to be painful in OA Range of Motion Flexion: 110 to 120 degrees Extension: 10 to 15 degrees Abduction: 30 to 50 degrees Adduction: 30 degrees External rotation: 40 to 60 degrees Internal rotation: 30 to 40 degrees Examination Strength testing isometric eccentric knee extension knee flexion Hip Flexion Strength Iliopsoas, rectus femoris, sartorius, tensor fascia lata, pectineus Hip Extension Strength Hamstrings, gluteus maximus Hip Adduction Strength Adductor longus, adductor brevis, adductor magnus, gracilis, pectineus, oburator externus Hip Abduction Testing Gluteus medius, gluteus minimus, tensor fascia lata Internal Rotation Strength Gluteus medius, gluteus minimus, tensor fascia lata External Rotation Strength Piriformis, Obturator internus & externus, Superior/inferior Gemelli, Quadratus femoris, Gluteus maximus Abdominal strength Special Tests Patrick’s Test (FAbER) hip joint SI joint Gaenslen’s Sign Pain at ipsilateral SIJ is positive test Special Tests modified Thomas Test hip flexor and quad flexibility Special Tests Ober Test iliotibial band flexibility Special Tests Piriformis Test Piriformis flexibility or pain Special Tests Popliteal Angle Hamstring flexibilty Special Tests Labral Injury FAdAxL: flexion, Adduction, Axial Load + some IR/ER pain +/- click True Hip Pain Misdiagnosis Common The patients studied by Lesher's team received hip injections for pain. Prior to hip injecton, patients told doctors where they felt pain: Buttocks: 71% Thigh: 57% Groin: 55% Lower leg: 22% Foot: 6% Knee: 2% SOURCE: John Lesher, M.D. 22nd Annual Meeting of the American Academy of Pain Medicine, San Diego, Feb. 22-25, 2006. News release, American Academy of Pain Medicine. Think outside the pelvis! Abdominal exam Obturator and Iliopsoas signs Back exam Pelvic exam in females Hip joint problems can radiate to KNEE Diagnostic Imaging Radiographs Anterior-Posterior view Frog leg view STANDING films to r/o early OA Bone scan: stress fxs CT: subtle fractures MRI: soft tissue, stress fx Arthrogram: labral tears Approach to hip problems Better anatomy knowledge better diagnoses Differentiate Anterior, Lateral, and Posterior Hip Pain Develop an appropriate differential based on the location and the exam Consider AGE in DDx Margo K, et al. Evaluation and management of hip pain: An algorithmic approach J Fam Pract. 2003, 52:8 Common Hip Problems by Age Newborn – Congenital dislcation of hip Age 2-8 – AVN of hip (Legg-CalvePerthes), sysnovitis Age10-14 – Slipped Cap Fem Epiphysis Age 14-25 – Stress Fracture Age 20-40 – Labral Tear Age >40 – Osteoarthritis Anterior Hip Pain Differential Dx Osteoarthritis Muscle strains or tendinopathy Stress fracture (femoral neck, pubis) Sports “hernia” Osteitis pubis Acetabular labral tears Obturator or ilioinguinal nerve entrapment Meralgia paresthetica (may be lateral) Inflammatory arthritis Iliac crest apophysitis AVN of femoral head Lateral Hip Pain Differential Dx Greater trochanteric bursitis ITB Meralgia paresthetica OA, labral tear, AVN TFL or gluteus medius strain Posterior Hip Pain Differential Dx Lumbar spine disease and radicolopathy Eval for “red flags” Sacroiliac joint disorders Hip extensor strain or tendinopathy Glut max, hamstrings External rotator strain Piriformis strain or “syndrome” Aortoiliac vascular occlusive disease (rare) Specific Conditions Osteitis Pubis Repetitive trauma to pubic symphysis due to overuse Running/cutting, esp soccer, football, basketball S/Sx: insidious onset dull anterior groin pain; may radiate; TTP over PS; +/- pain w/ resisted Adduction or passive Abduction Xrays helpful Tx: relative rest, brief