Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
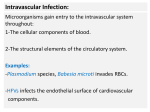
Plasmodium falciparum wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Marburg virus disease wikipedia , lookup
Staphylococcus aureus wikipedia , lookup
West Nile fever wikipedia , lookup
Leptospirosis wikipedia , lookup
Sarcocystis wikipedia , lookup
Brucellosis wikipedia , lookup
Trichinosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Hepatitis B wikipedia , lookup
Oesophagostomum wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Neonatal infection wikipedia , lookup
Anaerobic infection wikipedia , lookup
Gülden Çelik Learning Objectives At the end of this lecture, the student should be able to: Define bacteremia, fungemia, and sepsis List the main types of bacteremia and reasons List the main microorganisms causing bacteremia List the main laboratory method for detection List the important factors influencing the laboratory test result Bacteremia • Presence of viable bacteria in the blood • May be transient • Self-limited without clinical consequences But: • Frequently reflects the presence of serious infections • Life-threatening in immunocompromised • Often associated with hospitalization and instrumentation Pseudobacteremia • As a result of contamination of blood samples during phlebotomy • False positive results of blood culture • Contamination is due to skin commensals: coagulasenegative staphylococci(CoNS) or other skin flora But: • Depending on the clinical situation these skin flora may not represent pseudobacteremia Occult(unsuspected)bacteremia No physical sign s or symptoms of severe infection Frequently in children younger than 2 years Due to Streptococcus pneumoniae Diagnosis may be overlooked If treatment delayed, catastrophic sequences Sepsis In the past septisemia :bacteremia+bacterial invasion and toxin production Now terms are used to explain systemic response to infection according to the severity: Systemic inflammatory response syndrome(SIRS) Septic shock Multiple organ dysfunction syndrome (MODS) %70 septic patients Blood culture negative Clasification of bacteremia Site of origin: Primary bacteremia: Arises from endovascular source such as infected cardiac valve or infected intraveneous catheter Secondary bacteremia: Arises from infected extravasular source such as lung in patient with pneumonia Bacteremia of unknown origin Clasification of microbiology Gram-positive Gram-negative polymicrobial CoNS bacteremia In hospitalized patient Indwelling vascular device Polymicrobial bacteremia Enterococci and gram-negative microorganisms: invasion from bowel perforation Clasification of place of acquisition Community acquired Nosocomial : resistant strains Clasification of duration Transient: dental, colonoscopic procedures Intermittant: meningecoccemia Continuous: infective endocarditis Bacteremic patients Incidence of septic shock %10-30 Mortality of septic shock:%40-50 Risk for bacteremia Decreased immune competency of selected patients Increased use of invasive procedures Age of the patient Administration of drug therapy Microbiology Over the last 25 years patterns of organisms has shifted: 1960s-1970s: gram-negatives E.coli,P. Aeruginosa 1980s-1990s:gram-positives: S. aureus, CoNS, enterococcus More recently:Fungi(Candida) Fungemia: antifungal susceptibility test Microbiology Methicillin-resistant S. aureus(MRSA) Vancomycin-resistant enterococci(VRE) Extended-spektrum Beta-lactamases (ESBL) producing gram-negatives Haemophilus influenzae b (Hib)decreased by %95 by conjugate Hib vaccine Clinical syndomes associated with bacteremia • Catheter-related bloodstream infection • Urinary tract infection • Pneumonia • Intraabdominal infection • Skin infection • Infective endocarditis • Musculoskeletal infection • Central nervous system infection Laboratory diagnosis Hemoculture(Venous blood ! : in sterile conditions)) Density of bacteremia in adults versus neonates: 10-15 bacteria/ml is detected by the blood culture Newborns have higher numbers of microorganisms Laboratory diagnosis Hemoculture(Venous blood ! : in sterile conditions)) Density of bacteremia in adults versus neonates: 10-15 bacteria/ml is detected by the blood culture Newborns have higher numbers of microorganisms Rapid molecular techniques: NAT(nucleic acid amplification techniques) Laboratory diagnosis Hemoculture (volume!) Density of bacteremia in adults versus neonates: Age Amount ≤9 yıl 1 ml per year ≥10 yıl 20ml Laboratory diagnosis Hemoculture Frequency of collection(!) Three sets One set: 1 aerobic one anaerobic Just before fever rises(!) Laboratory diagnosis 1.set:%80 2.set:%90 3.set:%99 -In the first 1-2 hours from three different veins 3 sets -In subacute bacterial endocarditis: in the first 24 hours three sets 1 hour in between sampling -Bacteremia of unknown origin: in 48 hours 4-6 times 10ml Laboratory diagnosis Brucellosis During the initial presentation and at the anticipated temperature spike Blood culture methods Blood culture systems 7 days of incubation Bacterial endocarditis and fungemia: 2weeks Brucellosis:21-28 days subcultured weekly Anaerobic subculture is performed after 2 days Any presumptive positive finding should be reported to the physician by phone(panic values in laboratory). Source of contamination %2 -3 Staphylococcus epidermidis Micrococcus Diphtheroids Propionibacterium acnes Any organism cultured from 2-3 blood cultures should not be overlooked as contaminant Source of contamination Microbiologists can not make this determination(true pathogen or contaminant) in the laboratory: Physician input and patient history is needed. Prevention: Hemoculture : education of nurses for sampling ! HEMOCULTURE (BLOOD CULTURE) Upon opening the bottle if it’s contaminated Disinfect the rubber cap with alcohol swab. Let it dry at least 30 seconds. the puncture site antisepsis