Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Aortic stenosis wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Congenital heart defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
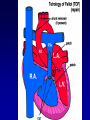
Tetralogy of Fallot Beth Harrison Advisor: Samuel Powdrill, PA-C PAS 646 Outline • • • • • • Review blood flow through the heart Discuss ToF anatomic abnormalities Etiology Clinical Presentation Labs and Exams Two surgical interventions Healthy Heart Blood Flow • Deoxygenated blood from the body enters the RA • At the same time, oxygen rich blood leaves the lungs to flow into the LA • Blood in the RA enters the RV through the tricuspid valve • At the same time, blood flows from the LA to the LV through the mitral valve Blood Flow cont. • Blood in the RV is pumped through the PA to the lungs • At the same time, LV pumps blood out the aorta to supply the body with oxygen rich blood • As seen in ToF, structural defects lead to the circulation of oxygen-poor blood ToF • 4 anatomic malformations: -Right Ventricular Hypertrophy -Pulmonary Valve Stenosis -Transposition of the aorta -Ventricular Septal Defect ToF • RVH -secondary to PA Stenosis -Increased P on RV leads to RVH • Transposition of Aorta -aorta is displaced • VSD -”hole in the heart” -mixing of oxygenated and unoxygenated blood -cyanosis • PVS -more severe, less blood transported to the lungs and more deoxygenated blood will pass through VSD to aorta to be circulated throughout the body Etiology • Theory: destruction of the neuronal crest cells during embryogenesis • In the laboratory setting, destruction of these cells reproduced results displayed with certain cardiac malformations. Clinical Presentation • Clinical presentation is directly related to the degree of pulmonary stenosis. • Severe stenosis results in immediate cyanosis following birth. Mild stenosis will not present until later. • Growth is retarded – insufficient oxygen and nutrients • SOA on exertion “Tet Spell” • “Tet spells” at 23yo, child becomes cyanotic, may experience syncope Exams and Tests • CBC - hematocrit • ECG -RVH, RAD • CXR -boot shaped heart, right sided aortic arch • Echocardiogram -VSD Surgical Intervention 1 • Complete intracardiac repair of VSD and PA stenosis. • Enter chest through the sternum. Connect the heart and lung machine. Heart is stopped. • Repair the VSD with a patch. • Determine if PA needs to be removed or if removing the excessive muscle tissue will help to function correctly. • Pacemaker wires are placed temporarily because of the potential for postoperative ventricular arrhythmias. • Individual chamber pressures are then measured before the chest is closed. The pressure readings help to determine how effective the surgery was. • Complications: infective bacterial endocarditis, pulmonic regurgitation, arrhythmias, RBBB, or left anterior hemiblock Surgical Intervention 2 • New method for patching the VSD • Transcatheter patches were selected specifically for VSD size. Radio-opaque loop inside of each patch allowed for attachment of double nylon thread. Made retrieval possible if necessary. • Pts were anticoagulated with heparin initially, followed with ASA 24 hr later. • 48 hrs later the apparatus was inserted into the femoral vein were it was catherized until it reach the ascending aorta. • Echo was used to determine its location within the heart, allowing for proper placement of the patch for the VSD. • Pts were monitored in the ICU for 24 hrs. • Only 2 of the 16 pts in this study did not benefit from this study. In comparison to others, their VSD’s were much larger. • Pulmonary valvuloplastics were also performed. • Complications: there were no reported complications for VSD in this study Why Do We Need to Know? • Not every case of ToF will be discovered by cardiologist and pediatricians. • Some symptoms will be subtle and present later in life to PCPs. • Several case studies discussed patients who chose not to have their ToF corrected. We need to know if ToF defects are causing their health problem or if the problems are from other sources. References • • • • • • • • • American Heart Organization (AHO). “Tetralogy of Fallot.” 2005. Available online: http://www.americanheart.org/presenter.jhtml?identifier=11071 Greenberg, S. Bruce. “Tetralogy of Fallot.” 2004 Emedicine.com, Inc. Available online: http://www.emedicine.com/radio/topic685.htm Inova Heart and Vascular Institute. “Tetralogy of Fallot.” 2006. Available online: www.inova.org/inovapublic.srt/heart/pediatric_services/cardiac_surgery/tetralogy_of_fallot.html Moyano D., I C Huggon, L D Allan. “Fetal echocardiography in trisomy 18.” Originally published online 24 May 2005. Arch. Dis. Child. Fetal Neonatal Edition 2005; 90; pp. 520-522. Pflieger, Kurt. “Tetralogy of Fallot.” 2005 Emedicine.com, Inc. Available online: http://www.emedicine.com/emerg/topic575.htm Sideris, Eleftherios. “Transcatheter Patch Occlusion of Perimembranous Ventricular Septal Defects.” The American Journal of Cardiology; 95(12), 15 June 2005, 1518-1521. Warnes, Carole. “The Adult With Congenital Heart Disease.” Journal of the American College of Cardiology; 2005; 26(1): 1-8. Yang, X., L J Freeman and C Ross. “Unoperated Tetralogy of Fallot: case report of a natural survivor who died in his 73rd year; is it ever too late to operate?” Postgraduate Medical Journal 2005; 81; 133-134. Zeballos, Alvaro. “Tetralogy of Fallot.” 2003 Emedicine.com, Inc. Available online: http://www.emedicinehealth.com/fulltext/11205.htm