Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
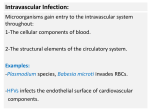
Intravascular Infection: Microorganisms gain entry to the intravascular system throughout: 1-The cellular components of blood. 2-The structural elements of the circulatory system. Examples: -Plasmodium species, Babesia microti invades RBCs. -HFVs infects the endothelial surface of cardiovascular components. Definitions: Endarteritis: intravascular infection of artery. It is associated with: 1-Congenital arterial anomaly; ductus arteriosus. 2-Diseased arterial endothelium; atherosclerotic plaques. Phlebitis: infection of the lumen of vein ; It is directly correlated with: 1-Direct spread from an adjacent focus of infection. 2-Intravascular foreign bodies (catheter) implanted in vein. N Infective Endocarditis: -Is an infection of the endocardial surface of the heart. -It is localized on the cardiac valves, the atrial or ventricular wall ,and the chordae tendineae. -Arise as a consequence of cardiac surgery or intra-cardiac instrumentation, and bacteremia. Classification of Endocarditis: 1-Infective. 2-Non-Infective. Or: 1-Acute: febrile , toxic illness lasting only days to several weeks. 2-Subacute: lower fever, anorexia, weakness, weight loss, and are symptomatic for longer than several weeks. Epidemiology: -Infective endocarditis accounts for 1 in 1000 admissions to large general hospitals. -More than 50% of cases involve people older than 50 years of age. N The common predisposing factors for endocarditis are: 1-Congenital cardiac defects: -Bicuspid aortic valves, ductus arteriosus, or ventricular septal defects. 2-Degenerative valvular diseases. 3-Acute Rheumatic fever: Streptococcal M protein Cross-reactivity with cardiac myosin. 4-Prosthetic heart valves. 5- Cardiac rhythm management device (CRMD). n Causes of Infective endocarditis: -Left sided endocarditis are most common, accounting for 95% of cases. -Right sided endocarditis accounts only for 5% of cases. Causes of endocarditis: 1-Native valve endocarditis: A-Acute : Staphylococcus aureus accounts for 60% of cases. 40% include alpha-Streptococcus and G-ve bacilli. Average mortality rate is 20%. Higher in patients over 65 years of age. N B-Subacute: -Alpha-Streptococci and non-hemolytic accounts for 60%. -40% include Enterococcus, Coagulase negative Staphylococcus species, fastidious Gram negative bacilli. -Among injection drug users (younger persons): -Staphylococcus aureus causes 75% of right-sided endocarditis. -Whereas a wide range of microbes cause left-sided endocarditis; 25% Staph aureus, 40% Streptococci and Enterococci, 18% fungi and Gram negative bacilli. N 2-Prosthetic valve endocarditis: Depends on the time after surgery when infection becomes symptomatic. A-Nosocomial acquired endocarditis: -50% of cases caused by Staphylococcus aureus. -Gram negative, Corynebacterium, and fungi. B-Community acquired endocarditis: -It occurs as a consequence of bacteremia. -It is acquired in the first year after valve replacement. -Staphylococcus aureus, Staphylococcus epidermidis (Beta-lactam resistance), and Streptococci. Pathogenesis and Microbial virulence factors: -Only a limited types of bacteria can cause endocarditis. -Microbial invasion into bloodstream (bacteremia). Microbial agents (Bacteremia) Host defense Thrombotic Vegetation Endothelium adhesion, Bacterial Vegetation Plasma Proteins Coagulation factors N -Microbes reach the cardiac valve. -Microbes resist complement-mediated bactericidal activity and escape phagocytosis. -Primary damage of valve endothelium; cytokines; expression of Beta1 integrin by endothelium; binding of plasma fibronectin ; coagulation and formation of sterile vegetation (Platelet-fibrin aggregates); (non-bacterial thrombotic vegetation). N -Increased microbial adhesion; -Alpha-hemolytic Strpetococci species produce extracellular dextran and Fim A adhesin that bind strongly to fibronectin and thrombotic vegetation. -Enterococci lipoteichoic acid promotes similar adhesion. -Staphylococcus aureus fibrinogen binding protein initiate the microbial adherence to thrombotic vegetation. -Formation of bacterial vegetation (108 to 109 CFU/gm). N -Colonization of heart endocardium due to: 1-Endothelium tissue factors; formation of thrombin. 