Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
PEDIATRIC GI
EMERGENCIES
Kevin Levere
Jan 16, 2003
Objectives
• To appreciate differences from adults in
• GI bleeds
• Pancreatitis
• Liver disease
• To review common pediatric abdominal
emergencies
• IBD, toxic megacolon, metabolic disease, constipation,
colic, and jaundice are not discussed
Pediatric GI Bleeds
• Many etiologies similar to adult
• Frequency differs significantly
• Some uniquely pediatric causes
• Mortality lower than adult counterparts
• Fewer comorbidities
• Relatively greater physiological flexibility
• Division between upper and lower
• Ligament of Treitz
Case
• 4wo ex35wker girl, breast feeding. Spat up a
shot-glass worth of red blood.
• Apart from oral thrush, her exam is normal.
• Hx: Got Vit K. No meds. Growing. No BRBPR.
• FHx: No bleeding diatheses. Mom not on
meds, but has mastitis.
• Apt test turns yellow-brown
Case
• 2yo boy passing several fairly large maroon
coloured BMs, x12hrs. Painless. Normal BM Hx
until then.
• 37, 140, 90/70, 24, pale but playful. OB+. Hgb
60, rest of CBC normal.
• Which is best course of action?
•
•
•
•
A) cross-match, radionuclide scan, IV bolus, surgery
B) cross-match, IV bolus, scan, surgery
C) cross-match, IV bolus, surgery, scan
D) IV bolus, 0- transfusion, surgery, forget the scan
DIFFERENTIAL DIAGNOSIS OF GI BLEEDING *
Upper GI Bleed
Newborns
Infants
Children
Swallowed maternal blood
Epistaxis
Epistaxis
Hemorrhagic gastritis
Gastritis
Tonsillitis/sinusitis
Stress ulcer
Esophagitis
Gastritis
Idiopathic
Stress ulcer
Mallory-Weiss tear
Coagulopathy
Gastric/duodenal ulcer
Gastric/duodenal ulcer
Gastric outlet obstruction
Foreign bodies
Medications
Gastric volvulus
Gastric volvulus
Tumors
Pyloric stenosis
Esophageal varices
Hematologic disorders
Antral/pyloric webs
Esophageal varices
Munchausen by proxy
Lower GI Bleed
Anal fissure
Anal fissure
Anal fissure
Allergic proctocolitis
Infectious diarrhea
Infectious diarrhea
Infectious diarrhea
Allergic proctocolitis
Polyp
Hirschsprung’s disease
Meckel’s diverticulum
Hemorrhoids
Necrotizing enterocolitis
Intussusception
Inflammatory bowel disease
Volvulus
GI duplication
Henoch-Schonlein purpura
Stress ulcer
Peptic ulcer
Meckel’s diverticulum
Vascular malformation
Foreign body
Peptic ulcer
GI duplication
Hemolytic uremic syndrome
Vascular malformations
From Mezoff AG, Preud Homme DL. Contemp Pediatr 1994; 11:60-92.
* In order of frequency, most common in bold.
Pediatric GI Bleeds
• Hemorrhagic disease of the newborn
• Early (<1wk)
• Vitamin K deficiency
• Rare now administration of vitamin K shortly after birth
has become routine
• Maternal anticoagulant and intrapartum
antiepileptic drug use
• Late onset (2-6mos)
• Fat malabsorption
Pediatric GI Bleeds
• Ingestion of maternal blood
• Apt Downey test
• 1:1 stool with tap water, spin
• 5:1 supernatant with 1% NaOH
• After 2 mins
• Pink = fetal Hgb
• Yellow = maternal Hgb
Pediatric UGI Bleeds
• Upper GI Bleeds
• No good epidemiologic data outside PICU
• 6-25%, depending on prophylactic therapy
• 0.4% considered significant
• Commonest endoscopic findings
•
•
•
•
•
Gastritis
Esophagitis
Varices
Ulcers
Mallory-Weiss tears
Pediatric UGI Bleeds
• Ulcers and Gastritis
• Gastric acid production begins shortly after
birth
• Ulcers relatively rare
• Most are associated with NSAIDs and stress
• H. pylori infection
• Diffuse nodular gastritis commonest presentation
• Infection increases with age
• <5yo rare
• ~20-50% by 10yo (SES dependent)
• 40-80% adults (SES dependent)
Pediatric UGI Bleeds
• Esophagitis
• Severe GERD
• FB or chemical injury
• Infection
• Vascular anomalies
• Hemangiomas
• Hereditary telangiectasia
• Aortoenteric fistulas
• Congenital malformations
• Duplications, obstructions
• Predisposed to mechanical injury
Pediatric UGI Bleeds
• Management
• Similar to adults
• ABC’s, history and physical
• NG
• Same dilemma as in adults, but no pediatric data
• No longer use ice cold lavages
• Diagnostics
• CBC, PTT/INR, LFT’s, cross-match
• Limited roles for imaging – CXR, U/S, angiography
• Medications
• Acid-suppressive +/- visceral vasoconstrictive
• Limited but supportive data; dosing is the key difference
Pediatric UGI Bleeds
• Management
• Endoscopy
• Indications less standardized than in adults
• For severe or persistent/recurrent bleeding
• Diagnostic
• No data on risk of rebleeding based on findings
• Interventional as in adults
• Size the limiting factor for techniques
• Safety similar to adult data
• Complication rate 0.3% in retrospective study of 2026
Pediatric UGI Bleeds
• Management
• Surgery as back-up
• Failed endoscopic therapy
• Surgical lesion, e.g. Dieulafoy’s lesion
• Take home point
• Non-GI sources as common as GI sources in
“pediatric UGI bleeds”
Pediatric LGI Bleeds
• Lower GI Bleeds
• 0.3% of ED visits
• 50% <1yo
• Allergic colitis, fissures commonest
• >1yo
• Infectious GE, fissure, polyps commonest
• Ann Emerg Med, 1994
Pediatric LGI Bleeds
• Diagnosis
• Nature of bleeding helps localize origin
• N.B. hematochezia unreliable in infants, with their
faster GI transit times
• History and physical
• If doubt bleeding, or suspect false-pos guaiac
• Immunodiffusion of fecal Hgb
• Sensitivity and specificity ~70% each, as with guaiac
• Fecal alpha-1-AT measurement
• Sensitivity 88%, specificity 90%
• Also elevated in protein-losing enteropathy???