NSAID, cross-tng, stretching/strength rehab, consider steroid injection Hip Pointer Contusion to the iliac crest S/Sx: pain, swelling, and ecchymosis severe limit to motion +/- palpable hematoma Xrays to r/o fractures TX: rest, ice, compression, ?benefit from steroid/lido inj after acute phase, progressive ROM, strength rehab RTP: padding over area Piriformis Syndrome Pain due to sciatic nerve compression at piriformis Cause: trauma, prolonged sitting, overuse; anomalies in 15-20% S/Sx: dull buttock pain +/- radiation into leg TTP over mid-buttock Pain worse with passive IR or resisted ER -Tx: relative rest, ER stretching, +/- steroid injection Trochanteric bursitis Causes: friction between IT band, glut medius/minimus/max and greater trochanter; common in running w/ improper biomechanics and overtraining direct blows S/Sx: local pain, tenderness over the greater trochanter Eval for leg length discrep, adductor/abductor muscle imbalance, hyperpronation Tx: relative rest, ice, brief NSAID, ITB stretching, +/- steroid injection Address biomechanical defects above Ischial bursitis Cause: excessive friction over ischial tuberosity, or direct blow (hematoma, scarring) S/Sx: pain with sitting, TTP over ischial tuberosity, pain w/ passive hip flexion and active/resistive hip extension Xray to r/o fractures in traumatic hx Tx: Ice, padding, brief NSAID Prolonged: steroid injection Refractory: surgical excision Iliopsoas bursitis Cause: overuse of hip flexors S/Sx: anterior hip pain, +/- snap preferred position of hip in flex/ER, TTP to deep palpation anteriorly, pain with passive hip extension Tx: relative rest, ice, brief NSAID, stretching of iliopsoas, +/- steroid injection (preferably w/ guidance) Sports “hernia” TTP lower abd wall No palpable hernias Co-incident injuries Adductor tendinopathy Osteitis pubis Imaging: consider MRI to r/o other conditions Dynamic US helpful? Tx: relative rest, flexibility, strength surgery if refractory Muscle strains Adductors, gluteals, quads, hamstring tears usually from overstretching during eccentric contraction, esp when muscle fatigued Risk factors Early in season Muscle imbalance, inflexibility, inadequate warmup S/Sx: localized pain and TTP, +/- swelling or ecchymosis , rarely palpable muscle defect, and decreased ROM Graded I, II, III similar to sprains Xrays to r/o avulsion fxs if near muscle origins; MRI if suspected complete tear Tx: PRICEMM, Rehab (ROMstrengthcardiosport-specific tng) Quadriceps Contusions Direct blow to muscle causes tissue damage S/Sx: localized TTP, +/-ecchymosis Grade I: knee flexion >90 Grade II: knee flexion 45-90 Grade III: knee flexion <45 Tx: PRICE; avoid NSAID 48 hrs Max knee flexion, wrap in place 24 hrs Crutches, gradual WB, rehab (ROMstrength) RTP when FROM, 90%+ strength, activity w/o pain Complications: Compartment syndrome (acute) Myositis ossificans (chronic) Slowly enlarging mass, redness, increasing pain Xrays + 3-4 weeks, BS/US sooner Stress Fractures Caused by repetitive overuse stresses RF’s: training errors, females, inadequate footwear, intrinsic factors Pelvic, femoral neck, femoral shaft S/Sx: insidious pain w/ activity; +/- local TTP or pain w/ hop test, +/- decreased ROM Xrays first, MRI or BS if neg but suspected Tx Femoral: immediate NWB, Ortho referral Tension sidesurgery Pelvic/femoral shaft: painless relative rest; graduated WB, strength/stretching rehab, address other RF’s Hip fractures Most common through femoral neck, various traumatic causes S/Sx: pain, swelling, and loss of function Involved leg shortened and externally rotated Tx: Ortho referral, surgery Hip Dislocation