Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Coronary artery disease wikipedia , lookup
Artificial heart valve wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Rheumatic fever wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Aortic stenosis wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Cardiothoracic surgery wikipedia , lookup
Congenital heart defect wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
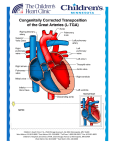
Dextro-Transposition of the great arteries wikipedia , lookup
NURSING CARE OF THE CHILD WITH A CARDIOVASCULAR DISEASE ASSESSMENT OF HEART DISORDERS IN CHILDREN • History • Physical assessment – general appearance – pulse, blood pressure, & respirations ASSESSMENT OF HEART DISORDERS IN CHILDREN • Diagnostic tests – – – – Electrocardiogram Radiography Echocardiography Phonocardiography & magnetic resonance imaging – Exercise testing – Laboratory tests CONGENITAL HEART DISEASE • Defects with increased pulmonary blood flow – Ventricular Septal Defect • Opening between ventricles • S/S – 4-8 weeks, fatigue and harsh murmur • Therapeutic management – Most close spontaneously, those that don’t require open heart surgery • Defects with increased pulmonary blood flow – Atrial Septal Defect • Opening between the atria • S/S – Murmur, second heart sound splitting • Management – Surgery – Patent Ductus Arteriosus • Fetal structure that should begin closing with the first breath and should complete by 3 months • S/S – Wide pulse pressure and continuous murmur • Management – Administration of indomethacin – Cardiac Catheterization – Surgery NURSING CARE OF THE CHILD WITH A HEART DISORDER • Obstructive defects – Pulmonic Stenosis • Narrowing of the pulmonary valve or artery causing the right ventricle to hypertrophy • S/S – Mild right sided heart failure – Cyanosis – SEM • Therapeutic Management – Balloon angioplasty to relieve the stenosis -Aortic Stenosis • Stenosis of the aortic valve prevents blood from passing from the left ventricle into the aorta, leading to hypertrophy of the left ventricle • S/S – Usually asymptomatic but with murmur – May have chest pain and even sudden death • Therapeutic Management – Stabilization with a Beta Blocker or Calcium Channel Blocker – Balloon valvuloplasty – Valve replacement – Coarctation of the Aorta • Narrowing of the lumen of the aorta • S/S – Absence of palpable femoral &/or brachial pulses; headache, vertigo, nosebleeds, CVA; leg pain • Therapeutic Management – Surgery or angiography • Defects with decreased pulmonary blood flow – Tricuspid Atresia • The tricuspid valve is closed, blood flows through the patent foramen ovale into the left atrium, bypassing the lungs. Then it is shunted back through a PDA into the lungs. When these structures close, cyanosis, tachycardia, and dyspnea occur. Surgery must correct. • Treatment: IV infusion of PGE until surgery • Defects with decreased pulmonary blood flow – Tetralogy of Fallot • Four anomalies – – – – Pulmonary stenosis VSD Dextroposition of the aorta Hypertrophy of right ventricle • S/S – Cyanosis – Polycythemia (increase in number of RBC) – Dyspnea, growth restriction, clubbing of fingers • Therapeutic Management – Surgery ACQUIRED HEART DISEASE • Congestive Heart Failure – S/S • Tachycardia, tachypnea • Right sided: increased venous pressure, hepatomegaly • Left sided: dyspnea, crackles (rales), cyanosis, and, eventually, ride sided failure – Therapeutic management • Reduce workload of the heart using diuretics, inotropics, and vasodilators • Rheumatic fever – S/S • Systolic murmur • Chorea (sudden involuntary movement of the limbs) • Macular rash on the trunk • Swollen and tender joints, SQ nodules on tendon sheaths • Positive ASO titer and increased ESR and C-reactive protein – Therapeutic management • Bedrest • Antibiotics to eliminate Group A Beta hemolytic Strept • Prognosis depends on how much heart involvement • Kawasaki disease – S/S (early) • High fever that doesn’t respond to therapy • Swollen hands and feet, enlarged joints • Strawberry tongue, red lips, conjunctiva • Enlarged cervical lymph nodes – S/S (late) • Skin desquamation • Platelet count increases • aneurysms – Therapeutic management • Administration of Ibuprofen for inflammation and platelet aggregation • IV immunoglobulin to decrease immune response • Most children recover fully but some will need heart surgery to repair damage