Pediatric LGI Bleeds
• Numerous laboratory and imaging options
•
•
•
•
Blood
Stool
Urine
Plain films, nuclear scans, endoscopy
• Commonly used in painless bleeding
• Non-barium contrast studies, U/S, CT, MRI,
angiography
• Dependent on suspected etiology
Pediatric LGI Bleeds
• Management
• Similar to adults
• ABC’s, history and physical
• NG
• Aspirate can help identify if blood from UGI source
• Diagnostics
• CBC, PTT/INR, LFT’s, cross-match, etc
• Medications
• Visceral vasoconstrictive
• Supportive data for role in LGI bleeds
• Treat underlying cause
Pediatric LGI Bleeds
• Neonatal
• NEC
• Risk factors
•
•
•
•
•
•
•
Prematurity (87% of cases)
Hypoxia
Sepsis
Acidosis
Early enteral feeds
Umbilical vascular catheter
PDA
• Epidemics support infectious component
Pediatric LGI Bleeds
• Neonatal
• NEC
• Onset
• Typically <4wks of age; can be late as 3mos
• Manifestation
•
•
•
•
Abdominal distention, gastric retention
Poor feeding, V/D, lethargy, apnea
Gross blood in stools in only 25%
Severe cases lead to SIRS
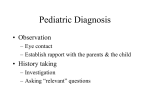
Pediatric LGI Bleeds
• Pneumatosis
intestinalis in 50-75%
at diagnosis
• Portal venous gas in
severe disease
Pediatric LGI Bleeds
• Neonatal
• NEC
• Complications
• Mortality up to 5%
• Strictures in 10%
• Treatment
• Supportive
• Antibiotics, gut rest
• Surgical back-up
Pediatric LGI Bleeds
• Neonatal
• Hirschsprung disease
• Congenital aganglionic megacolon
• Delayed (>48hr) passage of meconiom
• History of (often progressive) constipation
• 25% have blood in stool
• Diagnosis
• Contrast enema – proximal dilation = normal bowel
• Rectal manometry
• Biopsy with absent ganglion cells
• Treatment is surgical resection
Pediatric LGI Bleeds
• Infants
• “Allergic” colitis
• Intolerance to cow’s milk protein
•
•
•
•
0.2-7.5% prevalence
Soy protein intolerance in 14-25% of these
Typically not IgE mediated
Resolves in most by 2yo
• Treatment is dietary restriction
• Volvulus
• Intussusception
Pediatric LGI Bleeds
• Children
•
•
•
•
Infectious enterocolitis
HUS, HSP, pseudomembranous colitis
IBD
Vascular malformations
• Hemangiomas, telangiectias, varices, hemorrhoids
• Polyps
• Other tumors, e.g. colon cancer, are rare
• Trauma
• FB, NAT
Pediatric LGI Bleeds
• Meckel’s diverticulum
• Vitellointestinal duct remnant
• 50% have gastric mucosa
• Most important source of small bowel bleeding
• Gastric mucosal ulceration vs intussusception
• Rule of 2’s
•
•
•
•
2% of population
2:1 male:female
2 feet from IC valve
Under 2yo commonest
• Diagnosed by radionuclide scan
• Treatment is surgical resection
Pediatric LGI Bleeds
• Take home point
• Think of NEC and Meckel’s
• Both relatively common
• Both potentially serious
Case
• 13yo girl with 3days fever, despite Tylenol used
round the clock. Also c/o N/V, anorexia,
moderate epigastric pain. Today a bit jaundiced.
Denies EtOH or other drug use. Her boyfriend
has Mono.
• 38.7, 100, 120/85, 22. Abdo tender, a bit
distended, else exam normal.
