Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Presented at SPIE Medim, San Diego CA, February 2007
Determination of drill paths for percutaneous cochlear access
accounting for target positioning error
Jack H. Noble a, Frank M. Warrenb, Robert F. Labadiec, Benoit Dawant a,
and J. Michael Fitzpatrick a
a
Department of Electrical Engineering and Computer Science, Vanderbilt University,
Nashville, TN 37235, USA;
b
c
Division of Otolaryngology, University of Utah, Salt Lake City, UT 84132;
Department of Otolaryngology-Head and Neck Surgery, Vanderbilt University Medical Center,
Nashville, TN 37232, USA
ABSTRACT
In cochlear implant surgery an electrode array is permanently implanted to stimulate the auditory nerve and allow
deaf people to hear. Current surgical techniques require wide excavation of the mastoid region of the temporal bone
and one to three hours time to avoid damage to vital structures. Recently a far less invasive approach has been
proposed—percutaneous cochlear access, in which a single hole is drilled from skull surface to the cochlea. The drill
path is determined by attaching a fiducial system to the patient’s skull and then choosing, on a pre-operative CT, an
entry point and a target point. The drill is advanced to the target, the electrodes placed through the hole, and a
stimulator implanted at the surface of the skull. The major challenge is the determination of a safe and effective drill
path, which with high probability avoids specific vital structures—the facial nerve, the ossicles, and the external ear
canal—and arrives at the basal turn of the cochlea. These four features lie within a few millimeters of each other, the
drill is one millimeter in diameter, and errors in the determination of the target position are on the order of 0.5mm
root-mean square. Thus, path selection is both difficult and critical to the success of the surgery. This paper presents
a method for finding optimally safe and effective paths while accounting for target positioning error.
Keywords: Image-guided surgery, Monte Carlo, cochlear implant, percutaneous access
1. INTRODUCTION
Cochlear Implantation is a surgical procedure performed on individuals who experience profound to severe
sensorineural hearing loss, i.e. individuals who are deaf. In normal ears, sound waves propagate through the
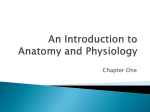
external ear to the ear drum. Vibrations are amplified by the malleus, incus, and stapes before causing a fluid wave
to travel in the inner ear, the cochlea (Figure 1). This fluid wave travels over many tiny hair cells. The bending of
these hair cells begins a complex molecular cascade which results in stimulation of the auditory nerve. The auditory
nerve innervates an area of the brain which allows one to hear. The natural ability to hear can be hindered by
damage to any of these structures. Cases involving less severe hearing loss are normally treated using hearing aids,
which amplify the sound waves that impinge on the ear drum. When damage becomes severe, cochlear implants are
the preferred treatment. More than 80,000 implants have been placed worldwide, including 60,000 in the United
States. Projections indicate that over 750,000 Americans with severe hearing loss may benefit from an implant [1].
In cochlear implant surgery, an electrode array is permanently implanted into the cochlea by threading the array
through the basal turn (Figure 1). The array is connected to a receiver mounted securely under the skin behind the
patient’s ear. When activated, the external processor senses sound, decomposes it (usually involving Fourier
analysis), and digitally reconstructs it before sending the signal through the skin to the internal receiver which then
1
Presented at SPIE Medim, San Diego CA, February 2007
Basal
Turn
Basal
Turn
(a)
(b)
Figure 1. Ear Anatomy. (a) Anatomy of the external, middle, and inner ear.
threaded through the Basal Turn of the cochlea.
(b) Implanted electrode array is
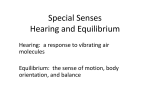
Figure 2. Percutaneous surgery fiducial system
activates the appropriate intracochlear electrodes causing stimulation of the auditory nerve and hearing. Current
methods of performing the surgery require wide excavation of the mastoid region of the temporal bone. The
precautionary measures necessary to safely avoid sensitive structures can prolong surgery time from one to three
hours. Recently another approach has been proposed—percutaneous cochlear access, in which a single hole is
drilled on a straight path from the skull surface to the cochlea [2,3].
