Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
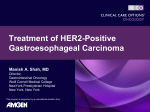
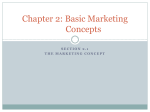
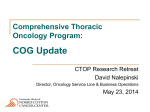
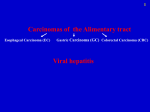
Surveillance and Diagnosis of Gastroesophageal Carcinoma David Watkins, MB BS, MRCP Consultant Medical Oncologist Gastrointestinal Cancer Unit Royal Marsden Hospital London and Surrey, United Kingdom This program is supported by an educational donation from Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology About These Slides Our thanks to the presenters who gave permission to include their original data Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent These slides may not be published or posted online without permission from Clinical Care Options Disclaimer The materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Program Faculty Program Director: Faculty: Manish A. Shah, MD David Watkins, MB BS, MRCP Director, Gastrointestinal Oncology Weill Cornell Medical College NewYork-Presbyterian Hospital New York, New York Consultant Medical Oncologist Gastrointestinal Cancer Unit Royal Marsden Hospital London and Surrey, United Kingdom Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Faculty Disclosures Manish A. Shah, MD, has disclosed that he has received consulting fees and contracted research support from Genentech and sanofi-aventis. David Watkins, MB BS, MRCP, has no significant financial relationships to disclose. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology World Cancer Incidence Stomach 8% Stomach 16% Stomach 7% Stomach 8% Esophagus 8% Esophagus 7% Cancer Research UK. GLOBOCAN 2008 v. 1.2. Cancer incidence and mortality worldwide. Ferlay J, et al. Int J Cancer. 2010;127:2893-2917. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology World Cancer Incidence Stomach ~68,800 Stomach ~595,300 Stomach ~15,600 Stomach ~14,100 Esophagus ~7100 Esophagus ~15,500 Cancer Research UK. GLOBOCAN 2008 v. 1.2. Cancer incidence and mortality worldwide. Ferlay J, et al. Int J Cancer. 2010;127:2893-2917. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology World Cancer Incidence Stomach 8% Squamous cell esophagus Stomach 16% Stomach 7% Stomach 8% Esophagus 8% Esophagus 7% Cancer Research UK. GLOBOCAN 2008 v. 1.2. Cancer incidence and mortality worldwide. Ferlay J, et al. Int J Cancer. 2010;127:2893-2917. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Esophageal Cancer Age-Standardized Incidence and Mortality: Males Southern Africa Eastern Asia Eastern Africa World Northern Europe South-Central Asia Western Europe South America Northern America Central and Eastern Europe Australia/New Zealand Incidence Mortality Stomach Cancer 0 10 20 30 Rate per 100,000 40 Eastern Asia Central and Eastern Europe World South America Southern Europe Central America Western Asia Caribbean Southeastern Asia Western Europe Northern Europe Incidence Mortality 0 Cancer Research UK. 50 10 20 30 Rate per 100,000 40 50 Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Age-Standardized Mortality Trends: Males 90 80 Stomach Cancer 11 Japan UK USA 10 Esophageal Cancer Japan UK USA 9 70 60 50 40 30 Rate per 100,000 Rate per 100,000 8 7 6 5 4 3 20 10 0 1950 1960 1970 1980 1990 2000 Yr World Health Organization. Mortality database. 2 1 0 1950 1960 1970 1980 1990 2000 Yr Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Age-Standardized Mortality Trends: Males All Cancers 11 200 10 180 9 160 8 Rate per 100,000 Rate per 100,000 220 140 120 100 80 60 40 Japan UK USA 20 0 1950 1960 1970 1980 1990 2000 Yr World Health Organization. Mortality database. Esophageal Cancer 7 6 5 4 3 2 Japan UK USA 1 0 1950 1960 1970 1980 1990 2000 Yr Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Age-Standardized Mortality Trends: Esophageal Cancer 55 Squamous Regions 11 Kazakhstan Turkmenistan Uzbekistan 50 45 10 9 35 30 25 20 7 6 5 4 15 3 10 2 5 1 0 1981 Japan UK USA 8 Rate per 100,000 Rate per 100,000 40 Esophageal Cancer 1991 2001 Yr World Health Organization. Mortality database. 