Pancreatitis
• Differential
•
•
•
•
•
Gastroenteritis
Ulcer
Hepatitis
Pneumonia
Biliary tract obstruction
Pancreatitis
• Much less common than in adults
• Pathogenesis
• Cell injury (toxin or otherwise) sets off
pancreatic autodigestion and inflammatory
response
Pancreatitis
• Acute
• Interstitial edema
• Usually resolves within 2-7 days – mortality 5%
• Complications – rare
• Pseudocyst – slow to mature and resolve (weeks)
• Phlegmon, necrosis +/- hemorrhage
• SIRS – 50-80%+ mortality
• Chronic/recurring
• Endocrine and exocrine insufficiencies
• Calcification
Pancreatitis
• Etiology – the key difference in pediatrics
• Trauma
• Blunt injury – commonest cause; think of NAT
• Infection
• Viral (not just mumps), et al
• Multisystem disease
• CF, collagen vascular disease, vasculitits, metabolic
• Obstructive
• Congenital anomalies, biliary microlithiasis
• Drugs and Toxins
• EtOH, acetaminophen
• Hereditary – autosomal dominant
• Idiopathic (25%)
Pancreatitis
• Clinical Picture
• Abdominal pain
• Steady, epigastric, with tenderness, distention
• Persistent vomiting
• Proportional to abdominal pain
• Fever
• Associations in complicated picture
• Mass, e.g. in 50% of cases with pseudocyst
• Asictes, pleural effusions, hypocalcemia, hyperglycemia,
jaundice
• Grey Turner (flank) and Cullen (periumbilical) signs
• MSOF and shock
Pancreatitis
• Diagnosis
• Serum lipase
• sensitivity 86% to 99%; specificity of 50% to 99%
• Elevated 1-2 weeks longer than amylase
• Serum amylase
• sensitivity 75% to 92%; specificity 20% to 60%
• General lab evaluation
• Urinary trypsin activation peptide (TAP)
• Investigational prognosticator
• Ranson and APACHE-II criteria
• Not reliable in pediatrics
Pancreatitis
• Diagnosis
• Diagnostic imaging – 20% normal at first
• Plain films
• Pleural effusions, “sentinel loop”, “cut-off sign”
• U/S
• Biliary tract evaluation, or follow-up of cysts/abcesses
• CT
• Usually only if poor U/S visualization
• ERCP/MRCP
• Considered if recurrent/undiagnosed problems
• For suspected stones
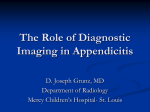
Pancreatitis
• Acute pancreatitis
• Pseudocyst 5 months
after acute episode
Pancreatitis
• Management
• “Pancreatic rest”
• NPO +/- NG
• Pain control
• Meperidine – opioid causing least enterobiliary pressure by
contraction of Sphincter of Oddi
• Fluid and electrolyte homeostasis
• Surgical and antibiotic interventions rare
• Abcess, infected pseudocyst, necrosis, hemorrhage
• Address underlying cause if able
Pancreatitis
• Take home point
• Trauma, including non-accidental, is the
commonest cause
Liver Failure
• Fulminant hepatic failure
• Acutely impaired hepatocyte function with
• Encephalopathy within 8 weeks of initial
symptoms, with a previously healthy liver, or
• Encephalopathy within 2 weeks of jaundice, even if
previously underlying liver dysfunction
Liver Failure
• Cirrhosis
• End-stage of acute or chronic disease
• Fibrosis following injury from hepatitis, necrosis, or
biliary obstruction
• Restricts blood flow, creating portal hypertension,
and ischemia further impairing heptocyte function
• Biliary atresia
• Commonest cause of liver failure in pediatrics
Fulminant Hepatic Failure
• Etiology
• Viral
• HBV likely the commonest of these
• TORCH
• Toxins
• Acetaminophen the most common toxin
• Amanita phalloides, EtOH, PHT, VPA…
• Vascular
• Veno-occlusive disease, ischemia, thrombosis
Fulminant Hepatic Failure
• Etiology
• Metabolic
• Wilson’s, neonatal iron storage disease,
tyrosinemia, galactosemia, fatty acid oxidation
defects, mitochondrial disease
• Reye’s syndrome
• Others
• Malignancy, autoimmune, idiopathic (20-40%)
Fulminant Hepatic Failure
• Clinical Picture
•
•
•
•
•
•
•
Jaundice
Fetor hepaticus
Fever
Anorexia
Vomiting
Abdominal pain
Encephalopathy
• Grades I-IV = mild confusion to coma
Fulminant Hepatic Failure
• Note about ALT
• Most specific for hepatocellular toxicity,
BUT…
• Falls as exhaust hepatocyte supply
• Markers of function
• Bilirubin, albumin, INR, glucose, NH3
Fulminant Hepatic Failure
• Complications
• Cerebral edema
• Renal failure
• Coagulopathy
• GIT commonest site of bleeding
•
•
•
•
Hypoglycemia
Metabolic instability
Infection
MSOF
Fulminant Hepatic Failure
• Treatment in ED
• Eliminate or treat cause if able
• N-acetylcysteine, charcoal
• Supportive therapy
• ABC’s, then
• Increased ICP
• Mannitol or hyperventilation; no Dexamethasone
• Bleeding
• FFP; FVIIa being studied
• H2 blocker > sucralfate; PPI role being studied
Fulminant Hepatic Failure
• Treatment thereafter
• Ongoing supportive care
• Corticosteroids shown to worsen outcome
• For encephalopathy
•
•
•
•
Lactulose
Neomycin
Low protein diet
Plasmapheresis
• Specific therapies
• Antivirals, TIPS, thrombolysis, transplant
Fulminant Hepatic Failure
• Prognosis
• 50% experience serious infection
• Mortality with medical care ~70%
• Worse prognosis if <10yo or >40yo
• Transplant survival 50-80%
• Spontaneous recovery
• More likely with low grade encephalopathy
• Viral and acetaminophen 50-60%
• Wilson’s and some idiosyncratic reactions 10-20%
Liver Failure
• Take home point
• Infants with fulminant hepatic failure typically
have congenital problems, i.e. underlying liver
disease
• They don’t strictly fit the definition for fulminance
Case
• 5yo with 1day of vomiting and occasional
diarrhea. Severe abdo pain on and off every 15
mins or so. No sick contacts.