Percutaneous access is accomplished by performing preoperative planning using CT imagery to create an
appropriate drill guide. Prior to surgery, anchors are affixed to the patient’s skull by creating three small skin
incisions and screwing self-tapping anchors into the bone. The incisions are stitched over the anchors, and a CT
image of the patient is acquired. Using the image, the physician is able to pick a safe direct drill path from the skin
surface to the cochlea. With the path and image information about anchor location, a drill guide unique to the
patient is rapid prototyped. In surgery, the drill guide is attached to the bone implanted anchors on the patient’s
skull. The drill is attached to the guide, which governs the path of the drill all the way to the cochlea (Figure 2).
This method of preoperative planning for drill guide construction was proven successful for Deep Brain Stimulators
(DBS) procedures [4].
Several key advantages make percutaneous cochlear access preferable over traditional methods. Percutaneous
access would prove to be a far less invasive surgery since a single hole is drilled to the cochlea rather than full
excavation of the mastoid region. Excavation is the most time consuming portion of the surgery since great care is
needed to expose and avoid sensitive structures. By averting excavation, surgery time can be reduced from the
current 2 to 3 hours down to as short as 30 minutes. Percutaneous access would standardize and simplify the
surgical technique which could allow more surgeons ability to perform the surgery. Currently, patients must wait 1-
2
Presented at SPIE Medim, San Diego CA, February 2007
Ossicles
Ossicles
External Ear
Canal Wall
Facial Nerve
Ossicles
Facial Nerve
Facial Recess
Drill Path
Drill Path
External Ear
Canal Wall
External Ear
Canal Wall
Facial Nerve
2mm
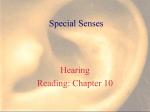
Figure 3. CT of left ear. Ossicles, external ear canal wall, facial nerve, facial recess, and drill path.
(Left) Sagittal view. (Middle) Axial view. (Right) Coronal view.
Basal Turn
Basal Turn
Drill Path
Round
Window
Drill Path
Round
Window
2mm
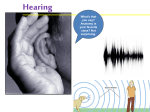
Figure 4. CT of left ear. Basal turn of cochlea, round window, and drill path (Left) Axial.
Coronal.
(Right)
3 weeks for activation as swelling from the open-field surgery is resolved. With a percutaneous approach, swelling
no longer becomes an issue and activation can occur on the same day as surgery.
Percutaneous access can become a preferred solution only if the method proves to be at least as safe and reliable
as current surgical methods. To determine whether the proposed system can meet this criterion, the meaning of a
safe and reliable method must first be defined. A safe cochlear implant drilling procedure can be simply defined as
a procedure in which access to the cochlea via the preferred target point (the basal turn of the cochlea) is achieved
while avoiding nearby vital anatomy (the facial nerve, the external ear canal, and the ossicles). The facial nerve is a
highly sensitive structure that controls all movement of the ipsilateral face. If damaged, this may lead to temporary
and/or permanent facial paralysis. Violation of the external auditory canal can lead to a breech in sterility and open
a potential avenue for future infection with possible implant extrusion. While injury to the ossicles is not
catastrophic -- implanted patients are already deaf -- in the future implants will most likely involve individuals with
residual hearing where violation of the ossicles would be discouraged. Thus we have included the ossicles as vital,
adjacent structures.
In a typical cochlear implant surgery, the target point is the basal turn of the cochlea via the round window
(Figure 4). The actual entry point is the surface of the skull. However, as adjacent vital anatomy occurs
approximately 2cm deep from the surface of the skull to the level of the facial nerve, a deeper entry region is the true
constraint (i.e. it does not matter where the lateral skull is entered as long as this deeper region's boundaries are not
transgressed). This region is termed the facial recess and is bordered by the facial nerve, the medial aspect of the
3
Presented at SPIE Medim, San Diego CA, February 2007
Facial Nerve
Ossicles
Facial
Recess
Round
Window
Round
Window
(a)
Ossicles
Drill Path
Cochlea
Facial
Recess
Facial Nerve
Drill Path
External Ear
Canal Wall
(b)
(c)
External Ear
Canal Wall
(d)
Cochlea
Figure 5. 3D rendering of the structures of the left ear. Drill path is 1.0mm diameter. (a) View along drill
path. The facial recess region is approximately the same depth as the facial nerve. The round window
directly precedes the basal turn of the cochlea. (b) Left-to-right view.