0 1950 1960 1970 1980 1990 2000 Yr Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Risk Factors for Gastroesophageal Cancer Diet, alcohol, hot drinks, tobacco smoking Acid reflux, obesity, smoking, diet Esophagus Gastroesophageal junction Liver Cardiac sphincter H. pylori, atrophic gastritis, diet Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Barrett’s Esophagus GERD: principle risk factor for Barrett’s esophagus[1] Only 1% to 3% of patients will develop cancer[2] Assessed endoscopically, histologically[3] – Length of segment – Grade of dysplasia – Low grade: antireflux therapy (medical) recommended, followed by endoscopic surveillance every 6-12 mos – High grade: antireflux therapy, followed by repeat endoscopic assessment and specialist review. – Potential role for EMR, ablative therapy, surgery 1. Jemal A, et al. CA Cancer J Clin. 2011;61:69-90. 2. Schnell TG, et al. Gastroenterology. 2001;120:16071619. 3. AGA, et al. Gastroeneterology. 2011;140:1084-1091. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Screening and Surveillance for Barrett’s Esophagus BOSS: Barrett’s Esophagus Surveillance Study[1] – Endoscopy with biopsy every 2 yrs for 10 yrs vs endoscopy as indicated[1] 1. Clinicaltrials.gov. NCT00987857. 2. Kadri SR, et al. BMJ.2010;341:c4372. 3. Lao-Sirieix P, et al. Gut. 2009;58:1451-1459. 4. Cancer Research UK. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Screening and Surveillance for Barrett’s Esophagus BOSS: Barrett’s Esophagus Surveillance Study[1] – Endoscopy with biopsy every 2 yrs for 10 yrs vs endoscopy as indicated[1] Identification of Barrett’s in the general population – Cytosponge as a nonendoscopic procedure for the detection of Barrett’s esophagus in primary care[2] – Microarray datasets were used to identify putative biomarkers present in Barrett’s esophagus but absent from normal mucosa[3] – Trefoil factor 3 – marker of Barrett’s esophagus[3] – Under evaluation in BEST2 study; 500-700 cases and 500-700 controls[4] 1. Clinicaltrials.gov. NCT00987857. 2. Kadri SR, et al. BMJ.2010;341:c4372. 3. Lao-Sirieix P, et al. Gut. 2009;58:1451-1459. 4. Cancer Research UK. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Data on H. pylori Eradication Studies Multicenter, prospective cohort study 2000-2007 (Japan)[1] Randomized placebo-controlled study 1994-2002 (China)[2] – 4133 patients with H. pylorisensitive peptic ulcers elected to undergo H. pylori eradication or standard antacid therapy – 1630 healthy H. pylori carriers randomized to H. pylori eradication vs placebo – 56 gastric cancer cases with mean follow-up of 5.6 yrs – No significant incidence difference with vs without eradication treatment in overall population (P = .33) – Overall no significant difference in incidence with vs without eradication therapy – Incidence ratio: 0.58 (95% CI: 0.28-1.19) – 18 gastric cancer cases – In subgroup without precancerous lesions at entry (n = 988), eradication treatment was associated with significant reduction in gastric cancer incidence (P = .02) 1. Mabe K, et al. World J Gastroenterol. 2009;15:2490-2497. 2. Wong BC, et al. JAMA. 2004;291:187-194. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Dietary/Lifestyle Factors and Cancer Incidence Strong associations of stomach cancer with the intake of highly salted foods including salted fish and pickled vegetables A diet high in fresh fruit and vegetables seems to reduce the risk of esophageal cancer Higher levels of selenium in the blood were shown to reduce the risk of esophageal cancer by almost 50% Obesity roughly doubles the risk of adenocarcnima of the esophagus; accounts for approximately 20% of cases Smoking tobacco and excess alcohol are some of the main risk factors for esophageal cancer in the Western parts of the world Chewing tobacco or betel quid is also associated with an increased risk of cancer of the esophagus Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Trends in Obesity 80 USA England Spain Austria Australia France Korea Canada Italy Proportion Overweight (%) 70 60 50 40 30 20 10 0 1970 1980 1990 2000 Yr Wang YC, et al. Lancet. 2011;378:815-825. 