Femoral head usually goes posteriorly common mechanism: knee to dashboard during traffic collision S/Sx: extreme pain, obvious deformity, unwilling to move the extremity; position typically flexion, adduction, and internal rotation (FAdIR) Tx: emergent reduction in ER under sedation (Ortho STAT!) AVN of Femoral Head Causes: Trauma: fxs, hip dislocation, surgery Medical conditions (numerous) S/Sx: nonspecific hip pain, may radiate to knee; exam may be relatively unremarkable, with decr IR/ER as dz advances Xrays usually diagnostic >3mo duration; MRI or BS if normal Tx: make pt NWB and refer to Ortho Conservative tx vs hip replacement depending on severity Conditions in adolescents and children Pelvic Apophysitis THE PHYSICIAN AND SPORTSMEDICINE - VOL 29 - NO. 1 - JANUARY 2001 Pelvic Apophysitis Cause: overuse at tendinous insertion at apophysis Iliac crest > ASIS, AIIS, lesser troch, greater troch, ischial tuberosity S/Sx: localized pain, TTP, pain w/ passive stretch of attached muscle Xrays to r/o avulsion fxs Tx: relative rest (rare crutches), ice, brief NSAID?, cross training, strength rehab, flexibility Pelvic Avulsion Fractures Caused by violent contraction of the attaching muscle in skeletally immature athlete Sprint, jump, soccer, gymnast, dancer, football Ischial tuberosity > AIIS > ASIS > iliac crest, lesser troch, greater troch S/Sx: sudden pain +/- pop, poor ROM, local pain and TTP +/- muscle bulging away from the attachment Xrays needed to eval size/displacement Tx: PRICEMM, progressive rehab Ortho referral if displacement >2 cm Slipped Capital Femoral Epiphysis (SCFE) Slippage of femoral epiphysis laterally off femoral head Most prevalent ages 9-15, esp overweight Bilateral up to 50% S/Sx: insidious poorly localized hip/groin pain +/- radiation to knee, worse w/ activ May have limited IR Xrays usually diagnostic; MRI early if neg but dz suspected Tx: immed NWB, Ortho referral, surgery Kline’s Line: tangent to superior femoral neck on AP view Abnormal: Less or no transsection of physis Normal transsection of physis Legg-Calve-Perthes Dz Avascular necrosis of proximal femoral epiphysis Most prevalent ages 4-9, males 4:1 Develops slowly S/Sx: intermittent deep hip pain worse w/ activity, +/- radiating to groin, ant/med thigh, knee; limping, decreased ROM, and hip flexor tightness may be noted Xrays usually diagnostic: MRI or BS early if xray neg but AVN suspected Tx: Ortho referral; crutches, pain meds Acute Transient (“Toxic”) Synovitis inflammatory process of hip w/ chronic irritation and excess secretion of synovial fluid within the capsule; ? cause Most common dx in limping child <10, but it’s a Dx of exclusion; r/o septic arthritis, SCFE, stress fx, etc. Xrays normal; MRI helpful ruling out other causes Labs: normal CBC, CRP S/Sx: pain w/ walking, low-grade fever Tx: relative rest, analgesics Conclusion Know your anatomy Know why you’re doing an exam References Birrer R. and O’Connor F. Sports Medicine for the Primary Care Physician. Boca Raton: CRC Press, 2004. Greene W. Essentials of Musculoskeletal Care. Rosemont: American Academy of Orthopaedic Surgeons, 2001. Hoppenfeld S. Physical Examination of the Spine and Extremities. East Norwalk: Appleton-Century-Crofts, 1976;5974. Lillegard W. Evaluation of Knee Injuries. In W Lillegard (ed), Handbook of Sports Medicine. Boston: Butterworth-Heinemann, 1999: 233-249. Netter F. Atlas of Human Anatomy. West Caldwell: CIBAGeigy, 1989. Tandeter H. et al. Acute Knee Injuries: Use of Decision Rules for Selective Radiograph Ordering. American Family Physician. Dec 1999; 60: 2599-608. (For Radiograph Images)