• 37.9, 120, 110/75, 22. Abdo diffusely tender, no
peritonitis, no mass. CBC normal, OB+.
Intussusception
• Differential Diagnosis
•
•
•
•
GE
Formula intolerance
Volvulus
Incarcerated hernia
• inguinal>internal
Intussusception
• Definition
• Invagination of proximal intussusceptum into
distal intussuscipiens
• Ileocolic>cecocolic>ileoileal
• Epidemiology
•
•
•
•
1-4/1,000 live births
50% by 1yr,80% by 2yrs, 90% by 5yrs
Peak incidence 10mos (2mos-2yrs)
2-4:1 male:female
Intussusception
• Etiology
• 90-95% idiopathic in <2yo’s
• Peyer patches’ hypothetical role
• Pathologic lead points commoner in >5yo’s
• Meckel’s diverticulum commonest
• Polyps, HSP lesions, lymphomas, appendix, HUS,
parasite, hemangiomas, metastases, CF, fecolith
• Entrapped mesentery, bowel edema cause
ischemia
Intussusception
• Clinical Picture
• Classic triad seen in <20%
• 13% have less than or equal to 1 of these features
• Intermittent abdominal pain (50-90%)
• Vomiting (60-80%)
• Blood and mucous in stools (20-60%)
• Currant jelly stools are a late sign (20%)
Intussusception
• Clinical Picture
• Nonspecifics
• Fever
• Poor feeding
• Lethargy
• Physical Exam
• “Dance’s sign” = sausage in RLQ (up to 70%)
• Abdominal mass in 25-85%
Intussusception
• Diagnosis
• Plain films
• Normal in <30%; suspect mass in 70%; obstruction
• Barium or H2O-soluble enema
• Gold standard for diagnosis and therapy
• Misses ileoileal cases, e.g. Meckel’s
• U/S
• High accuracy
• Adjunct to enemas, to monitor therapeutic effect
Intussusception
• Plain film
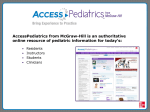
Intussusception
• Coil-spring
appearance
• Target on U/S
Intussusception
• Therapy
• Barium or H2O-soluble enema
• Successful reduction in 80% <48hrs, 50% >48hrs
• Air-contrast enema
• Studies suggest at least as effective as barium
• Bowel perforation in 0.1-0.2% vs 0.5-2.5% with Ba
• Surgical
• Reduction vs resection
• Dexamethasone
• Hypothesis that it might reduce recurrence
Intussusception
• Initial misdiagnosis in up to 60%
• GE commonest
• Consider in differential of lethargy
• Spontaneous resolution rare
• Mortality increases after 24-48hrs
• Recurrence rate 5-8%
• Higher if pathologic lead point
• Less after surgery
Intussusception
• Take home points
• Be suspicious of this diagnosis
• Add it to your differential for lethargy
Volvulus
• Definition
• Closed loop obstruction from twist in GIT from
a predisposing embryonic malrotation
• Epidemiology
• Malrotation in 1/500 births
• 70% experience volvulus
• 2/3 of volvulus occurs by 1mo, 75% by 12mo
Volvulus
• Clinical Picture
• Bilious emesis (80-100%)
• Abdominal pain
• Peritonitis, shock as ischemia progresses
• Necrosis can occur within 2hrs
• Feeding intolerance
• Normal abdominal examination in 50%
• Since obstruction is usually high and proximal
Volvulus
• Differential Diagnosis
• Small bowel obstruction (most are duodenal)
•
•
•
•
Web
Stenosis
Atresia
Hernia
• Large bowel obstruction
• Adynamic ileus
Volvulus
• Diagnosis
• Plain films
• Variable: normal, SBO, LBO
• UGI
• Taper/beak of contrast; Ligament of Trietz
abnormally located
• Malrotation can be suspected by U/S
• Abnormal position of superior mesenteric vessels
• Malrotation work-up includes contrast enema
• Cecum most common element of malrotation
Volvulus
• Management
• Volvulus is a surgical emergency
• Take home point
• Bilious emesis is volvulus until proven
otherwise
Appendicitis
• Definition
• Appendicitis!