(c) Left-to-right, anterior-toposterior view. (d) Posterior-to-anterior view.
external auditory canal, and the body of one of the ossicles, the incus. The drill path is thus constrained to pass
through the facial recess and hit the target, the basal turn of the cochlea. Thus, the entry point of the surface of the
skull can be determined by extending this drill path laterally. When looking through the facial recess to the cochlea
along the preferred drilling trajectory, it can be seen that the structures we wish to avoid create a window
approximately 3.5mm in diameter through which a safe path to the cochlea can be planned (Figure 5a).
Currently, the major problems with the proposed method of percutaneous cochlear access are the various
sources of error. Data from the DBS project suggests that there is a Root Mean Squared (RMS) Target Registration
Error (TRE) [5] in the drill guide system of 0.5mm at the distance from the surface of the skull to the cochlea, with a
pessimistic estimation of 0.8mm RMS. A value of 0.8mm RMS would be a safe estimation of error if there were no
arbitrary nature in how the physician chooses the appropriate path in the preoperative CT. Choosing a path to avoid
three-dimensional structures by examining a volume of two dimensional images has proved to be quite difficult,
even for experienced physicians. There are difficulties in repeatability as well as true safety in avoiding sensitive
structures. While finding a line segment through the facial recess to the cochlea that avoids sensitive structures is
not so difficult, manually choosing a safe line segment that accounts for the 1.0mm diameter of the surgical drill
burr as well as the 0.8mm RMS error in the drill guide system is highly difficult, if not impossible, to do manually.
A method of automatic drill path computation was proposed in [6], but that method did not account for TRE. In this
paper we present a method of automatic computation of the degree of safety of any arbitrary drill path as well as an
automatic search algorithm to plan a probabilistically safe drill trajectory for access to the cochlea.
2. METHODS
2.1 Initial Information
Our method to determine the probabilistic safety of a given drill path assumes that some information is given. It
is necessary to have a drill path target point, a drill path entry point search space, and all sensitive structures defined
and represented as segmented isosurfaces in the patient image, which is a CT volume. It is also necessary to know a
point along the drill path line that can be specified with negligible error and a point on the line that experiences
normally distributed error with a known standard deviation. The drill burr must have a known radius.
2.2 Detecting Surface Contact
In order to determine whether a given path will cause the drill burr to contact a sensitive structure, we first need
to be able to calculate the closest distance between the planned path and the surface of the structure. Suppose there
is a drill path line L which passes through entry point pe and target point pt. Any point m on the line L can be
represented as
4
Presented at SPIE Medim, San Diego CA, February 2007
m pe xaˆ ,
(1)
where
p p
e
aˆ t
pt pe
,
(2)
and x is some scalar. Suppose now that we have a triangulated surface S that is composed of Mt triangles. Triangle
TS(p) is the pth triangle on surface S. The edges of TS(p) comprise three line segments. Assume that line L does not
pass through triangle TS(p). This assumption will be explained later. It is easy to see that unless L is parallel to the
face of TS(p), the closest point on triangle TS(p) to line L will always lie of one of the three edges of TS(p). In the case
in which line L is parallel to the face of triangle TS(p), it is possible to have infinitely many closest points in TS(p).
These closest points cross the face of TS(p) as a line segment parallel to line L. All points along that segment are of
equal distance to line L. When the goal is to find any one position in triangle TS(p) at which TS(p) is closest to line L,
suitable closest points still exist on the line segment edges of TS(p). It is reasonable then to simplify the calculation of
the closest distance between triangle TS(p) and line L by calculating only the closest distance from the line segment
edges of TS(p) to line L.
The Mt triangles on surface S are composed of Ml line segments. The set of all line segments that define S can
be represented by two sets of vertices v1 and v2, where one endpoint of segment S(i) is v1(i), the other endpoint is v2(i),
and S(i) is the ith line segment in S. Any point q(i) along the line segment S(i) can be represented similarly to Eq. (1)
as
(3)
q(i ) v(i ) y (i ) bˆ(i ) ,
1
where
(i ) (i )
v v1
bˆ(i ) 2
v (i ) v (i )
1
2
,
(4)
and y(i) is some scalar bounded by
0 y (i ) v2(i ) v1(i )
(5)
.
