Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Toxicodynamics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug discovery wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
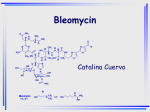
Antineoplastic AB Prepared by: Bashayer Al- Balkhi Layla Al-Blowi Alanoud Al-Homoud Amal Al-Subaity Zeina Al-Abdulkareem Supervised by: Dr. Qadria AL-Deab Dr. Areej Altaweel Introduction to cancer Our bodies are made up of millions of tiny cells. Most of our cells divide and multiply from time to time - when an old cell is worn out or damaged, a new cell is formed to replace it. Each cell contains genes (made up from DNA). The proteins inside the gene control when the cell should divide and multiply. If the gene is damaged or altered, the cell becomes abnormal. This abnormal cell can then divide and multiply, without knowing when to stop. When a group of abnormal cells clump together and grow, a tumour forms. There are two types of tumours: - Benign tumours are not cancerous, and will not invade or spread to other parts of the body. - malignant tumours are the real cancers. They can grow very quickly, invade nearby tissues and organs, and cause damage. They may even spread to other parts of the body and cause secondary tumours (metastases). There are two broad categories of cancers: - Carcinomas: cancers that develop in the surface linings of organs. - Sarcomas: cancers that appear in the cells of solid tissues, such as muscles, bones and blood vessels. Carcinomas are the most common. Types of cancer There are about 200 different types of cancer. Some types are more serious than others, some are more easily treated, and others have better survival rates. They include: bladder, breast, colon, rectal, kidney (renal cell) cancer, leukaemia, lung, pancreatic, prostate, melanoma, and thyroid cancer. Symptoms unexplained lumps and swellings, tiredness, weight loss, poor appetite, night sweats, fever, and anaemia. Causes Hereditary. Smoking. Diet. Environmental factors such as UV light from the sun. Diagnosis X-ray. Ultrasound. Computerised tomography (CT or CAT) scan. Magnetic resonance imaging (MRI) scan. Positron emission tomography scan (PET). Once the problem area is found, blood and tissue samples (biopsy) will be taken for analysis and testing to determine if, or how far, the cancer has spread in the body (this is called staging). Prevention Stop smoking. Eat a healthy diet. Reduce alcohol intake. Use protection from the harmful effects of the sun. Treatment Surgery: the main treatment for most solid tumours, especially when the cancer is in the early stages and has not spread to other areas of the body. Radiotherapy: aims to destroy the cancerous cells with radiation from X-rays. Chemotherapy: Different drug combinations are given depending on the type of cancer. The drugs are given either by mouth, or more commonly by IV, to try and kill cancer cells or stop them from spreading. Chemotherapy Depending on which drug combination given, there may be some side effects, such as sickness, diarrhoea, hair loss and mouth sores. The majority of chemotherapeutic drugs can be divided in to: alkylating agents, antimetabolites, mitotic inhibitors, antineoplastic antibiotics, hormonal agents, and miscellaneous antineoplastic agents. Antineoplastic antibiotic A type of anticancer drug that blocks cell growth by interfering with DNA. The antineoplastic antibiotics are products of Streptomyces. The important drugs in this group include, actinomycin D (dactinomycin), doxorubicin, mitoxantrone, and bleomycin. Drugs less commonly used include daunorubicin, mithramycin, and mitomycin. Doxorubicin Drug Description Doxorubicin is an anthracycline glycoside antineoplastic antibiotic produced by Streptomyces peucetius var. caesius. Structure and SAR Daunorubicin: R. = OCH3, R2 = H Doxorubicin: R. = OCH3, R2 = OH ldarubicin: R. = H, R2 = OH Carminomycin: R. = OH, R2 = H The anthracycline antibiotics have tetracycline ring structures with an unusual sugar, daunosamine, attached by glycosidic linkage. Cytotoxic agents of this class all have quinone and hydro quinone moieties on adj acent rings that permit them to function as electron-accepting and donating agents. Although there are marked differences in the clinical use of daunorubicin and doxorubicin, their chemical structure differ only by a single hydroxyl group on C-14 The anthracyclinones differ from each other in the number and location of the phenolic hydroxyl