Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Hospital-acquired infection wikipedia , lookup
Hepatitis B wikipedia , lookup
Henipavirus wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Meningococcal disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
West Nile fever wikipedia , lookup
Oesophagostomum wikipedia , lookup
Yellow fever wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Anthrax vaccine adsorbed wikipedia , lookup
Onchocerciasis wikipedia , lookup
Brucellosis wikipedia , lookup
1793 Philadelphia yellow fever epidemic wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Typhoid fever wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Biological warfare wikipedia , lookup
History of smallpox wikipedia , lookup
Rocky Mountain spotted fever wikipedia , lookup
Steven Hatfill wikipedia , lookup
Yellow fever in Buenos Aires wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Orthohantavirus wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Leptospirosis wikipedia , lookup
Bioterrorism wikipedia , lookup
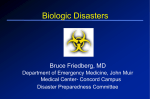
BIOTERRORISM UPDATE FOR EMS ANTONIO NAPOLITANO MD ATTENDING BRIDGEPORT HOSPITAL JHPC MEDICAL DIRECTOR OUTLINE • • • • • Overview History Agents most likely to succeed What to look out for What to do WHAT ARE BIOLOGICAL WEAPONS? • Microorganisms or biologic toxins used to produce death and disease. • Components of BW’s – – – – Payload Munition Delivery system Dispersal mechanism: line source vs. point source WHAT MAKES A BIOLOGICAL WEAPON DESIRABLE TO A BIOTERRORIST???? • • • • • • • Stable Deliverable as an aerosol Respiratory transmission Particle diameter of 1-5 microns Highly infectious Deadly No effective vaccine DELIVERY METHODS • Missile warheads • Aerosol generators – Airplane/boat – Fixed device • Food/water contamination • Percutaneously WHAT TO LOOK OUT FOR ? • Suspect a biological weapons attack if these signs of unusual disease clustering is present: – Large epidemic with unprecedented numbers of ill and dying – Common exposure site, common complaints in a large number of people – Unusual diseases for a particular region – Multiple simultaneous outbreaks – Reports of sick or dying animals/plants – Single case of disease by uncommon agent ie smallpox, VHF or inhalation anthrax WHAT TO LOOK OUT FOR ? • Disease associations to know – Widened mediastinum = inhalation anthrax – Hemorrhagic meningitis = inhalation anthrax – Vesicular/pustular rash on face/hands with all lesions at the same stage of development = smallpox – Symmetrical bulbar palsies and descending paralysis = botulism toxin – Pneumonia and hemoptysis = pneumonic plague CATEGORIES OF BW’s • Category A are highest priority agents – – – – – – Anthrax Botulism Plague Smallpox Tularemia Viral hemorrhagic fever CATEGORY B • Second highest priority agents – – – – – – Q fever Brucellosis Glanders Ricin Toxin from Ricinus communis Epsilon Toxin of Clostridium perfringens Staphylococcus Enterotoxin B CATEGORY C • Third highest priority agents – – – – – – Nipah virus Hantaviruses Tickborne Hemorrhagic Fever Viruses Tickborne Encephalitis Viruses Yellow Fever Multidrug-resistant Tuberculosis History of Biological Warfare • • • • Poisoning of wells by Assyrians in 6th century B.C. 1346 – Battle of Caffa. Smallpox-infested blankets given to Native Americans Japanese biowarfare experiments in Manchuria during WWII. Unit 731. • “Yellow rain” in Laos, Kampuchea in 1970’s. • Iraqi stockpiles found in Gulf War. • Aum Shimbun released anthrax spores along with sarin into Tokyo subway system in 1995. ANTHRAX • First described 3,500 years ago. The first vaccine ever invented and milk Pasteurization were invented to combat this bug. • Cutaneous, GI, and Pulmonary forms. • Engineered in the Soviet Union to be resistant to Doxycycline and Penicillin. • A disease of herbivores. Endemic to Balkans, Turkey, W. Africa, Spain, C Asia. INCUBATIO N • Spores break down at infection site, and the organism is picked up by macrophages and transported to lymph nodes where they cause massive, often hemorrhagic, lympadenopathy.. • Organisms elaborate toxins as they multiply. • Incubation usually 1-6 days but can be seen as far as 60 days. • 8000-50,000 spores necessary to cause disease ANTHRAX PATHOPHYSIOLOGY CUTANEOUS ANTHRAX • Pruritic red papule that necroses after three or 4 days and becomes a black eschar which sloughs off after 2-3 weeks. • 5-25% of cases become systemic or fatal. Excising the eschar can cause dissemination. • Mortality untreated cases 