Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
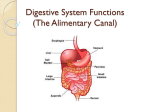
Physiology and Pharmacology of the Large Intestine Professor John Peters e-mail [email protected] Learning Objectives After this lecture, students should be able to: Describe the structure and function of the large intestine and the patterns of motility that it exhibits Provide an account of the defaecation reflex Outline the causes of constipation and its treatment by purgatives Describe water balance within the G.I. Tract Understand the principles of oral rehydration therapy and the role of SGLT1 in this process Outline the causes of diarrhoea and its treatment by antimotility agents The Large Intestine - General Approximately 1.5 m long, 6 cm diameter Comprises • Colon o Ascending o Transverse o Descending o Sigmoid • Caecum • Appendix • Rectum Normally receives approximately 500 ml of chyme (indigestible residues, unabsorbed biliary components, unabsorbed fluid) per day – entry permitted by the gastroilial reflex Is primarily involved in: • Absorption of fluids and electrolytes (Na+, Cl-) • Secretion of electrolytes (K+ and HCO3-) and mucus • Formation, storage and periodic elimination of faeces Patterns of Motility in the Large Intestine (1) Haustration Peristaltic propulsive movements Mass movement Defaecation Haustration - haustra are saccules caused by contraction of the circular muscle – similar to segmentation in function, but much lower frequency Peristaltic propulsive movement – occur in both the aboral and oral directions. Oral movements occur principally in the ascending and transverse colon – contributes to long transit time (16 – 48 hours) Mass movement – simultaneous contraction of large sections (about 20 cm) of the circular muscle of the ascending and transverse colon - drives faeces into distal regions • • Occurs about one to three times daily Typically triggered by a meal (often breakfast) via the gastrocolic response involving o gastrin o extrinsic nerve plexuses Patterns of Motility in the Large Intestine (2) Defaecation Pelvic nerve Activation of afferents to spinal cord Activation of parasympathetic efferents Mass movement rectum fills with faecal matter Activation of rectal stretch receptors Activation of afferents to brain (urge to defaecate) Contraction of smooth muscle of colon and rectum – internal anal sphincter relaxes Relaxation of skeletal muscle of external anal sphincter Defaecation assisted by abdomenal contraction and expiration against closed glottis Pudendal nerve Altered firing in efferents to spinal cord Contraction of skeletal muscle of external anal sphincter Defaecation delayed – rectal wall gradually relaxes CONSTIPATION and PURGATIVES Numerous causes of constipation: e.g. improper diet, drugs, metabolic disorders Constipation is the presence of hard dried faeces within the colon Pugatives: increase peristalsis and/or soften faeces causing, or assisting, evacuation are resorted to far too readily in some societies by individuals obsessed by ‘regularity’ can be abused in eating disorders and may also disguise underlying disease Medically sound uses of laxatives include: • when ‘straining’ is potentially damaging to health (e.g. patients with angina), or when defaecation is painful (e.g. haemorrhoids) predisposing to constipation • to clear the bowel before surgery or endoscopy • to treat drug-induced constipation, or constipation in bedridden, or elderly patients PURGATIVES AND THEIR MECHANISM(S) OF ACTION Bulk laxatives (e.g. methylcellulose -orally) Stimulant purgatives (e.g. bisacodyl – oral or suppository) Retain H2O volume Retain H2O volume Osmotic laxatives (e.g. magnesium sulphate / hydroxide – orally sodium citrate – rectally) Stimulate peristalis; cause H2O and electrolyte secretion Faecal softening Faecal softners (e.g. docusate sodium – orally) Absorption of Water in the GI Tract Absorption of water is a passive process driven by the transport of solutes (particularly Na+) from the lumen of the intestines to the bloodstream Water ingested and secreted is normally in balance with water absorbed Typical values are: 9.3 litre entering tract per day 8.3 litre absorbed by small intestine 1 litre enters large intestine of which 90% is absorbed Thus faeces normally contain 100 ml water along with 50 ml cellulose, bilirubin and bacteria Diarrhoea is defined as loss of fluid and solutes from the GI tract in excess of 500 ml per day CAUSES OF DIARRHOEA (1) Diarrhoea can have numerous causes: infectious agents – viruses, bacteria (e.g. traveller’s diarrhoea) chronic disease toxins drugs psychological factors Diarrhoea may involve the small, or large, intestine can result in dehydration, metabolic acidosis (HCO3- loss) and hypokalaemia (K+ loss) may be fatal if severe (e.g. cholera) Treatment of severe acute diarrhoea can include: maintenance of fluid and electrolyte balance (first priority) use of anti-infective agents (if appropriate) use of non-antimicrobial antidiarrhoeal agents (symptomatic) CAUSES OF DIARRHOEA (2) • • • Impaired absorption of NaCl Congenital defects Inflammation Infection (e.g. enterotoxins from some strains of E.coli and campylobacter sp.) • Excess bile acid in colon Non-absorbable, or poorly absorbable, solutes in intestinal lumen • Lactase deficiency Hypermotility Excessive secretion • Cholera provides a classic (and extreme) example • • • • • • cholera toxin enters enterocyte enzymatically inhibits GTPase activity of the Gs subunit increased activity of adenylate cyclase increased concentration of cAMP cAMP stimulates CFTR hypersecretion of Cl-, with Na+ and water following Na+/K+ ATPase Na+/K+/2Clco-tranporter Chloride channel (CFTR) Rehydration Therapy Exploits SGLT1 1. 2 Na+ bind 2. Affinity for glucose increases, glucose binds 3. Na+ and glucose translocate from extracellular to intracellular 4. 2 Na+ dissociate, affinity for glucose falls 5. Glucose dissociates 6. Cycle is repeated Oral rehydration salts contain (for example) • Glucose 20 g • Sodium chloride 3.5 g • Sodium bicarbonate 2.5 g • Potassium chloride 1.5 g Dissolved in a volume of 1 L drinking water Absorption of Na+ and glucose by SGLT1 cause accompanying absorption of H20 ANTIMOTILITY AGENTS USED IN TREATMENT OF DIARRHOEA Many morphine-like (or opiate) drugs have anti-diarrhoeal activity The actions of opiates on the alimentary tract include: • inhibition of enteric neurones (hyperpolarization via activation of -opioid receptors) • decreased peristalis, increased segmentation (i.e. constipating) • increased fluid absorption • constriction of pyloric, ileocolic and anal sphincters The major opiates used in diarrhoea are: • codeine • diphenoxylate - low CNS penetration, low solubility in water (abuse potential) • loperamide – low CNS penetration, low solubility in water, undergoes enterohepatic recycling