2010 2020 Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Aspirin as Primary Prevention 1.8 Randomised trail data Significant effect (P < .05) Trend (P < .1) No effect (P > .1) Case-control studies (odds ratio) 1.6 Renal 1.4 Endometrial 1.2 Bladder 1.0 0.8 Pancreatic Ovarian Lymphoma Prostate Melanoma Breast Gastric Lung Leukemia Colorectal 0.6 Biliary Esphageal (no cohort data) 0.4 0.4 0.6 0.8 1.0 1.2 Cohorts (risk ratio) Algra AM, et al. Lancet Oncol. 2012;13:518-527. 1.4 1.6 1.8 Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Aspirin as Primary Prevention – AspECT Study A phase III, randomized study of aspirin and esomeprazole chemoprevention in Barrett's metaplasia 2500 Patients – Recruitment completed Esomeprazole Clinicaltrials.gov. NCT00357682. Randomize Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Transition From Normal Mucosa to Barrett’s Esophagus Damage to squamous epithelium Mutagenic effects Facilitating molecular events Exposure of multipotential stem cells to acid results in abnormal differentiation Potential involvement of stromal factors Ongoing exposure to gastric acid Nitric oxide from dietary nitrates Upregulation of COX2: increase invasion, proliferation Altered p16: deregulation of cell-cycle checkpoint Deregulation of p53: deregulation of genomic maintenance Zhang HY, et al. Cancer Lett. 2009;275:170-177. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Transition From Barrett’s Esophagus to Invasive Cancer Genomic instability[1] Invasive cancer P9 LOH P17 LOH DNA content abnormality Characteristic genomic heterogeneity[2] 1. Zhang HY, et al. Cancer Lett. 2009;275:170-177. 2. Jankowski JA, et al. Am J Pathol. 1999; 154: 965-973. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Transition From Barrett’s Esophagus to Invasive Cancer Individual 1 A 89% A 69% A 51% B 11% B 31% C 49% 21 cM G 91% D 100% A 68% 35 cM E 100% F 100% C 32% 33 cM Incidence of esophageal adenocarcinoma Shannon index = 1.60 Divergence = 0.21 H 9% I 100% I 100% I 100% I 100% H 100% J 100% P < .001 0.8 Genetic divergence, upper quartile 0.4 0.2 Lower 3 quartiles 0.0 0 22 cM Individual 3 1 2 3 4 5 6 Yrs of follow-up 7 Maley CC, et al. Nature Genetics. 2006;38:468-473. K 100% L 100% K 100% 24 cM 28 cM Shannon index = 1.15 Divergence = 0.05 1.0 0.6 Individual 4 Incidence of esophageal adenocarcinoma Biopsies: Individual 2 A 100% 21 cM 30 cM Shannon index = 0.64 Divergence = 0.27 M 100% M 100% M 100% M 100% M 100% Shannon index = 0 Divergence = 0 1.0 P = .044 0.8 0.6 Segment length, upper quartile 0.4 0.2 Lower 3 quartiles 0.0 0 1 2 3 4 5 6 Yrs of follow-up 7 140 120 100 0 Beroukhim R, et al. Nature. 2010;463:899-905. Myeloproliferative Disorder Myxoid Liposarcoma Acute Lymphoblastic Leukemia Synovial Sarcoma Medulloblastoma Neuroblastoma Renal GIST Hepatocellular Non-Hodgkin’s Lymphoma Colorectal Glioma Mesothelioma All Cancers Thyroid Melanoma Prostate Leiomyosarcoma NSCL Ovarian SCL Breast Gastric Esophageal Squamous Esophageal Adenocarcinoma Pleomorphic Liposarcoma Malignant Fibrous Histiocytoma Dedifferentiated Liposarcoma SCNAs Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Tumor Heterogeneity Average Number of SCNAs per Tumor Type Amplifications Deletions 80 60 40 20 Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Molecular Drivers and Therapeutic Targets Chromosomal instability is the most common phenotype High-level gene amplification is a late event – Most frequently observed amplification events – ERBB2 – CCNE1 – KRAS – EGFR – CCND1 – C-MYC Miller CT, et al. Clin Cancer Res. 2003;9:4819-4825. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Molecular Drivers and Therapeutic Targets Chromosomal instability is the most common phenotype High-level gene amplification is a late event – Most frequently observed amplification events – ERBB2 - proven – CCNE1 - ? targetable – KRAS - ? targetable – EGFR – targetable - unproven – CCND1 - ? targetable – C-MYC - ? targetable Identification of the proliferative drivers should result in active novel treatment options Miller CT, et al. Clin Cancer Res. 2003;9:4819-4825. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Molecular Classification of Gastric Cancer Using cDNA Expression Analysis Gastric cancers treated uniformly, despite epidemiologic, anatomic, and histopathologic distinctions between subtypes Can subtypes be distinguished by gene expression analysis? – Patients with localized gastric cancers (N = 36) – cDNA expression analysis of endoscopic biopsy tissues by microarray Proximal nondiffuse, diffuse, and distal nondiffuse gastric cancers can be distinguished by gene signatures – Supervised classification: > 85% success in distinguishing subtypes Shah MA, et al. Clin Cancer Res. 2011;17:2693-2701. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Molecular Tumor Characterization and Classification Comprehensive genome analysis of 233 gastric cancer samples and 98 matched nonmalignant gastric samples 22 recurrent alterations identified – 13 amplifications; 9 deletions – Included known targets and novel genes – Mutual exclusivity of alterations identified 5 distinct gastric cancer subgroups defined by specific alterations Deng N, et al. Gut. 2012;61:673-684. FGFR2 KRAS ERBB2 = 72/193 (37.3%) EGFR MET RTK/RAS absent Data suggest that ≥ 37% of gastric cancer cases may be responsive to RTK/RAS-targeted therapy Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Implications of Genetic Heterogeneity Solid tumors often show heterogeneity Subpopulations with differing molecular characteristics Turner NC, Reis-Filho JS. Lancet Oncol.2012;13:e178-85. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Implications of Genetic Heterogeneity Targeted therapy Turner NC, Reis-Filho JS. Lancet Oncol.2012;13:e178-85. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Implications of Genetic Heterogeneity Targeted therapy Turner NC, Reis-Filho JS. Lancet Oncol.2012;13:e178-85. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Implications of Genetic Heterogeneity Targeted therapy Turner NC, Reis-Filho JS. Lancet Oncol.2012;13:e178-85. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Acquired Resistance to Targeted Therapies Acquired resistance targeted therapy Clonal selection of resistant subpopulation Need for biopsies at the time of disease progression Evidence of relevance in NSCLC Turner NC, Reis-Filho JS. Lancet Oncol.2012;13:e178-85. Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Novel Methods for Molecular Assessment Analysis of circulating tumor cells – Currently limited by technology (~ 50% of patients) – New platforms in development – Suitable for all biomarker analysis – Potential to replace tissue biopsy Analysis of circulating tumor DNA – Tumor DNA mutational testing – Potential for broader role? Imaging biomarkers – Radiolabeled targeted agents Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology Conclusions Wide variation in global incidence – Diet, life style, H. pylori Falling incidence of gastric and squamous cancer Barrett’s/esophageal carcinoma – Rising incidence – Screening strategies being studied – Needs better markers to predict risk of progression Knowledge of the molecular drivers will lead to new therapies Gastroesophageal Carcinoma: New Directions in Mechanistically Targeted Therapy clinicaloptions.com/oncology NCI’s 24 Provocative Questions How does obesity contribute to cancer risk? What environmental factors change the risk of various cancers when people move from 1 geographic region to another? Why don't more people alter behaviors known to increase the risk of cancers? Given the evidence that some drugs commonly and chronically used for other indications, such as an anti-inflammatory drug, can protect against cancer incidence and mortality, can we determine the mechanism by which any of these drugs work? Are there definable properties of a nonmalignant lesion that predict the likelihood of progression to invasive or metastatic disease? National Cancer Institute Provocative Questions Project. Go Online for More CCO Coverage of Chicago 2012! Capsule Summaries of all the key data, plus CME-certified Slidesets exploring the clinical implications of these findings Downloadable slides: for use as a study resource or in your noncommericial presentations clinicaloptions.com/oncology