groups, the degree of oxidation of the two-carbon side chain at the position 9, and the presence of a carboxylic acid ester at position 10 Doxorubicin binds to nucleic acids, presumably by specific intercalation of the planar anthracycline nucleus with the DNA double helix. The anthracycline ring is lipophilic, but the saturated end of the ring system contains abundant hydroxyl groups adjacent to the amino sugar, producing a hydrophilic center. The molecule is amphoteric, containing acidic functions in the ring phenolic groups and a basic function in the sugar amino group. It binds to cell membranes as well as plasma proteins. Mechanism of action Doxorubicin binds directly to DNA via intercalation between base pairs on the DNA helix. Doxorubicin also inhibits DNA repair by inhibiting topoisomerase II. These actions result in the blockade of DNA and RNA synthesis and fragmentation of DNA. Doxorubicin is also a powerful iron-chelator. The iron-doxorubicin complex can bind DNA and cell membranes producing free radicals that immediately cleave DNA and cell membranes. Doxorubicin appears to be active in all phases of the cell cycle and although maximally cytotoxic in S phase, it is not cell cycle-phase specific. Mechanism of Resistance: 1- One mechanism for adriamycin resistance, impaired cellular drug uptake, may experimentally be overcome by concomitant amphoteracin B (Fungizone) injection in some adriamycin-resistant patients. 2- Acceleration of the efflux, P-glycoprotein, synthesized in high quantity as a result of gene amplification. 3- Increased GSH peroxidase activity. 4- Decreased activity of topoisomerase II. Spectrum & uses In experimental animal systems, Adriamycin has wide spectrum of activity in both solid tumors such as sarcomas, carcinomas, melanomas as well as transplantable and viral induced leukemia lymphomas. Uses Carcinomas-Doxorubicin: breast carcinoma, ovarian carcinoma , thyroid carcinoma endometrial carcinoma, testicular carcinoma , lung carcinoma Sarcomas-Doxorubicin: Ewing's sarcoma, osteosarcoma, rhabdomyosarcomas Hematologic Cancers-Doxorubicin: acute leukemia, multiple myeloma , Hodgkin's disease, non-Hodgkin's lymphoma The most often reported combination, AdOAP, includes Adriamycin with vincristine (Oncovin), cytarabine (ARAC), and prednisone. For resistant Hodgkin's and non-Hodgkin's lymphoma the combination CHOP has demonstrated activity and combines Adriamycin (hydroxyl daunorubicin) with cyclophosphamide, Oncovin, and prednisone. Rout of administration: administered IV Dosage Form: injection, powder, lyophilized, for solution. Pharmacokinetics Absorption: Oral: poor <50% Metabolism: Primarily hepatic to doxorubicinol (active) - then to inactive aglycones, conjugated sulfates and glucoronides Excretion: feces 40-50% as unchanged drug, urine 3-10% as metabolites. Drug Interaction AGENT EFFECT MECHANISM MANAGEMENT barbiturates (phenobarbital) delayed, moderate possible; decreased pharmacologica l effects of doxorubicin doxorubicin metabolism increased by barbiturates via CYP3A4 induction monitor therapy calcium channel blockers (e.g: verapamil) doxorubicininduced cardiotoxicity may be increased additive toxicity monitor cardiac function throughout treatment Cyclophosphamide doxorubicininduced cardiotoxicity may be increased additional myocardial cell damage caution, but combination regime is commonly used digoxin tablets delayed, moderate, suspected; decreased pharmacological effects of digoxin digoxin absorption decreased by antineoplastic agents due to alteration of intestinal mucosa monitor for decreased effect of digoxin quinolones (e.g., ciprofloxacin) delayed, moderate, possible; the antimicrobial effect of quinolones may be decreased quinolone absorption decreased by antineoplastic agents due to alteration of intestinal mucosa monitor therapy stavudine decreased pharmacologica l effects of stavudine stavudine avoid metabolism to concomitant active drug is use decreased by doxorubicin due to inhibition of phosphorylation streptozocin greatly enhanced leukopenia and thrombocytope nia doxorubicin half caution life possibly prolonged Doxorubicin (Adriamycin) has been found to be physically incompatible with the following drugs 1. Fluorouracil (5-FU). 