20%. Treated<1%. GASTROINTESTINAL ANTHRAX • Very rare, need to ingest spores in contaminated meat or large numbers of spores in water. • Presentation depends on area of GI tract affected • Fulminant peritonitis, mesenteric lymphadenitis and septicemia. • Mortality25-60% all comers. PULMONARY ANTHRAX • Very rare but VERY LETHAL • Early on easy to confuse with a viral illness. • To date none of the 10 index cases have had rhinorrhea associated with them. All had positive CXR”s • After 2-3 days of the above ( The patient may actually improve) the patient rapidly progresses to respiratory distress,shock and death. • Hemorrhagic meningitis is common CXR OF PULMONARY ANTHRAX • Widened mediastinum shown at right. • Pleural effusions common, usually hemorrhagic. • Most toxic patients also have hemorrhagic meningitis. • Chest wall edema. PULMONARY ANTHRAXCONTINUED • This disease is so rare that even as few as two cases can be interpreted as evidence that a biologic attack is being waged. • Diagnosis mad by Blood, CSF, or pleural fluid. • Mortality 89- 100% (Pre antibiotic Critical Care era. TREATMENT • Largely supportive • Ciprofloxacin or Doxycycline the initial therapy, given the high incidence of Penicillin resistance. Can adjust therapy based on culture results • Therapy must be continued for 60 days given the persistant germination of spores. VACCINE • Available in the UK and USA. • Purified Protective Antigen adsorbed onto aluminum adjuvant. • Six .5 cc shots over 18 months; military feels that a three shot series will protect individual for 6 months after series. • Local reactions common.(6%) Don’t give to people with prior exposure NO DATA THAT ANY OF THESE WILL PROTECT FROM AN AEROSOL CHALLENGE!!!!! ANTIBIOTIC PROPHYLAXIS RECOMENDED FOR ANY IMMINENT BIOLOGIC WEAPON! PLAGUE • Zoonotic disease transmitted by infected fleas or by aerosol in a biologic. Person to person also seen in Pneumonic plague. • 30 types of fleas and over 200 different mammals can harbor the bacteria. • Move to Australia or Antarctica. • Bubonic, septicemic, and inhalation syndromes all known. BUBONIC • 1-10 day incubation period then high fever malaise and purulent lymphadenopathy of the groin, but also seen in cervical and axillary lymph nodes, and a plethora of rashes seen. • 80% of these patients blood culture positive but only 25% progress to the septicemic form. SEPTICEMIC PLAGUE • These patients behave like your basic septic patient; fever chills hypotension and shock plus often nausea, vomiting and diarrhea. • Often develop acral thrombosis; clotting and gangrene of extremities, and skin with more proximal purpura. • Can progress to pnumonic both by bloodstream and inhalation. PNEUMONIC • 2-3 DAY INCUBATION FOR BOTH. • Cough, dyspnea sputum/blood, toxemia, rapidly progressing to acute respiratory failure. CXR shows patchy bilateral alveolar infiltrates • Preterminal events are circulatory collapse hemorrhage and peripheral thrombosis in septicemic and bubonic. • Mortality 50%bubonic and septicemic, 100% for pneumonic. Pneumonic Plague • 2-3 day incubation period • Non-specific complaints, but hemoptysis is common • Secondary transmission is possible • Treatment: streptomycin IM or IV gentamicin or IV doxycycline • Prophylaxis: po ciprofloxacin or doxycycline MORTALITY FROM PLAGUE • Pulmonary form still 50 % mortality even with antibiotics. Less than 5% with the other forms. • Death most likely even with therapy if treatment delayed beyond 18 hours of infection. Again Cipro and Doxycycline. • These facts plus a flea vector and person to person make plague a serious threat. OTHER BACTERIAL BIOLOGICS • Tularemia- Non spore bacterium that spreads by skin, mucosa, GI, and Pulmonary(as few as 50 organisms needed for pulmonary infection.) • Arthropods, contact, ingestion, handling of meat or inhalation are potential vectors. • Glandular, septicemic, pneumonic,forms seen as well as ulceroglandular and oculoglandular OTHER BACTERIAL AGENTS • Cholera; Darkfield and Phase contrast microscopes and culture. IV therapy for vomiting, losing greater than 7 liters a day, and shock. Killed vaccine that only protects for 6 months. Bactrim, Doxy, and TMP/SMX. • Pssitacosis(Parrot fever) 1-2 weeks incubation aerosolized dried droppings, aerosol and human to human. Fever Nausea, vomiting,myalgias and atypical pneumonia. Erythromycin and Doxycline. • Brucellosis THE VIRAL WEAPONS • • • • Smallpox Q fever (rickettsial) Venezuelan Equine Encephalitis Anything else SMALLPOX • • • • First described 2000 years ago. ? Origin