• Pathophysiology
• Luminal obstruction vs mucosal ulceration
leads to inflammation or infection, edema and
ischemia, then perforation, and subsequent
peritonitis or abcess formation
Appendicitis
• Epidemiology
• Incidence: 2/10,000 <4yo, 25/10,000 teens
• 1/10th incidence where high fiber diets
•
•
•
•
•
Seasonal variability
Family history has RR of 3.5-10
Lifetime risk: 9% males, 7% females
1-8% of ED Diagnoses of abdominal pain
Perforation: ~90% <3yo, <15% teens
Appendicitis
• Pathophysiology Encore
• Appendix’s function - ? immunologic
• Funnel shaped tube in infants
• Less likely to obstruct
• Maximal lymphoid hyperplasia in teens
• Corresponds to peak incidence
• More mobile than in adult population
• Hence more confounding clinical features
Appendicitis
• Clinical Picture – age dependent
• Classic progression
• Periumbilical pain – N/V – RLQ pain
• Occurs in 50% of adult cases, less in pediatric
• Hence initial misdiagnosis 28-57%
• Neonates (~80% mortality)
• Features are nonspecific
•
•
•
•
Lethargy, irritability (20%)
Vomiting (60%)
Abdominal distention (60-90%)
Mass (20-40%), abdominal cellulitis, dyspnea, shock
Appendicitis
• Clinical Picture
• Infants – misdiagnosis 70-100%
• Commonest features
•
•
•
•
Vomiting (85-90%)
Pain and diffuse tenderness (35-92%)
Fever (50%)
Diarrhea (18-46%)
• Right hip complaints (3-23%)
Appendicitis
• Clinical Picture
• Pre-schoolers – misdiagnosis 19-57%
• Vomiting often noted before pain
• RLQ pain and tenderness become more prominent
than diffuse pain
• Rebound and guarding evident
Appendicitis
• Clinical Picture
• School-aged kids – misdiagnosis 12-28%
• Clearer communication of features
• Non-classic features
• Vomiting prior to pain (18%)
• Dysuria (up to 20%)
• Constipation or diarrhea (~20% each)
• Adolescents – misdiagnosis <15%
• Challenge in female population
• Pelvic pathology
Appendicitis
• Clinical Picture
• Rebound most sensitive (83%) and (with percussion)
most specific (82%) for peritonitis (adult data)
• No pediatric data on psoas, obturator, cough, and
Rovsing’s signs, or cat’s-eye symptoms
• Rectal exam adds little outside of infant population
(except legal fodder in the USA)
• Alvarado’s MANTRELS scoring system not accurate
in pediatrics
Appendicitis
• Differential Diagnosis
•
•
•
•
•
•
•
•
•
GE
Mesenteric adenitis
Tubo-overian pathology
UTI
Intussusception
Meckel’s diverticulitis
Testicular pathology
RLL pneumonia
Sepsis
Appendicitis
• Diagnostic Studies – limited role, nothing 100%
• WBC
• Non-specific, non-sensitive – might alter suspiscions >48hrs
• Neutrophilia
• More sensitive at <24hrs of symptoms than WBC
• CRP
• Studies suggest more sensitive than WBC if perforation
• Beta-HCG
• The only “mandatory” test, in teen girls
• U/A
• 7-25% abnormal due to appendicitis
Appendicitis
• Radiology
• Plain films
• Fecolith in 13-20% (1-2% without appendicitis)
• Role if suspect free air, obstruction, or mass
• WBC scans
• Variable results, therefore not recommended
• U/S
• Sensitivity 80-92%, specificity 86-98%
• Don’t visualize appendix in 10% with appendicitis
• CT (+/- contrast)
• Sensitivity 87-100%, specificity 83-97%
• Sometimes used to follow-up negative U/S
Appendicitis
• Management
• Controversy over use of “prophylactic” antibiotics in
uncomplicated appendicitis
• Often decision deferred to surgeon
• Fluid resuscitation and broad-spectrum antibiotics if
suspect perforation
• Observation in equivocal cases
• Rare cases sound like recurrent appendicitis
• Think IBD!
Appendicitis
• Take home points
• Young children and adolescent girls are
hardest to diagnose
• In the CT vs U/S debate
• U/S is often better in thin patients
• CT is often better in fat patients
• Utilization is centre and resource dependent
Incarcerated Inguinal Hernia
• Hernias
• Indirect in >99% of pediatric cases
• Epidemiology
• 1-2 inguinal hernias/100 live births
• Up to 30% in prems
• Most right-sided; 10% bilateral (more in girls!)