2. Dexamethasone 3. Hydrocortisone sodium phosphate 4. Aminophylline 5. Cephalothin sodium (Keflin) 6. Sodium heparin Side effects Cardiovascular: Acute: arrhythmias, heart block, pericarditismyocarditis, facial flushing GIT: acute nausea and vomiting, mucositis, ulceration, necrosis of the colon, anorexia and diarrhea, stomatitis, esophagitis. Genitourinary: discoloration of urine (red) Hematologic: myelosuppression, leucopenia, dose limiting toxicity. Endocrine & metabolic: hyperuricemia Dactinomycin Introduction Common trade name : Cosmegen. Dactinomycin is a drug used to treat many kinds of cancer . It is a derivative of streptomyces parvulus. Structure-Activity Relationship The planar phenoxazone actinocin, which is responsible for the yellow-red colour of the compounds. The differences among naturally occurring actinomycins are confined to the peptide side chains, and the variations are in the structure of the constituent amino acids. By varying the amino acid content of the growth medium, it is possible to alter the types of actinomycins produced and the biological activity of the molecule . Mechanism of Action The planar phenoxazone ring intercalates between adjacent guanine-cytosine base pairs of DNA . The summation of these interactions provides great stability to the dactinomycin-DNA complex, and, as a result of the binding of dactinomycin, the transcription of DNA by RNA polymerase is blocked. Mechanism of resistance Resistance is due to an increased efflux of the antibiotic from the cell via P-glycoprotein. DNA repair may be also play a role . Uses Ewings sarcoma Rhabdomyosarcoma Wilms tumor Less frequent uses : Germ cell tumours Melanoma Testicular cancer Uterine cancer Dosage The dose intensity per 2-wk cycle for adults and children should not exceed 15 mcg/kg/day or 400 to 600 mcg/m 2 /day for 5 days. Pharmacokinetic administered by parentral injection . Excreted both in bile and in the urine and disappears from plasma with a terminal halflife of 36 hours. Metabolism is minimal. Does not cross the blood-brain barrier. Drug interaction AGENT EFFECT MECHANISM MANAGEME NT Halogenate d inhalation anesthetics (e.g, enflurane , halothane ) Increased hepatotoxicity additive caution Side effect nausea and vomiting loss of appetite abdominal pain diarrhea difficulty swallowing thinned or brittle hair skin irritation Contraindication If you are allergic to any ingredient in this medicine. If you have chickenpox , or shingles (herpes zoster infection), or if you have had either of these infections recently. Warnings Dactinomycin is extremely corrosive to soft tissue. If extravasation occurs during IV use, severe damage to soft tissues will occur. Avoid use in pregnancy ( teratogenic ) and avoided in breast feeding. Mitomycin Introduction The mitomycins are a family of aziridine-containing natural products isolated from Streptomyces lavendulae. use as a chemotherapeutic agent by virtue of its anti-tumor antibiotic activity. Brand Names: Mutamycin® Index Terms: Mitomycin-C, Mitomycin-X, MTC, NSC-26980. Strucrure & SAR 1. 2. 3. at least three reactive center of compound have been identified: Cl carbon of mitosane ring. Quinone ring structure, which can undergo one or two electron reduction Urethane groups that can open to form an alkylating site at CI0. Mechanism of action After intracellular enzymatic reduction of quinon and loss of the methoxy group, mitomycin becomes a bi-functional or trifunctional alkylating agent; it can also be activated nonenzymatically. The drug inhibits DNA synthesis and cross links DNA at N6 position of adenine and at the O6 and N2 position of guanine. In addition, single-strand breakage of DNA is caused by reduced mitomycin; this can be prevented by free radical scavengers. Mitomycin is derived from Streptomyces caespitosus and has antineoplastic activity similar to that of the alkylating agents. Mitomycin selectively inhibits the synthesis of DNA by causing cross-linking, degrades preformed DNA, and causes nuclear lysis and formation of giant cells. At high concentrations, cellular RNA and protein synthesis may also be suppressed. Mitomycin is cell cycle phase-nonspecific, although it has its maximum effect in late G- and early S-phases. Mechanism of resistance Resistance has been ascribed to deficient activation, intracellular inactivation of the reduced quinine, and P-glycoproteinmediated drug efflux. Even if we give combination of therapy this protein is capable of causing rapid efflux of multi-drug resistance (MRD). MRD type drugs, thus protecting the cells from damage by preventing these drugs from reaching their intracellular target. Uses & spectrum Primary uses: Anal cancer, Bladder cancer (intravesical), Colon cancer, Gastric