There exists a point qc(i) on segment S(i) and another point mc(i) on line L such that the distance from qc(i) to mc(i) is the
shortest distance dmin(i) between line L and segment S(i). Closest point calculations are shown in the appendix,
Section 6.1. Assuming that the maximum length of all line segments that compose triangulated surface S is small
relative to the probable closest distance of L to surface S (that is, as long as the surface triangulation is precise
enough to realistically model the surface), the closest distance D from line L to surface S can be reasonably
estimated by
(i )
D dist S , L min i d min
,
(6)
where mini represents the minimum over all i line segments on surface S, and dmin(i) is calculated as in Section 6.1.
D is defined in Eq. (6) based on the premise that the closest portion of any triangle on surface S to line L is
approximately equal to the closest distance between the real surface represented by S and line L.
Determining whether the drill burr along line L will hit surface S can now easily be defined by the following
criterion. For any given path L, if D is greater than the radius of the drill burr, then the burr following line L will
miss surface S. If D is less than the radius of the drill burr, then the drill burr will hit S.
Our original assumption that L does not pass through triangle TS(p) will not be true if L actually passes through S.
This case can be ignored as long as the radius of the drill burr is much larger than the longest line segment
5
Presented at SPIE Medim, San Diego CA, February 2007
composing surface S. Under this condition D should be equal to zero but will actually be estimated to have value
greater than zero when line L passes through surface S. However, because the line segments of each triangle in S are
constrained to be small compared to the radius of the drill burr, the estimated distance D when L passes through
surface S will be much less than the radius of the burr. According to our previously defined criterion, the drill burr
on line L will still hit S. Therefore, because we are interested in determining whether the drill burr on L hits surface
S and not interested in finding the true distance between L and S, nothing is lost by ignoring this case.
2.3 Safety Calculation
With a method of calculating a ‘hit’ or ‘miss’ for any given drill trajectory, a safety probability model can be
constructed using a Monte Carlo method. A normally distributed pseudo-random number generator can be used to
create a [N x 1] sized vector rσ such that σ is the expected RMS magnitude of the vector and N is the number of
dimensions of the space of the vector. If rξ(j) is the random number giving the jth component of the vector rσ with
standard deviation ξ, then
N
(7)
For 3D space with N=3 and σ = 0.8mm, ξ is approximately 0.5mm. We generate rσ and use it to displace the
trajectory at the site of the selected target position pt by simple addition so that it is displaced to pt’ = pt + rσ. By
replacing target point pt with displaced point pt’ in Section 2.2 calculations, a ‘hit’ or ‘miss’ can be determined for
the displaced path. If a ‘hit’ or ‘miss’ is recorded iteratively, each iteration using a new random displacement rσ, a
large set of hits or misses can be collected. Given a large enough number of iterations, the probability that the
original drill path can successfully avoid damage to a particular surface, Ps, can be approximated by
Ps
n misses
n
misses
nhits
(8)
where nmisses denotes the number of misses over all iterations and nhits is defined similarly. Ps is the quantified
measure of safety that path L will not damage structure S.
2.4 Safe Path Search
The drill path line is defined as the line that includes the skull entry point pe and round window target point pt.
In the search for a safe path, the path is varied by changing pe and thus the path can be labeled by pe. The safe path
search determines the safety of a set of drill paths {pe} defined within a designated search space, employing a safety
calculation for each path by repeatedly displacing pt by rσ to simulate error in the specification of the target position.
For this application we limit the search space to include only drill paths that pass through the facial recess region. In
accordance with this search space, the drill path line will in practice be defined as the line L that passes through
facial recess point pfr and target point pt. It follows that for any given pfr and pt, there is a corresponding pe along
line L positioned at the surface of the skull. Passing an entry point pe that corresponds to a particular pfr through Eq.
(1) and performing distance and safety calculations in Section 2.2 and 2.3 will yield the probability Ps that the drill
path along line L defined by pfr, or equivalently by the corresponding pe, will successfully avoid damaging structure
S.
