Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
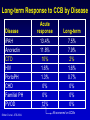
VASCULAR COMPLICATIONS OF SYSTEMIC SCLEROSIS Wednesday, November 15, 2006 • Washington, DC • Richard M. Silver, MD, Program Chair VASCULAR COMPLICATIONS OF SYSTEMIC SCLEROSIS Treatment Targets for PAH in Systemic Sclerosis Myung H. Park, MD, FACC Assistant Professor of Medicine Director, Pulmonary Vascular Diseases Program University of Maryland Medical Center Baltimore, Maryland VASCULAR COMPLICATIONS OF SYSTEMIC SCLEROSIS DISCLOSURE STATEMENT Myung H. Park, MD, FACC Grants/research support: Actelion Pharmaceuticals US, Inc., CoTherix, Inc., United Therapeutics Consultant: Actelion Pharmaceuticals US, Inc., CoTherix, Inc., Myogen, Inc., Pfizer Inc, United Therapeutics Speakers’ bureau: Actelion Pharmaceuticals US, Inc., Encysive Pharmaceuticals Inc., Pfizer Inc, United Therapeutics Off-label uses for products may be discussed. Definition of Pulmonary Arterial Hypertension • Pulmonary arterial hypertension: – Mean PAP >25 mm Hg at rest – Mean PAP >30 mm Hg with exercise • Normal pulmonary capillary wedge pressure (<15 mm Hg) Barst, RJ et al. J Am Coll Cardiol. 2004;43:40S- 47S. Incidence of Pulmonary Hypertension • Population Incidence – Primary 4 : 500,000 – Familial 1 : 30,000,000 • Disease Specific Incidence Chest 2003. – Connective Tissue 1 : 10 – 1 : 1,000 – Portopulmonary 8 : 1,000 – HIV 1 : 5,000 – Anorexigens (>3 mo) 1 : 17,000 – Anorexigens (>6 mo) 1 : 10,000 – CTEPH 1 : 10,000 Connective Tissue Disease: Major Risk Factor for Development of PAH Connective Tissue Disease (CTD) • Most common and severe in CREST – Diffuse scleroderma—up to 33% – Limited scleroderma (CREST)—25%30% – SLE—4% to 14% – RA—up to 21% (mild) • PH most common cause of death in CREST • Identical to iPAH pathology • Medical treatment same as for iPAH – But benefits less than for iPAH CREST=Calcinosis cutis, Raynaud’s phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasia. 2003 WHO Pulmonary Hypertension Diagnostic Classification 1. Pulmonary Arterial Hypertension 3. PH With Lung Diseases/Hypoxemia • Idiopathic PAH (Formerly iPAH) • COPD • Familial PAH • Interstitial lung diseases • Related to: • Sleep-disordered breathing – Connective tissue diseases – HIV • Developmental abnormalities – Portal hypertension 4. PH Due to Chronic Thrombotic and/or Embolic Disease – Anorexigens • TE obstruction of proximal PA – Congenital heart disease • TE obstruction of distal PA • Portopulmonary hypertension • PAH with venule/cap involvement • Nonthrombotic pulmonary embolism 5. Miscellaneous 2. Pulmonary Venous Hypertension • Sarcoidosis • Atrial or ventricular heart disease • Pulmonary histocytosis • Valvular heart disease • Lymphangiomatosis Observed 5-Year Survival Without Treatment in iPAH: National Registry 100 1 yr: 68% 80 3 yr: 48% % Surviving 60 5 yr: 34% 40 Median survival: 2.8 yrs 20 0 0 0.5 1.0 1.5 2.0 2.5 3.0 Years of follow-up Adapted from: D’Alonzo GE et al. Ann Int Med. 1991;115:343-349. 3.5 4.0 4.5 5.0 Survival Comparison of Patients With SScPAH and iPAH With Similar Hemodynamics 1.0 0.8 Survival (%) 0.6 iPAH 0.4 SSc-PAH 0.2 Log-rank text2=4.88 p=0.03 0 No. at risk: SSc-PAH: iPAH: 0 1 22 33 7 24 Kawut SM et al. Chest. 2003;123:344-350. 2 3 Time (yrs) 4 5 – 9 – 3 – – 3 15 Pulmonary Arterial Hypertension: Understanding the Pathobiology Insult Vascular Injury Genetic predisposition Neurohormonal Imbalance Vascular Remodeling and Dysfunction Disease Progression Gaine SP, Rubin LJ. Lancet. 1998;352:719-725. Cardiac Hypertrophy Neurohormonal Imbalance in PAH Increased Activity Endothelin-1 Angiopoietin-1 PAI-1 Growth factors PDGF Reduced Activity Prostacyclin Nitric oxide VIP PAI = plasminogen activator inhibitor. VIP = vasoactive intestinal peptide. McLaughlin V et al. Circulation. 