• 10% complicated by incarceration
• Commonest cause of obstruction in infants
• 70% of these by 1yo
• 4-6:1 male:female
Incarcerated Inguinal Hernia
• Hernia vs Hydrocele
Incarcerated Inguinal Hernia
• Clinical picture
•
•
•
•
Bulge in groin
Progresses to off-colour, firm, tender mass
Symptoms and signs of intestinal obstruction
Unlike hydrocele, can feel neck of mass at
distal inguinal ring
• Transillumination suggests hydrocele
Incarcerated Inguinal Hernia
• Differential Diagnosis
• Hydrocele
• Undescended or retractile testes
• Lymphadenopathy
• Management
• Manual reduction
• 95% success, less if ovary entrapped
• Surgery for all hernias
• Emergent if not reducible
Case
• 6 wk old boy with 2/52 forceful non-bilious
vomiting after feeds. Responsive, feeds hungrily.
• 36.5, 150, 28, 90/50. CRT>2secs, AF
depressed. Abdo soft, non-tender.Skin turgor
diminished. Na 125, K 3.8, Cl 85, CO2 30.
• Which of these is correct?
• A) Congenital adrenal hyperplasia
• B) Hypertrophic pyloric stenosis
• C) Malrotation with volvulus
• D) Milk allergy
Pyloric Stenosis
• Differential Diagnosis
•
•
•
•
•
•
GERD
Milk allergy
Infection (e.g. GE, sepsis)
Hydrocephalus
Metabolic disorders
Surgical causes
• Malrotation, webs, duplications, atresias, annular
pancreas
Pyloric Stenosis
• Definition
• Idiopathic hypertrophy of pyloric muscle
• Epidemiology
• 1-4/1,000 live births
• 2-5:1 male:female
• Family history; genetic syndromes
• Etiology
• Poor innervation of pyloric musculature
• Presumed molecular cause (e.g. NO, GrwthF)
Pyloric Stenosis
• Clinical Picture
• Presents 1-10wks
• Peak incidence 3-5wks
• Progressive nonbilious projectile emesis post
feeds
• Earlier onset but slower progression in prems
• Hungry until too dehydrated
Pyloric Stenosis
• Physical Examination
• Up to 90% specific, but <50% sensitive
• RUQ “Olive”
• 60-80% found “by an experienced examiner”
• LUQ peristalsis
• Saw it at last!
Pyloric Stenosis
• Diagnosis
• Hypochloremic metabolic alkalosis
• +/- hypokalemia
• +/- hyponatremia
• +/- paradoxical aciduria
• Imaging
• U/S vs UGI
• Both >90% sensitive
Pyloric Stenosis
• Management
• Correct hydration and electrolyte disorders
• Focus on chloride replacement else alkalosis
resistant to therapy
• Severe alkalosis and hyponatremia need slow
correction to decrease risk of pontine myelinolysis
Pyloric Stenosis
• Management
• Pyloromyotomy commonest choice
• Natural history
• spontaneous resolution over weeks to months
• Controversial option – long-term TPN
• Atropine has reportedly hastened this resolution
• No good trials to date for this option
• No long-term differences in gastric emptying
Pyloric Stenosis
• Take home point
• This is a medical, not a surgical emergency
DEHYDRATION IN
PEDIATRICS
Kevin Levere
Jan 16, 2003
Definition
• Loss of H2O and salt from ECF
• Isonatremic – 70-80%
• Hyponatremic – 10-20%
• Hypernatremic – 10-20%
Question
• Which of the following is associated with greater
fluid loss per KG for a given severity of clinical
manifestations of dehydration?
• A) Fever
• B) Hypernatremia
• C) Male gender
• D) Obesity
• E) Older age
Etiology
• Infectious gastroenteritis
• Commonest by far (>1 episode/yr/pediatric
patient)
• Compounded by malnutrition
• Pyloric stenosis
• DKA or DI
• Starvation
Pathophysiology
• Lean Body Mass (LBM) is 65-80% H2O
• Infants
• 25% ECF, 45% ICF
• Children by 5yo (equivalent to adults)
• 20% ECF, 50% ICF
• Plasma is within ECF
• 6% of LBM at all ages
• Total Body Weight is ~10% fat in older
children and adults
• So Total Body Water is ~60% of Total Body Mass
Pathophysiology
• Renal and hormonal homeostasis
• Preserve H2O, regulate Na
• Losses
• Insensible, GI, renal
• Intake
• Deficient
• Hypoosmolar vs hyperosmolar
Clinical Picture
• Isonatremic
• Isoosmolar state, no fluid compartment gradient
• ICF preserved
• Hyponatremic
• Further H2O loss as shifts from ECF into ICF
• Exacerbates circulatory depletion, enhancing signs
• Hypernatremic
• ECF preserved by shifts from ICF
• Attenuates circulatory signs; doughy skin; lethargy
Clinical Picture
• Signs arise at 3% - Lancet, 1989
• Clinical overestimation is common
• Clinical Physician estimates ~70%
sensitive
• Pediatr Emerg Care, 1997
• Tachycardia presents early
• Not specific, and surprisingly not sensitive
• Decreased U/O occurs by 5%
• Therefore poor predictor of severity
Clinical Findings of Dehydration (Adapted from WHO)
Signs and Symptoms
Degree of Impairment
None or Mild
Moderate
Severe
General Condition