Values for pfr are chosen over a 2D bounding box defined by the facial recess. The box passes through the
center of mass of the 3D facial recess region and is normal to the line that passes through the round window target
and center of mass of the facial recess. This is simply a method of defining the search window to be perpendicular
to a roughly estimated, safe drill-path line. Confining the search to a bounding box in this manner allows any path
that passes through the facial recess region to be included in the search while simplifying the search space to two
dimensions. The algorithm finds the degree of safety in avoiding each sensitive structure associated with any pfr in
the search space. Each probability of safety Ps is passed into a cost function that assigns the entry point a scalar
value c representing its desirability. For any given entry point k in the search space the cost function is defined as
6
Presented at SPIE Medim, San Diego CA, February 2007
P P
c( k ) Ps( k )
b1
(k )
s2
1
b2
(k )
s3
b3
,
(9)
where s1, s2, and s3 denote the facial nerve, external ear canal, and ossicles surfaces, and exponents b1, b2, and b3
denote constant coefficients used to weight each surface with a relative safety importance. Note that the formula in
Eq. (9) does not represent a probability, but is simply a way to combine three probabilities into one scalar value that
can be optimized by some searching method.
Values for exponents b1, b2, and b3 may be derived using any appropriate method. In this application we derive
these exponents based on goals for safety for each structure established by an experienced surgeon. A planned path
is deemed acceptable if the path’s probability of safety for each particular structure meets the particular goals for
safety set for those structures. To account for these goals in the cost function, b1, b2, and b3 are chosen such that
each of the probability factors contributes approximately equally to the cost function in the vicinity of the goals.
Approximate equality is achieved by choosing values of b1, b2, and b3 such that
Gn
bn
so that
bn
Gm m ,
b
log Gsm
bm
,
(10)
(11)
log Gsn
where n denotes the nth surface, m denotes the mth surface such that m is any surface other than n, G is the goal for
safety of a particular surface, and b is an exponent in the cost function.
Any searching method can be employed to find a path that is at least locally optimal, but because of the
irregular patterns that can emerge in the spatial variation of c(k) across different patients resulting from the
differences in inter-patient anatomy for this application, we choose to implement an coarse-to-fine exhaustive
searching method.
3. RESULTS
3.1 Parameter Definition
All evaluations were performed in Matlab (Mathworks, Natick, MA). All experiments were performed using
identical parameters. For the segmentation of the critical structures, fully automatic methods were implemented
using an atlas-based strategy as presented in [6] combined with simple edge detection and intensity uniformity
criterion. For the drill-path error, the point of drill contact to the surface of the skull pe is treated as the error-free
position, because it is so close to the drill guide that its error is negligible, while the round window target at the basal
turn of the cochlea pt is treated as the point on the line that experiences targeting error. Goals for safety were
decided to be probabilities of at least 0.999, 0.950, and 0.670 for avoiding damage to the facial nerve, external ear
canal wall, and ossicles, respectively. Exponent b2 was arbitrarily set to 1, and exponents b1 and b3 were calculated
using Eq. (11) to be 51.27 and 0.13. A simple fail-safe measure was also implemented to ensure that Ps1 is always
greater than 0.999, since safety of the facial nerve is of utmost concern. The drill burr used for the proposed surgery
has a radius of 0.5mm, and a pessimistic RMS error of 0.8mm is assumed. A complete search requires 15 to 20
minutes on a 3 GHz PC (Microsoft Windows XP).
3.2 Experimental Results
Experiments were conducted using patient CT scans of three left and eight right normal ears. Experiments
followed Institutional Review Board approved protocols. The algorithm achieved a fully automated determination of
7
Presented at SPIE Medim, San Diego CA, February 2007
Probability of Safety
Goals
Patient
1
1
2
2
3
4
5
6
7
8
9
Ear
L
R
L
R
L
R
R
R
R
R
R
Facial Nerve
External Ear
Canal Wall
Ossicles
0.999
0.95
0.67
1.0000
1.0000
0.9998
0.9992
0.9990
1.0000
0.9994
0.9996
0.9992
1.0000
0.9994
1.000
0.998
0.987
0.915
0.826
0.999
0.946
0.989
0.923
0.998
1.000
0.974
0.976
0.994
0.992
0.995
0.994
0.907
0.925
0.970
0.999
0.984
Table 1. Experimental results for automatically planned drill paths. Facial nerve values are precise to 4
decimals. All other values are precise to 3 decimals. Planned paths constrained to have facial nerve
probability of safety greater than 0.999.