2006:114. Therapeutic Options for PAH General Tx • Supplemental O2 FDA Approved for PAH Investigational Tx • Prostanoids • Prostanoids • Diuretics – epoprostenol • CCB – treprostinil (SC,IV) • Warfarin – inhaled iloprost • Digitalis • ERAs – bosentan • PDE-5 Inhibitors – sildenafil – Inhaled treprostinil – Oral treprostinil • ERAs – sitaxsentan – ambrisentan • PDE-5 Inhibitor – tedalafil ACCP Grading System for Recommendations Net Benefit to Patient (adjusted for risk and based on clinical assessment) Quality of Evidence Good: Fair: Low: Expert Opinion: Substantial Intermediate Small/Weak None Conflicting Negative Good A A B D I D Fair A B C D I D Low B C C I I D Expert Opinion E/A E/B E/C I I E/D Evidence is based on good randomized controlled trials or meta-analysis Evidence is based on other controlled trials or other RTCs with minor flaws Evidence is based on non-randomized, case-control, or other observational studies Evidence is based on consensus of carefully selected panel of experts. There are no published studies that meet the criteria for inclusion in the literature review. McCrory DC et al. Chest 2004;126. Therapy for PAH Functional class II/III/IV General Care Oral anticoagulants (B for iPAH, E/C for other PAH) + diuretics + oxygen (E/A) + digoxin Acute Vasoreactivity Testing (A for iPAH, E/C for PAH) Negative Positive Oral CCB (B for iPAH, E/B for other PAH) Sustained Response Functional Class III Endothelin receptor antagonists bosentan (A) or Yes No Continue CCB Chronic IV epoprostenol (A) bosentan (B) Chronic IV epoprostenol (A) treprostinil (B) or Prostanoid Analogues Chronic IV iloprost (C) SC treprostinil (B), Inhaled iloprost (B), beraprost (l) PDE-5 Inhibitors (sildenafil) (C) Badesch D et al. Chest. 2004;126. Functional Class IV No improvement or deterioration Atrioseptostomy Lung Transplantation Therapy for PAH Functional class II/III/IV General Care Oral anticoagulants (B for iPAH, E/C for other PAH) + diuretics + oxygen (E/A) + digoxin Acute Vasoreactivity Testing (A for iPAH, E/C for PAH) Negative Positive Oral CCB (B for iPAH, E/B for other PAH) Sustained Response Functional Class III Endothelin receptor antagonists bosentan (A) or Yes No Continue CCB Chronic IV epoprostenol (A) bosentan (B) Chronic IV epoprostenol (A) treprostinil (B) or Prostanoid Analogues Chronic IV iloprost (C) SC treprostinil (B), Inhaled iloprost (B), beraprost (l) PDE-5 Inhibitors (sildenafil) (C) Badesch D et al. Chest. 2004;126. Functional Class IV No improvement or deterioration Atrioseptostomy Lung Transplantation Anticoagulation Therapy for Pulmonary Arterial Hypertension • Idiopathic PAH – Improved survival reported with oral anticoagulation in iPAH1, – In situ microscopic thrombosis documented in patients with iPAH – RV failure and venous stasis increases risk of pulmonary thromboembolism – Recommended target INR1.5-2.5 but varies from center to center • PAH associated with other diseases - controversial – Consider risk/benefit ratio • Scleroderma – risk of increased GI bleeding higher • Consider if right ventricle is enlarged and systolic dysfunction present Badesch D et al. Chest. 2004;126. 1Rich S et al. N Engl J Med .1992;327. Conventional Therapies • Diuretics • Digoxin – Reduce peripheral – May increase contractility edema, intravascular in refractory right heart volume, and venous failure pressure – Can be useful in patients – Avoid excessive with atrial tachyarrhythmia diuresis • Oxygen – Combination of loop diuretics and – Supplemental oxygen to spironolactone may be maintain oxygen saturation beneficial >90% at all times – Hypoxemia is a potent vasoconstrictor Badesch D, et al. Chest. 