Infants
Thirsty; alert; restless
Lethargic or drowsy
Limp; cold, cyanotic
extremities; may be
comatose
Older Children
Thirsty; alert; restless
Alert; postural dizziness
Apprehensive; cold,
cyanotic extremities;
muscle cramps
Quality of Radial
Pulse
Normal
Thready or weak
Feeble or impalpable
Quality of
Respiration
Normal
Deep
Deep and rapid
Skin Elasticity
Pinch retracts
immediately
Pinch retracts slowly
Pinch retracts very
slowly (>2 sec)
Eyes
Normal
Sunken
Very sunken
Tears
Present
Absent
Absent
Mucous Membranes
Moist
Dry
Very dry
Urine Output (by
report of parent)
Normal
Reduced
None passed in many
hours
Clinical Picture
• Validity and Reliability of Clinical Signs
• Pediatrics, 1997
• Individual findings lack sensitivity
• Included capillary refill time and tachycardia
• For dehydration of 5% or more
• 3 or more findings 87% sensitive and 82% specific
• For dehydration of 10% or more
• 7 or more findings 82% sensitive and 90% specific
Clinical Picture
• Validity and Reliability of Clinical Signs
• Pediatrics, 1997
• Factors independently associated with
dehydration (in logistic regression)
•
•
•
•
Capillary refill >2 sec
Dry mucous membranes
Absent tears
Ill appearance
• For dehydration of 5% or more
• 2 of 4 findings 79% sensitive and 87% specific
lablablab
• Common lab tests
• Recommended in moderate to severe cases
• Not sensitive or specific for degree of dehydration
• Na
• Reflects relative losses of H2O and salts
• K
• Low if lost in diarrhea or if alkalotic (vomiting)
• High if renal compromise or acidosis
• HCO3
• Lost in renal compromise or stool losses
• Might replace if renal compromise and acidosis
More Labs
• Cl
• Alkalosis resistant to therapy if not replaced
• Urea
• Estimates degree of renal compromise
• Ca
• Reduced if phosphate retention or hypernatremia
• Rarely significant
• U/A
• Specific gravity
Fluid Therapy
• “Coconut Water!”
Fluid Therapy
• 150 years of History
• Parenteral concoctions assayed with varying success
• Early theories were that ICF was dehydrated because of
excess K in diarrhea – 1915
• Principle of cellular homeostatic limits led to maintenance
and deficit therapy, IV therapy as mainstay – NEJM, 1953
• Greater success after realized ECF dehydration was the
greater contributor, with potassium restored during
maintenance – Pediatrics, 1956
• Affect of net Na and glucose relationship on reabsorption
appreciated, oral rehydration therapy (ORT) success realized
– NEJM, 1968
• Free water and concentrated ORT solutions found to have
increased mortality, hence reduced osmolar questions
Oral Rehydration Therapy (ORT)
Osmoles
mOsm/L
Glucose
mmol/L
Na
mEq/L
Cl
mEq/L
HCO3
mEq/L
K
mEq/L
WHO
formulation
330
110
90
80
30
20
Pedialyte
270
140
45
35
30
20
AJ
(CHOs)
730
690
5
x
x
32
Sports drink
(CHOs)
330
255
20
x
3
3
D5W /
0.45% saline
454
77
77
0
0
300
Fluid Therapy
• Rice-based oral solution with WHO’s
electrolyte balance:
• More effective than the WHO ORS in reducing
stool output in people with cholera. This effect
was not apparent in infants and children with
non-cholera diarrhea
• Cochrane Database Syst Rev, 2000
• Starch and small proteins as Na cotransport,
with less osmolar effect on diarrhea
Fluid Therapy
• Reduced osmolarity solutions
• ~270mOsm/L, Na ~60-75mEq/L
•
•
•
•
33% fewer IV infusions
Decreased stool losses
Less vomiting
No additional risk of hyponatremia
• Cochrane Database Syst Rev, 2001
• Only significant incidence of hyponatremia found in
adults with cholera, but none were symptomatic
• CHOICE Study Group, 1999
Fluid Therapy
• For severe dehydration (~10% or
100ml/kg)
• Rapid intravenous ECF restoration
•
•
•
•
•
Over 2-6hrs
Improves renal perfusion and function
Reduces vomiting
Earlier resumption of oral intake, including food
Food and milk might shorten duration of diarrhea
despite transient lactase deficiency
• Avoid fatty food and simple sugars
Fluid Therapy
• For severe dehydration
• IV restoration followed by ORT to replace K,
restore ICF status
• For maintenance and ongoing losses
• Deficit calculations in isonatremic situations
not found to improve care
Fluid Therapy
• For hypernatremic dehydration
• Restore circulation (treat shock)
• Deliver maintenance and deficit over 48hrs to
avoid cerebral sequelae
• Hyperglycemia often accompanies
hypernatremia
• Slower restoration increases risk of
hypocalcemia, especially in young infants
Fluid Therapy
• For mild to moderate dehydration (5-9%)
• ORT is 90-95% effective
• Oral fluid challenge only if moderate (i.e.
