Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
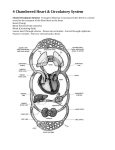
CARDIOVASCULAR SYSTEM • The entire cardiovascular system – the heart, blood vessels, and blood cells – originate from the Mesodermal germ layer. • The vascular system of the human embryo appears in the middle of the 3rd week. Angiogenic Cell Clusters • The origins of the heart tube are clusters of Angiogenic cells which are located in the cardiogenic plate. The cardiogenic plate, which is derived from splanchnopleuric mesoderm, is located cranial to the neural plate. Endocardial Tubes • These Angiogenic cell clusters coalesce to form right and left endocardial tubes. • Each tube is continuous cranially with a dorsal aorta, its outflow tract, and caudally with a vitteloumbilical vein, its inflow tract. • The lateral and cranial folding of the embryo forces the tubes into the thoracic cavity. As a result, these tubes come to lie closer to each other and begin to fuse in a cranial to caudal direction. • At approximately day 21 they are completely fused. Heart Tube • The newly formed heart tube bulges into the pericardial cavity and is attached to the dorsal wall by a fold of tissue, the dorsal mesocardium. This is a derivative of foregut splanchnoplueric mesoderm. Eventually this will rupture leaving the heart tube suspended in the pericardial cavity anchored cranially by the dorsal aortae and caudally by the vitteloumbilical veins. • As it bulges into the cavity it becomes invested in a layer of myocardium. A layer of acellular matrix, the cardiac jelly, separates the myocardium and the endothelial heart tube. • The newly formed heart tube may be divided into different regions. Starting caudally: • Sinus venosus - consisting of right and left horns. • Paired primitive atria. These structures will later fuse together to form common atrium. • Atrioventricular sulcus divides the atria and the primitive ventricle. • Primitive ventricle expands to become the left ventricle. • Interventricular sulcus divides the primitive ventricle and the bulbus cordis • Bulbus cordis which may be divided as follows: • Bulbus cordis - the proximal portion forms the right ventricle • Conus cordis • Truncus arteriosus • Aortic sac –By the time the heart tube has formed the bulboventricular loop, the two primitive right and left atria have fused to form a common atrium. –Note that it now lies cranial to the primitive ventricle and dorsal to the bulbus cordis. –The truncus arteriosus lies on the roof of the common atrium causing a depression and indicates where septation of the atrium will occur. • The partitioning of the atrium begins with the appearance of septum primum at about the 28th day. • This is a crest of tissue that grows from the dorsal wall of the atrium towards the endocardial cushions - - the ostium (opening) formed by the free edge of septum primum is the ostium primum. • Before the septum primum fuses with the endocardial cushions, perforations appear in the upper portion of the septum primum. • These perforations will coalesce to form the ostium secundum • Septum secundum does not fuse with the endocardial cushions. • Its free edge forms the foramen ovale. • The left venous valve and the septum spurium, located on the dorsal wall of the right atrium, fuse with the septum secundum as it grows. • At the end of the seventh week the human heart has reached its final stage of development. • Because the fetus does not use its lungs, most of the blood is diverted to the systemic circulation. This is accomplished by a right to left shunting of blood that occurs between the two atria. • The foramen ovale and the septum primum control this right and left communication. • The septum primum acts as a valve over the foramen ovale. • At birth the child will use its lungs for the first time and consequently more blood will flow into the pulmonary circulation. • The pressure increase in the left atrium (where the pulmonary veins empty) will force septum primum to be pushed up against septum secundum. • Shortly thereafter the two septa fuse to form a common atrial septum. Sinus Venosus Each horn receives venous blood from three vessels: 1. Vitelline vein 2. Umbilical vein 3. Common cardinal vein The fate of each structure is as follows: • the right sinus horn becomes enlarged • the right common cardinal vein ( along with some proximal portion of right ant. Cardinal vein) becomes the superior vena cava. • the right Vitelline vein becomes the inferior vena cava • the right umbilical vein is obliterated • Conversely, the left vein counterparts are obliterated and the left sinus horn diminishes in size and forms the coronary sinus and the oblique vein of the left atrium. Pulmonary veins • Development of the left atrium occurs concurrently with that of the right atrium. • During the early part of the fourth week an outgrowth of the pulmonary veins appear from the left atrium. • This "sprout" will bifurcate until there are four veins. • These vessels will then grow towards the lung buds. Ventricles • Primitive ventricle expands to become the left ventricle. • Externally the interventricular sulcus separates the right and left ventricles and internally they are separated by the bulboventricular tissue • Bulbus cordis - the proximal portion forms the right ventricle • Both ventricles will continue to expand until the late 7th/early 8th week. The growth of the ventricles is due to the centrifugal growth of the myocardium and the diverticulation of the internal walls • The muscular interventricular septum forms as a result of the expanding ventricles. • The walls of the right and left ventricles grow in opposition to each other to form the muscular septum. • Thus, the septum will cease to grow when the ventricular walls are no longer expanding. Atrioventricular canals • Swellings of mesenchymal tissue, the endocardial cushions, appear on the borders