in India, or Western Asia. Reached Europe by 700 AD. It killed more American Indians than European bullets in its spread to North America. (in the French Indian War we gave Indians blankets known to have come from smallpox patients). SMALLPOX • Variola virus and Orthopox virus. • Last “wild case” reported in 1977. • Transmitted by face-face, secretions, and aerosols. • Aerosols are deactivate by UV light within 24 hours. So SUPPOSEDLY patients presenting ill probably not need to be decontaminated. THE FACE OF SMALLPOX FACTS ABOUT SMALLPOX… • Approximately 10-17 day incubation period ending in a 2-3 day viral prodrome (fever, headache, neck and backache). • Rash follows soon afterwards. Starts as macules, turning to papules, which become vesicles and lastly pustules which crust over by approximately the 10th day. • If you have the rash you are infectious. FACTS ABOUT SMALLPOX…. • Variola Major and minor. Major was displayed on the previous slide and Minor is just less intense (look at day 3). • Minor most likely manifestation in partially immunized folks. • Two variants; Hemorrhagic and Malignant. Both have shorter prodromes. Former rapidly progresses to DIC like picture, and the latter becomes fulminant before vesicles/pustules form. Hemorrhagic Smallpox especially common in pregnant females. FACTS ABOUT SMALLPOX… • Complications are scarring (keratitis with ocular involvement), smallpox pneumonia, and arthritis which can cause permanent deformities. • Obviously if this got out, medical resources would be severely depleted beyond the 25% mortality projected for the disease. • All pediatric and most adults not immune. • Many more older, immunosuppressed people to deal with than in the past. FACTS ABOUT SMALLPOX… • The one thing that slows its spread is the fact that the patient is so ill that they are usually bed bound by the time the rash appears. • In a hospital this can be disastrous. In Germany one case with a cough in isolation managed to contaminate THREE FLOORS of a hospital. Disease can pass 10-20 generations from a single index case. • Think about spring breaks and Disney World. Therapy • Ribavirin, cidfovir and a derivative of the latter are available but have never actually been used in a smallpox case. • Vaccination within 4 days of exposure has been shown to decrease both the course and mortality of the disease. • In the event of an outbreak we all need a shot. • Diagnosis clinical, but DFA, electron microscopy and culture are all available. Which depends on facility. SMALLPOX • WHO has approximately 500,000 vaccines available. • USA approximately 10 million with an additional 50-60 million in various locations. • A question of potency and adequate storage of these vaccines has been raised. • Problem in the immunosuppressed. • 18 deaths in the 1961-62 in UK epidemic SMALLPOX • All possessions of the patient need to be steam cleaned or cleansed in bleach or other hospital grade cleanser. • Clothes and sheets should be autoclaved. • This is where I disagree with recommendations that patients presenting with smallpox don’t need decontamination. • Potential exposure with fever >101 is isolated before they have a rash and infect others!!!!!! Q FEVER • Coxiella Burnetti, not a virus but a rickettsia; 10-20 day incubation followed by a self limited illness 2days to 2weeks. Pneumonia is common and atypical in presentation, and hepatitis seen in 1/3 of the cases. One inhaled organism can cause disease. • Complications include chronic hepatis, endocarditis, meningitis,encephalitis and osteomyelitis • Diagnosis is by ELISA,Doxycycline and Erythromycin. Venezuelan Equine Encephalitis • VEE for short. There is also Western and Eastern (WEE and EEE). • Arthropods and aerosol. No evidence of Horse to Human or Human to Human transmission. ELISA Tests for Dx. • 1-6 day incubation, 24-72 hour acute phase of fevers,rigors,headache,malaise, photophobia and myalgias. Viral Hemorrhagic Fever • Ebola/Marburg/Lassa • Easily grown/ highly infectious when aerosolized • Symptoms: fever, malaise, signs of vascular permeability – – – – Conjunctival injection Hypotension Flushing Petechial hemorrhage • Treatment: supportive – ? ribavirin Botulism Toxin • • • • Most potent toxin known Easily isolated Can be food-borne or aerosolized IP = 3-8 days if acquired po, 24-36 hours if inhaled • Diagnosis: clinical – Bulbar palsies, descending paralysis, respiratory failure – No fever • Treatment: supportive – Antitoxin available from CDC or military ANY QUESTIONS??????? Thank you very much.