borderline for IV therapy)
Fluid Therapy
• NG vs IV
• Pediatrics, 2002
• 93 patients prospectively enrolled
• Moderate dehydration, failed oral fluid challenge
• Randomized to rapid NG vs IV hydration
• 50ml/kg over 3hrs of Pedialyte vs NS
• Both found to be safe and efficacious
• Significantly more emesis in NG group
• Significantly less cost
• Improved acidosis in NG vs worsened in IV
• Not clinically significant; no other lab variance
Fluid Therapy
• NG vs IV vs ORT
• Failure meant getting admitted
• 1 of the 47 NG arm failed (~2%)
• 2 of the 46 IV arm failed (~5%)
• ORT is 90-95% successful, and cheapest
• Still the first line therapy in moderate dehydration
• Oral fluid challenge poorly defined
• Only useful if borderline for IV/NG intervention
Medications
• Antidiarrheals
• None recommended in younger children
• AAP Guidelines, 1996
• Loperamide and other opiate derivatives
• Limited efficacy vs high rate of side effects
• Anticholinergics
• No clear efficacy, high rate of side effects
• Bismuth compounds
• Limited benefit vs lack of data on rates of side effects
• Adsorbents and lactobacillus
• No clear benefit, though little concern of toxicity
Medications
• Antiemetics
• Concensus opinion – they aren’t needed
• Little efficacy vs side effects
• CHMC Guidelines, 1997
• Ondansetron effective in reducing emesis
from GE, increasing success of ORT
• Ann Emerg Med, 2002
Medications
• Zinc
• Role in the malnourished
• Reduced duration and severity of diarrhea
• Independent of Vitamin A supplementation
• Pediatrics, 2002
• Regular Zn supplementation reduced frequency of
diarrheal illnesses (and pneumonias)
• J Pediatrics, 2002
Ad(sub)mission
• Significant dehydration and…
• Persistent and/or prolonged ongoing losses
• Care-givers far from help, or unable to help
• Ill despite fluids – consider other
diagnoses
• i.e. back to the beginning
Thank you
Liver Disease
• Chronic manifestations
•
•
•
•
•
•
•
•
•
•
•
Hepatomegaly
Jaundice
Pruritis
Spider hemangiomas
Palmar erythema
Ascites
Portal hypertension
Xanthomas
Encephalopathy
Renal dysfunction
Endocrinopathies (rarer than in adults)
Liver Disease
• Hepatomegaly
• Inflammation
• Infections, toxins, autoimmune disease
• Storage
• Glycogen, lipids, Wilson’s, iron
• Infiltration
• Primary and secondary neoplasia
• Congestion
• CHF, veno-occlusive disease, post-hepatic
obstruction
Liver disease
• Jaundice (aka icterus)
• In neonates at 80-100micromol/L
• Occurs at lower levels in children and adults
• Unconjugated bilirubin
• Lipid soluble; unbound crosses BBB
• Conjugated bilirubin
• Unbound is renally excreted
• Increased if >20% total bilirubin
Approach to Neonatal Jaundice
Unconjugated Hyperbilirubinemia
• Hemolytic disease
• Hereditary or acquired
• Sepsis, UTI
• Decreased hepatic conjugation
• Decrease hepatic intake
• Breast milk, hypothyroidism
• Decreased hepatocellular function
• Hepatitis
• Physiologic, Crigler-Najjar, Gilbert
• Enterohepatic recirculation
Neonatal Cholestasis
• Infectious
• Sepsis, hepatitis, TORCH
• Toxin
• TPN, sepsis, drugs
• Metabolic
• Galactosemia, tyrosinemia, alpha-1 AT defiency, CF
• Intrahepatic diseases
• Alagille, bile duct paucity, congenital fibrosis
• Extrahepatic biliary diseases
Extrahepatic biliary diseases
• Biliary atresia
• Commonest cause of liver failure in pediatrics
• Sclerosing cholangitis
• Association with IBD
•
•
•
•
•
•
Bile duct stenosis
Choledochal-pancreaticoductal junction anomaly
Spontaneous perforation of the bile duct
Choledochal cyst
Mass (neoplasia, stone)
Bile/mucous plug ("inspissated bile")
Liver Disease
• Evaluation
• ALT most specific for hepatocellular toxicity
• AST might have role in evaluation of EtOH
etiology, not a typical pediatric concern
• 5’ nucleotidase and GGT sensitive markers of
biliary obstruction or inflammation
• Alk phosphatase not so specific
• Bilirubin, albumin, INR, glucose, NH3
• Markers of function
Liver Disease
• Evaluation
• Metabolic survey
•
•
•
•
•
•
Electrolytes, Ca, Mg, PO4
Renal function, U/A (ketones)
Glucose, U reducing substances
NH3, lactate, urate
Blood gas
Serum AA’s, urine AA’s and OA’s
Liver Disease
• Evaluation
• Imaging
• U/S, CT, MRI, ERCP
• Masses, gall bladder, biliary tree
• Nuclear med studies now very rarely used
• Liver biopsy