(a)
(b)
(c)
(d)
Figure 6. Automatically determined drill paths. Paths match the diameter of the drill burr at 1.0mm.
Anatomy is identical to Figure 5. (a) Patient 1, left ear. (b) Patient 2, left ear. (c) Patient 4, right ear.
(d) Patient 6, right ear.
drill paths for each patient. Very positive results can be seen for most of the experimental trials shown in Table
1The estimations of safety for the automatically planned path with respect to the facial nerve were calculated by
5000 trials of randomly displaced paths as described in Section 2.2 (Table 1). Safety estimations for the external ear
canal wall and ossicles were calculated by 1000 trials. Several probabilities of 1.00 are listed in the table. While in
reality this is clearly impossible, those paths endured all trials without hitting the relevant structure. Given our
methodology those probabilities of safety are approximately 1.00. The numbers in bold in the external ear canal
wall safety column of Table 1 indicate that the probability of safety is below the threshold level. For these patients,
percutaneous cochlear access may not be the preferred treatment and traditional cochlear access techniques might be
recommended. For all seven other ears, percutaneous access appears to be a very promising surgical method. The
lowest facial nerve safety estimation of 0.999 successfully meets the threshold level of safety of 0.999. The lowest
ossicles safety estimation of 0.853 is well above the ossicles safety threshold of 0.67. Several examples of
automatically generated paths are shown in Figure 6. Although precise safety estimations are difficult to determine
with the human eye, all generated drill paths appear visually to be reasonable and safe solutions.
4. CONCLUSIONS
These results suggest that percutaneous cochlear access may be a viable alternative to traditional surgical
methods for placing cochlear implants. With the current estimation of TRE at the entrance to the cochlea, manual
determination of drill paths is prone to high variability in safety. Using the method presented in this paper, however,
safe paths can be automatically determined with reasonable consistency. Unlike choosing paths manually in a CT,
the automatic method accounts for measured TRE, estimates the relative safety of any path in statistical terms, and
8
Presented at SPIE Medim, San Diego CA, February 2007
indicates whether percutaneous access may be preferable to traditional methods for a specific patient. The results of
this paper have demonstrated that the suggested method of percutaneous cochlear access may not be viable for all
patients for a given TRE level, and therefore this paper has also demonstrated the need for error estimation to safely
perform percutaneous cochlear implant surgery. While automatic path determination appears to be feasible from
this small study, future investigations will be pursued involving a manual physician interface that allows the
physician to alter an automatically generated path and provides feedback to the physician involving the estimated
probability of safety of each sensitive structure given a chosen path.
5. ACKNOWLEDGEMENTS
This work has been supported in part by the Vanderbilt Undergraduate Summer Research Program (VUSRP) by
Vanderbilt University. We would like to thank Dr. Bobby Bodenheimer and Christian de Juan of the Vanderbilt
Department of Electrical Engineering and Computer Science for help with surface triangulations.
6. APPENDIX
6.1 Solution for Points of Closest Distance between a Line and Line Segment
Given a drill path line L containing points pe and pt, any point m on the line L can be represented using Eqs. (1)
and (2). The ith line segment on surface S is described by its vertices v1(i) and v2(i). Any point q(i) on segment S(i) can
be represented using Eqs. (3) and (4), and Inequality (5). With this representation, the problem becomes finding
scalar values x and y such that points m and q(i) are as close as possible. For such x and y, m is the closest point on
line L to S(i), and q(i) is the closest point on S(i) to line L. The function that describes the distance d between m and
q(i) is simply
(12)
d m q(i ) p v(i ) xaˆ ybˆ .
e
1
Since d is minimum at the minimum distance between L and S(i), the solution for x and y can be found where the
derivative of d 2 is equal to zero with respect to x and y. That is
p
d2
e
v1(i )
2
x
and
d2
y
pe v1(i )
2
i
x 2 y 2 2 xaˆ 2 ybˆ pe v1 2 xy bˆ aˆ
0 ,
x
i
x 2 y 2 2 xaˆ 2 ybˆ pe v1 2 xy bˆ aˆ
0 .
y
(13)
(14)
Carrying out the derivatives in Eqs. (13) and (14) yields,
x aˆ pe v1(i ) y bˆ aˆ 0
and y bˆ pe v1(i ) x bˆ aˆ 0 .