2004;126 Therapy for PAH Functional class II/III/IV General Care Oral anticoagulants (B for iPAH, E/C for other PAH) + diuretics + oxygen (E/A) + digoxin Acute Vasoreactivity Testing (A for iPAH, E/C for PAH) Negative Positive Oral CCB (B for iPAH, E/B for other PAH) Sustained Response Functional Class III Endothelin receptor antagonists bosentan (A) or Yes No Continue CCB Chronic IV epoprostenol (A) bosentan (B) Chronic IV epoprostenol (A) treprostinil (B) or Prostanoid Analogues Chronic IV iloprost (C) SC treprostinil (B), Inhaled iloprost (B), beraprost (l) PDE-5 Inhibitors (sildenafil) (C) Badesch D et al. Chest. 2004;126. Functional Class IV No improvement or deterioration Atrioseptostomy Lung Transplantation Correlation of Acute Response to Vasodilator to Long-Term Response to CCB in iPAH • Analyzed acute vasoreactivity testing in 557 patients with iPAH • Acute vasodilator used: PGI2 (n=150) or NO (n=407) • Acute responder: fall in both mPAP and PVR >20% from baseline – “20/20 criterion”. – 70 patients (12.6%) demonstrated acute response • Long term CCB responder: – NYHA I/II after 1 year on oral CCB without need for prostanoids and/or ERA – Only half of acute responders (6.8% of total) maintained response long-term Sitbon O et al. Circulation. 2005;111. Long-term Response to CCB by Disease Disease iPAH Anorectin CTD HIV PortoPH CHD Familial PH PVOD Sitbon O et al. ATS 2004. Acute response 13.4% 11.8% 10% 1.6% 1.3% 0% 0% 12% Long-term 7.5% 7.9% 2% 1.6% 0.7% 0% 0% 0% All worsened on CCBs Therapy for PAH Functional class II/III/IV General Care Oral anticoagulants (B for iPAH, E/C for other PAH) + diuretics + oxygen (E/A) + digoxin Acute Vasoreactivity Testing (A for iPAH, E/C for PAH) Negative Positive Oral CCB (B for iPAH, E/B for other PAH) Sustained Response Functional Class III Endothelin receptor antagonists bosentan (A) or Yes No Continue CCB Chronic IV epoprostenol (A) bosentan (B) Chronic IV epoprostenol (A) treprostinil (B) or Prostanoid Analogues Chronic IV iloprost (C) SC treprostinil (B), Inhaled iloprost (B), beraprost (l) PDE-5 Inhibitors (sildenafil) (C) Badesch D et al. Chest. 2004;126. Functional Class IV No improvement or deterioration Atrioseptostomy Lung Transplantation Epoprostenol Improves 6-Minute Walk Test in PAH Due to Scleroderma 80 60 Median 40 change from 20 baseline (m) 0 Week 1 Week 6 Epoprostenol (n=56) Conventional (n=55) Week 12 p0.001 63.5 p=0.003 48.5 13.3 -7.0 -14.0 -20 -36.0 -40 Baseline: epoprostenol 271.5 m; conventional 240.0 m. Adapted from Badesch D et al. Ann Intern Med. 2000;132:425-434. Survival With Long-term Epoprostenol by Etiology 1.0 0.8 CHD Other Kaplan-Meier 0.6 survival estimates 0.4 iPAH Scleroderma 0.2 p=0.002 0 No. at risk: PAH CHD SSc Other 0 1 2 49 11 19 12 40 8 11 9 26 6 7 5 3 4 Time (yrs) 16 3 5 4 Kuhn KP et al. Am J Respir Crit Care Med. 2003;167:580-586. 11 1 2 4 5 6 7 9 0 0 1 2 0 0 0 1 0 0 0 Challenges Implementing Epoprostenol Therapy • Development of tolerance • Many side effects (diarrhea, flushing, headache, neuropathy) • Only approved for advanced stages of disease (Class III to IV) • Cost (average cost $50,000-150,000 per year) • Need for continuous delivery system – Risk associated with catheter placement – Line related complications (infection, thrombosis, pump failure) Treprostinil (Remodulin®) SC • Analog of epoprostenol • Lasts longer – more stable molecule (~4 hours vs 3-5 minutes for epoprostenol) • Room temperature stable – do not need ice packs • Rapid and complete absorption subcutaneously – bioavailability 100% • Change pump every 3 days with SC (instead of every day with epoprostenol) Treprostinil Sodium Injection: Change in Exercise vs Treprostinil Dose at Week 12 +36 ± 9 (N=58) Mean ± SE Change from Baseline (meters) 40 35 N=470 30 25 20 +15 ± 7 (N=58) 15 +7 ± 10 (N=52) 10 5 0 -4 ± 12 (N=34) -5 1st Quartile < 5.0 (2.5 ± 0.2) 2nd Quartile 5 to <8.2 (5.6 ± 0.1) 3rd Quartile 8.2 to <13.8 (9.4 ± 0.2) (Mean ± SE) ng/kg/min Simonneau G et al, Am J Respir Crit Care Med. 2002;165. 