2-Destruction of endothelial cells by thrombocidins. -Bacterial vegetation occurs along the edges of the heart valves, on the ventricular side of mitral and aortic valve and on the atrial side of tricuspid valve. N Microscopically, Bacterial vegetation is a mass of platelets, fibrin, Micro-colonies of microbes, and inflammatory cells. In the subacute form of infective endocarditis, the vegetation also include: a center of granulomatous tissue, which may undergo fibrosis (collagen) or calcification. N -In 25-35% of cases, Infective endocarditis is associated with fragmentation of vegetation into the circulation, causing peripheral septic emboli. -Visceral organs and brain involvement. -Continuous bacteremia. -Formation of antibodies complexes; serum sickness disease (focal embolic glomerulonephritis). Diagnosis of infective Endocarditis: Direct : Microbiology: 1- Blood culture results have a 95% sensitivity. 2-Surgically removed vegetation analysis by culture and PCR. Indirect: Serology: -Serologic testing have led to identification of : Rickettsia species, Coxiella species, and Bartonella as infrequent but important causes of subacute endocarditis. Non-infective Endocarditis: This form occurs more often in patients with Lupus erythematosus and is thought to be due to the deposition of immune complexes. These immune complexes form small sterile vegetation. Bacteremia: Bacteremia is the invasion of bloodstream by bacteria. The blood is normally a sterile environment, so the detection of bacteria in the blood is always abnormal. Bacteria can enter the bloodstream as a severe complication of mucosal surfaces colonization or surgical procedures: 1-Dental extraction. 2-Gingival surgery. 3-Air way infection. 4-GIT, UTI (endoscopy, catheter) Septicemia: Septicemia (sepsis) : is the invasion of bloodstream by virulent microbe and its toxins which results in acute systemic illness. Septic shock: is a medical emergency caused by decreased blood flow and oxygen delivery to organs and tissues as a result of inflammatory response against blood sepsis. It can cause multiple organ dysfunction syndrome and death. N -The mortality rate from septic shock is approximately 25%50%. Microbial virulence and pathogenesis (Sepsis and septic shock): -The Gram negative lipopolysaccharide bind to LPS-binding protein which crosslink CD14 in blood. -Blood monocyte, and neutrophils discriminate the complexes by CD14 receptors. -Lipopolysaccharide is a polyclonal B lymphocyte activator. N -Production of cytokines in bloodstream; (IL-1, IL-8, IL-12, TNF). -Systemic Vasodilation of capillary endothelium, and Vasoconstriction in the vasculature; edema and chemotaxis. -Decreased blood pressure, increased smooth muscle contraction of respiratory tract. -Rapid breathing, low blood pressure, fever, and lethal shock. Sources of Bacteremia: In the hospital, indwelling catheters are a frequent cause of bacteremia, because they provide a means by which bacteria normally found on the skin can enter the bloodstream. Other sources of bacteremia include: Dental procedures ,Urinary tract infection, Respiratory tract infection, GIT infection, intravenous drug use, Contaminated endoscopy or colonoscopy, Post-operative infection. Causes of Bacteremia and Sepsis: 1-Gastrointestinal infection: Typhoid fever (Salmonellosis), Malta fever (Brucellosis), Yersinia infection and Bacteroid fragilis. 2-Genitourinary tract infection: Staphylococcus aureus, E.coli, Klebsiella, Citrobacter, Enterobacter, and Pseudomonus species. Treponema pallidum, and Neisseria gonorrheae. N 3-Respiratory tract infection: Neisseria meningitidis, H. influenza, Streptococcus pneumoniae, MRSA, VRE, and Klebsella pneumonia. Diagnosis of endocarditis and Bacteremia: Blood culture: A- a 5-8 ml blood should be extracted for culture. B- Specimens should be extracted during fever stage. C- Inoculation of blood culture bottle, and incubation under aerobic and anaerobic conditions at 37C for up to 8 days. Blood culture procedure: N Blood culture growth indicators: 1-Turbidity of blood culture media. 2-Air bubbles formation in the media. 3-Hemolysis of cultivated blood. Identification of pyogenic Cocci isolated from Blood culture: n Staphylococcus species: DNase postive Staphylococcus aureus Coagulase positive N Streptococcus viridans species are resistant to Optichin and insoluble in bile salt.