(15)
Solving for x and y yields
p
x
e
1 bˆ aˆ
v1(i ) bˆ bˆ aˆ aˆ
2
v
y
(i )
1
and
1 bˆ aˆ
pe aˆ bˆ aˆ bˆ
2
9
if Eq. (5) is preserved and bˆ aˆ 1 ,
(16)
Presented at SPIE Medim, San Diego CA, February 2007
In the case where bˆ aˆ 1 , line L and segment S(i) are parallel. Under this condition Eq. (16) cannot be solved
because there are infinitely many closest points on L and S(i). To preserve Inequality (5), y can arbitrarily be chosen
to equal 0 since all points on segment S(i) are closest points. If y in Eq. (16) is such that y is outside the range of
Inequality (5) then y describes a collinear point to segment S(i) that is out of the range of that segment. Therefore, if
y<0 the closest point on S(i) to L is at y=0. In that case, when we solve for x, we have q(i) = v1(i) so that
d m v1(i ) pe v1(i ) xaˆ
(17)
and
d2
x
so
y 0,
pe v1(i )
x aˆ pe v1(i )
2
x 2 2 xaˆ pe v1(i )
0 ,
x
if
y< 0 in Eq. (16)
or
(18)
bˆ aˆ 1 .
(19)
(i )
(i )
(i )
(i )
If y found using Eq. (16) is such that y v2 v1 , the closest point on S(i) to L is at y v2 v1 so that q(i)=v2(i).
Solving for x can be done in the same fashion as Eqs. (17),(18), and (19) by substituting v2(i) for v1(i) so that
y v2(i ) v1(i ) ,
x aˆ pe v2(i )
y v2(i ) v1(i )
if
in Eq. (16).
(20)
Once the coefficients x and y have been determined using Eqs. (16), (19), and (20), the closest distance dmin from S(i)
to line L is very simply
dmin m q(i )
,
(21)
Where m and q(i) are defined as in Eqs. (1) and (3) using coefficients x and y.
7. REFERENCES
1.
2.
3.
4.
5.
6.
Mohr PE, Feldman JJ, Dunbar JL, McConky-Robbins A, Niparko JK, Rittenhouse Rk, and Skinner MW. “The
societal costs of severe to profound hearing loss in the United States,” Int. J. Technol. Assess. Health Care
16(4), 1120-1135, 2000.
Labadie RF, Choudhury P, Cetinkaya E, Balachandran R, Haynes DS, Fenlon M, Juscyzk S, Fitzpatrick JM,
“Minimally-Invasive, Image-Guided, Facial-Recess Approach to the Middle Ear: Demonstration of the
Concept of Percutaneous Cochlear Access In-Vitro,” Otol. Neurotol. 26, 557-562, 2005.
Warren FM, Labadie RF, Balachandran R, Fitzpatrick JM. “Percutaneous Cochlear Access Using BoneMounted, Customized Drill Guides: Demonstration of Concept In-Vitro,” Mtg. Am. Otologic Soc., Chicago,
IL, May 2006.
Fitzpatrick JM, Konrad PE, Nickele C, Cetinkaya E, Kao C, “Accuracy of customized miniature stereotactic
platforms”, Stereotactic and Functional Neurosurgery, 83, 25-31, April 2005.
Fitzpatrick JM, West JB, Maurer CR Jr., “Predicting error in rigid-body, point-based image registration”, IEEE
Transactions on Medical Imaging 17, 694–702, Oct 1998.
Al-Marzouqi H, “Automatic planning of a safe drilling path to be used in cochlear implantation surgery using
image registration techniques”, MS Thesis, EECS Department, Vanderbilt University, 2006.
10