4th Quartile >13.8 (16.2 ± 0.4) Limitations of SC Treprostinil • Site pain is major impediment – Affects 85% – Not dose dependent – Treatments • Local measures: ice, heat, lidocaine • NSAIDs, narcotics, gabapentin • PLOgel – Patient education and support imperative for treatment success • pain • erythema • induration Open-Label Transition Study Results 6-Minute Walk Test Results: IV REMODULIN vs Flolan* Baseline on Flolan 438 m + 16 m NO Significant Change From Baseline 12 weeks on REMODULIN 439 m + 16 m P=NS N=27 *Data expressed as mean ± standard error. Safety results: 27 of 31 patients completed the study; 4 patients transitioned back to Flolan (3 due to leg pain, 1 with worsening PAH symptoms in setting of pneumonia). The most frequent adverse events were: extremity pain (71%), headache (45%), diarrhea (26%), and jaw pain (23%). One patient had syncope; 4 reported worsening dyspnea during titration. . Gomberg-Maitland M, et al. Am J Respir Crit Care Med. 2005;172:1586-1589. Inhaled Iloprost • Indicated for inhalation via the I-neb™ AAD® system only • 6-9 inhalations daily during waking hours – No more than once every two hours • Dose: maximum of 2.5 or 5 mcg per treatment • Side effects (headache, flushing, diarrhea) – Cough, Syncope • Advantage: Do not need a central line • Disadvantage: Compliance Effect of Inhaled Iloprost on Walk Distance 36 meters 36 meter difference Olschewski H et al. N Engl J Med. 2002;347. Endothelin Is A Key Pathogenic Mediator Proliferation Vasoconstriction vascular smooth muscle direct or via facilitation of other vasoconstrictor systems (renin angiotensin system, sympathetic) fibroblasts ET Hypertrophy cardiac/vascular Fibrosis fibroblast proliferation extracellular matrix proteins collagenase production Clozel. Ann Med. 2003:35;1-5. Inflammation vascular permeability neutrophil / mast cell activation promotes cellular adhesion cytokine production Endothelin Is a Key Mediator in PAH and PAH Secondary to Other Diseases 8 6 4 2 0 Non-PAH PAH Stewart et al., Ann Inter Med,1991; Concentration of ET-1(pg/ml) IrET-1 (pg/ml) 10 10 8 P<0.05 6 4 LcSSc Non-PAH LcSSc PAH Vancheeswaran et al., J. Rheum, 1994; Delta ET-LI (PV-RV) (pg/ml) Scleroderma iPAH 5 Congenital Heart Disease P<0.05 4 3 2 1 0 Non-PH PH Yoshibayashi et al., Circulation, 1991 Bosentan: Chemical Structure First Synthesis: December 1991 O O Pharmacokinetic Profile S N -H O O Orally active dual endothelin receptor antagonist O Bioavailability is ~50% and is not affected by food. N N N N O H Clozel M et al. J Pharmacol Exp Ther. 1994;270:228. Metabolized by the liver (CYP3A4 and 2C9) and eliminated via the bile. Bosentan (Tracleer®): BREATHE-1 • Randomized, double-blind, placebocontrolled • 16 week study • 213 patients with NYHA Class III or IV PAH – Idiopathic PAH (70%) – PAH associated with connective tissue disease (30%) • • • • Gender M / F: 22% / 78% Baseline 6MWD: 330 ± 74 meters WHO FC III / IV: 94% / 6% Mean PAP: 53 ± 17 mm Hg Rubin LJ et al. N Engl J Med. 2002;346. Bosentan and SSc-PAH Walk Test Change From Baseline to Study End SSc Pooled 40 All BREATHE-1 36 30 20 Placebo Bosentan 15 walk 10 distance 0 (m) -10 -8 -20 -30 -22 Bosentan (n=37) Placebo (n=15) Bosentan (n =144) Placebo (n=69) Adapted from Rubin LJ et al for the BREATHE Study Group. N Engl J Med. 2002;346:896-903, and Channick RN et al. Lancet. 