of the atrioventricular canal • There are four cushions: inferior and superior (ventral and dorsal), left and right. These swellings give the atrioventricular canal a "dog's bone" shape. • At approximately day 42 the superior and inferior cushions fuse forming a right and a left atrioventricular canal. • Now, the left atrium communicates with the left ventricle and the right atrium communicates with the right ventricle • The fused endocardial cushions are also responsible for the closure of the ostium primum by fusing with the free edge of the septum primum Partitioning of the Outflow Tract • The final morphological change in the heart is the partitioning of the outflow tract - -the truncus arteriosus and the conus cordis - - into the aorta and the pulmonary trunk. • This is accomplished by the development of a septum that forms in the outflow tract and the emergence of the two great vessels. • The septum forms from two pairs of swellings which grow from the walls of the outflow tract. These are the truncus swellings and the conus swellings Truncal swellings • Right superior which grows distally and to the left. Left inferior which grows distally and to the right. Both develop at the proximal part of the truncus and proceed to grow in two directions; 1) distally towards the aortic sac and 2) into the lumen of the outflow tract where they will eventually fuse together Conus swellings • Right dorsal which is continuous with the right superior Left ventral which is continuous with the left inferior like the truncal swellings, the conal swellings grow distally and towards each other, however they appear after the truncal swellings. Arterial system (Aortic arches) • Branchial arches has own artery. These arteries are known as Aortic arches. • Aortic arteries arise from aortic sac, the most distal part of the truncus arteriosus. • Total six pairs of arteries arise corresponding to arches. • Aortic sac forms right and left horns— brachiocephalic artery. • 1st aortic arch (part) - maxillary artery. • 2nd aortic arch some part forms hyoid and stapedial arteries. • Rest of 1st and 2nd arch disappears. • 3rd aortic arch- common carotid artery and first part of the internal carotid artery and external carotid artery. • 4th aortic arch Left side—arch of aorta. Right side – proximal segment of the right subclavian artery. • Fifth aortic arch is transient and is never well developed. • 6th aortic arch (pulmonary arch) Right side – proximal part forms proximal segment of the right pulmonary artery. Left side -- the distal part persists during intra uterine life as the ductus arteriosus. Vitelline arteries • Initially a number of paired vessels supplying the yolk sac, gradually fuse to form the arteries located in the dorsal mesentery of the gut. • They are represented by celiac, superior mesenteric and inferior mesenteric arteries. Umbilical arteries • The proximal portion after birth is represented as internal iliac and superior vesical arteries. • While the distal parts are obliterated to form the medial umbilical ligaments. Venous system Mainly 3 pairs of major veins formed in 5th week. 1.Vitelline or Omphalomesenteric veins carrying blood from the yolk sac to the sinus venosus. 2. Umbilical veins—originating in the chorionic villi and carrying oxygenated blood to the embryo. 3. Cardinal veins- draining the body of the embryo proper. • The anastomatic network of Vitelline veins around the duodenum develops into single vessel (vein) - PORTAL VEIN. Umbilical veins • With the increase of the placental circulation, a direct communication is formed between the left umbilical vein and the right hepatocardiac channel , by DUCTUS VENOSUS. • After birth left umbilical vein and ductus venosus are obliterated and form the ligamentum teres hepatis and ligamentum venosum respectively. Cardinal veins • Anterior cardinal veins- drain cephalic part of the embryo. • Posterior cardinal vein- drain remaining part of the body of the embryo. • Anterior and posterior veins join to form short common cardinal veins. Contd.. Cardinal veins • Other than this • Subcardinal veins- drain kidneys. • Sacrocardinal veins- drain lower extremities. • Supracradinal veins- drain body wall. • Anastomosis between the anterior cardinal veins develops into left brachiocephalic vein. Contd.. Cardinal veins • Superior vena cava is formed by the right common cardinal vein and the proximal portion of the right anterior cardinal vein. • Anastomosis between the Subcardinal veins forms the left renal vein. • Anastomosis between the Sacrocardinal veins forms the left common iliac vein. Abnormalities of Great Arteries • PATENT DUCTUS ARTERIOSUS- under normal condition the ductus arteriosus is functionally closed through contraction of its muscular wall shortly after birth. • Patent ductus arteriosus is one of the most frequently seen abnormalities of the great vessels. Abnormalities of Great Arteries • Coarctation of the Aorta In this condition the aortic lumen below the origin of the left subclavian artery is significantly narrowed. The umbilical vein enters the body through the umbilical ring and travels along the anterior abdominal wall to the liver. • About 1/2 the blood it carries passes into the liver. • The other 1/2 of the blood enters a vessel called the ductus venosus which bypasses the liver. – The ductus venosus travels a short distance and joins the inferior vena cava. – There, the oxygenated blood from the placenta is mixed with the deoxygenated blood from the lower parts of the body. This mixture continues through the vena cava to the right atrium In the adult heart, blood flows from the right atrium to the right ventricle then through the pulmonary arteries to the lungs. In the fetus however, the lungs are nonfunctional and the blood largely bypasses them. • As the blood from the inferior vena cava enters the right atrium, a large proportion of it is