2001;358:1119-1123. Data on file. BREATHE-1 SSc PATIENTS Event-Free (%) Time to Clinical Worsening* 100 90% Bosentan (n = 33) 75 Placebo (n = 14) 79% 50 25 0 0 4 8 12 16 18 Time (Wks) *Shortest time to death, premature withdrawal, hospitalization due to PAH worsening, or initiation of prostacyclin therapy. Bosentan Indication • PAH with WHO Class III (or IV) symptoms “to improve exercise capacity and decrease the rate of clinical worsening” • Caveat: Response may take time - up to 2 to 3 months – Patients should be informed – Should be used with caution in Class IV patients and not without right heart catheterization to document presence of PAH Bosentan Monitoring • Increase in liver enzymes – Seen in about 10-12% of patients – LFTs checked baseline and monthly – Dose related and reversible • Confirm elevation with another test • Stop if ALT/AST >3 ULN – evaluate for concomitant medication use • Consider reintroduction after resolution • Stop treatment if associated with clinical symptoms (eg, jaundice, fever, nausea, vomiting) • Dose 62.5 mg BID oral for 4 weeks. Titrate to 125 mg BID if LFTs stable. Side Effect Bosentan • Other side effects – Mild anemia – Teratogenic – Mild edema • Drug interactions – May decrease efficacy of hormonal contraception; barrier method advised – Contraindicated with glyburide and cyclosporine Differences in ET Receptors • ETA – Located on smooth muscle cells – Mediate vasoconstriction • ETB – Found on both endothelial and smooth muscle cells – Smooth muscle cells: mediates vasoconstriction – Endothelial cells: mediates vasodilation and clearance of ET-1 Selective vs Non-selective ERA? What Role Does ETB Receptor Play? • Controversial • Increased ETB receptor density in PH – spatial distribution not clear – Congenital heart disease • (Am J Respir Crit Care Med 2002;165) – Chronic thromboembolic PH • (Circulation 2002;105) – Scleroderma Other ERAs • Sitaxsentan: once daily specific ERA blocker – Phase III trials completed1 – Marketing application filed with the FDA, approval pending – Significant warfarin interaction – need to decrease dose by 80% – Less liver toxicity • Ambrisentan: once-daily specific ERA blocker (less than sitaxsentan) – Phase II trial showed ? less liver toxicity (3.1%), functional and hemodynamic improvements2 – Phase III trials underway 1. Barst RJ, et al. Am J Respir Crit Care Med. 2004;169:441-447. 2. Galie N, et al. J Am Coll Cardiol. 2005;46:529-535. Sildenafil for PAH: SUPER Study N 278 Age Mean: 49 y (range: 18-81 ) Gender 68 (25%) men; 209 (75%) women Primary Diagnosis iPAH: n=175 (63%) PAH secondary to CTD: n=84 (30%) PAH with surgical repair of congenital heart lesions: n=18 (6%) Mean 6-MWD distance 344 m mPAP 53 mm Hg Functional Classification Class I: n=1 (0.4%) Class II: n=107 (39%) Class III: n=154 (56%) Class IV: n=9 (3%) Dose 20, 40, 80 mg sildenafil or placebo in 1:1:1:1 Galie N et al. N Engl J Med. 2005:353:2148-2157. SUPER-1: Change in 6-MWD From Baseline to 12 Weeks Placebo Week 4 Sildenafil 20 mg n=278. Adapted from Galie N et al. N Engl J Med. 2005;353:38-47. Week 8 Sildenafil 40 mg 50 m 46 m *p<0.0001 * * * 45 m 70 60 50 40 30 from baseline 20 (m) 10 0 -10 -20 -30 Week 12 Sildenafil 80 mg PAH Determinants of Risk Lower Risk Determinants of Risk Higher Risk No Clinical evidence of RV failure Yes Gradual Progression Rapid II WHO class IV Longer (>400 m) 6MW distance Shorter (<300 m) Minimally elevated BNP Very elevated Minimal RV dysfunction Echocardiographic findings Pericardial effusion, significant RV dysfunction Normal/near normal RAP and CI Hemodynamics High RAP, low CI McLaughlin VV and McGoon M. Circulation. 2006;114:1417-1431. Summary • Multiple pathogenic pathways contribute to CTD-associated PAH – prostacyclin and NO cause vasodilatation, and smooth muscle proliferation – ET-1 production causes vasoconstriction, inflammation, fibrosis, cellular proliferation • Current targeted therapy has been demonstrated to improve clinical outcomes: – ERAs – PDE5 inhibitors – IV, SQ, or inhaled prostacyclin/prostanoid analogues • New treatment approaches are focusing on: – novel targets – improving delivery systems for current treatments – combination therapy to target multiple pathogenic pathways