shunted directly into the left atrium through an opening called the foramen ovale. • Septum primum is located on the left side of the atrial septum overlies the foramen ovale and helps prevent blood from moving in the reverse direction. Thus, acting as a valve. The rest of the fetal blood entering the right atrium, including a large proportion of the deoxygenated blood entering from the superior vena cava passes into the right ventricle and out through the pulmonary trunk. Only a small volume of blood enters the pulmonary circuit, because the lungs are collapsed, and their blood vessels have a high resistance to flow. Enough blood reaches the lung tissue to sustain them. Most of the blood in the pulmonary trunk bypasses the lungs by entering a fetal vessel called the ductus arteriosus which connects the pulmonary trunk to the descending portion of the aortic arch. • As a result of this connection, the blood with a relatively low O2 concentration which is returning to the heart through the superior vena cava, bypasses the lungs. • At the same time, the blood is prevented from entering the portion of the aorta that provides branches leading to the brain. • The more highly oxygenated blood that enters the left atrium through the foramen ovale is mixed with a small amount of deoxygenated blood returning from the pulmonary veins. • This mixture moves into the left ventricle and is pumped into the aorta. • Some of it reaches the myocardium through the coronary arteries and some reaches the brain through the carotid arteries. • The blood carried by the descending aorta is partially oxygenated and partially deoxygenated. • Some of it is carries into the branches of the aorta that lead to various parts of the lower regions of the body. • The rest passes into the umbilical arteries, which branch from the internal iliac arteries and lead to the placenta. • There the blood is reoxygenated. Lymphatic system • Lymphatic system begins its development after CVS. • The exact origin is not clear but may be from mesenchyme. • As a result 6 primary lymph sacs are formed. • Two jugular, two iliac, one retroperitoneal and one cisterna chyli. • Numerous channels contact the sacs with each other and also drain lymph from the entire body of the embryo proper. • The two main channels the right and left thoracic ducts join the jugular sacs with the cisternachyli, and forma an Anastomosis. • Thoracic duct develops from dorsal portion of right thoracic duct and Anastomosis and cranial portion of left thoracic duct. • Right lymphatic duct is derived from the cranial portion of the right thoracic duct. • Both ducts maintain their original connection with the venous system and empty in to the junction of the internal jugular and subclavian veins. CLASSIFICATION OF CHD Left to right shunt • VSD, ASD, PDA, PTA Right to left shunt • Tetralogy of Fallot No shunt • Transposition of great vessels • Stenosis, coarctation • Valvular anomalies Atrial Septal Defect • There are two types of ASD: • Primum type involves the endocardial cushions. • Secundum type involves septum primum or septum secundum ATRIAL SEPTAL DEFECT Ostium secundum type (90%) Ostium primum type Sinus venosus defect Persistent common atrioventricular canal DD: patent foramen ovale (25% adults) Secundum Type ASD • This type involves septum primum and/or septum secundum. In both cases the result is a patent foramen ovale. Persistent Atrioventricular Canal • The persistent atrioventricular canal results from the failure of the superior and inferior cushions to fuse • Thus there is a single atrioventricular canal in which all four chambers may freely communicate Ventricular Septal Defect • The ventricular septal defect is the most common of all congenital heart anomalies. It may be caused by any of the four malformations: (1) Deficient development of the proximal conus swellings. (2) Failure of the muscular portion of the interventricular septum to fuse with the free edge of the conus septum. (Membranous VSD) (3) Failure of the endocardial cushions to fuse. (4) Excessive diverticulation of the muscular septum- perforations in the muscular interventricular septum. (Muscular VSD) • In the case of a VSD there is a massive left to right shunting of blood and pulmonary hypertension. • The absence of the interventricular septum sometimes results in a Common Ventricle Transposition of the Great Vessels • Transposition is a condition in which the aorta arises from the right ventricle and the pulmonary trunk from the left ventricle. • This anomally is due to the failure of the truncoconal swellings to grow in the normal spiral direction • Mostly in Transposition ,there is also a ventricular septal defect and a patent ductus arteriosus. • These secondary defects make life possible as they provide a way for oxygenated blood to reach the entire body Persistent Truncus Arteriosus • Mostly persistent truncus arteriosus results when the truncoconal swellings fail to grow • Again there also there is mixture of the blood. Tetralogy of Fallot • This condition commonly and mainly results from a single error: the conus septum develops too far anteriorly giving rise to two unequally proportioned vessels- a large aorta and a smaller stenotic pulmonary trunk. The four main characteristics of Tetralogy of Fallot are: (1) Pulmonary stenosis (2) Ventricular septal defect (VSD) of the membranous portion (3) Overriding aorta (the aorta straddles the VSD) (4) Right ventricular hypertrophy due to the shunting of blood from left to right. (The pressure in the right ventricle is increased causing the walls of the right ventricle to expand.) Dextrocardia • Mostly seen variety is due to • Dextrocardia is an anomaly in which the primitive heart tube folds to the left in a mirror image of a normal bulboventricular loop. • This usually occurs when all the organ systems are reversed, a condition called situs inversus.