cancer, Head and neck cancer, Primary unknown cancer, Pseudomyxoma peritonei. Other uses: Breast cancer, Cervical cancer, Conjunctival melanoma (topical), Lung cancer, non-small cell, Ocular surface squamous neoplasia (topical), Pancreatic cancer, Primary acquired melanosis with atypia (topical). Compatible: bleomycin, doxorubicin, cyclophosphamide, fluorouracil, furosemide, methotrexate…etc. Incompatible: Aztreonam, cefepime, etoposide phosphate, filgrastim, gemcitabine…etc. Dosage: Single agent therapy: I.V.: 20 mg/m2 every 6-8 weeks. Combination therapy: I.V.: 10 mg/m2 every 6-8 weeks. Administration: Administer slow I.V. push or by slow (15-30 minute) infusion via a freely-running dextrose or saline infusion. Consider using a central venous catheter. Pharmacokinetic: Distribution: Vd: 22 L/m2; high drug concentrations found in kidney, tongue, muscle, heart, and lung tissue; probably not distributed into the CNS Metabolism: Hepatic Half-life elimination: 23-78 minutes; Terminal: 50 minutes Excretion: Urine (<10% as unchanged drug), with elevated serum concentrations. Drug interaction: Agent: vinca alkaloids. Effect: shortness of breath and broncho-spasm have been reported in patients receiving vinca alkaloids in combination with or after mitomycin. Mechanism: unknown. Management: may be managed with bronchodilators, steroids and/or oxygen Side effect Cardiovascular: CHF Central nervous system: Fever Dermatologic: Alopecia, nail banding/discoloration Gastrointestinal: Nausea, vomiting and anorexia Hematologic: Anemia, myelosuppression 1 to 10%: Dermatologic: Rash Gastrointestinal: Stomatitis Neuromuscular: Paresthesia Renal: Creatinine increased Respiratory: Interstitial pneumonitis, infiltrates, dyspnea, cough. <1%: Malaise, pruritus, extravasation reactions, hemolytic uremic syndrome, renal failure, bladder fibrosis/contraction (intravesical administration). Precaution Before taking this drug, tell your doctor: If you are pregnant, or breastfeeding. This drug may cause birth defects if either the male or female, cause sterility. If you have any of the following medical problems: chickenpox or gout, heart disease, kidney stones, liver disease, or other forms of cancer. While you are being treated with mitomycin, and after you stop treatment, do not have any immunizations (vaccinations) without your doctor’s okay. Mitomycin can lower your blood counts. Your doctor will check your blood counts before and after each treatment. Mitomycin is given intravenously. If the drug accidentally leaks out of the vein where it is given, it may damage the tissue and cause scarring. Hair loss is temporary, and your hair will grow back after treatment. Mitomycin can cause severe nausea and vomiting Contraindication Hypersensitivity to mitomycin or any component of the formulation; thrombocytopenia; coagulation disorders, increased bleeding tendency; pregnancy. Bleomycin Introduction Is a glycosylated peptide antibiotic produced by the bacterium Streptomyces verticillus. When used as an anti-cancer agent, the chemotherapeutical forms are primarily bleomycin A2 and B2 . Common trade name: Blenoxane ® Structure The bleomycin are water-soluble, basic glycopeptides. It forms equimolar complexes with metal ions SAR 1-The bleomycins are family of basic gycopeptides that differ from one another in their terminal alkylamine group . 2-The toxic effects and antitumor spectrum are probably modified by changes in the terminal alkylamine moiety . 3-The bleomycin Cu(π) complex has no antitumor activity . 4-The active form contain Fe(π) with complex formation through the nitrogen moiety in : β-aminoalanine Propionamide Β-hydroxyl-histidine Mannose Mechanism of action The cytotoxic action results from their ability to cause oxidative damage to the deoxyribose of the thymidylate and other nucleotides leading to single- and double-stranded breaks in DNA . This action results in inhibition of DNA synthesis . It is believed that bleomycin chelates metal ions producing a pseudoenzyme that reacts with oxygen to produce superoxide and hydroxide free radicals that cleave DNA. In addition, these complexes also mediate lipid peroxidation and oxidation of other cellular molecules. Resistance Although the mechanisms of resistance have not been elucidated, experimental systems have implicated increased levels of bleomycin hydrolase ( or deaminase ) , glutathione-S-transferase, and possibly, increased efflux of drug. DNA repair also may contribute . Spectrum & uses Hodgkin’s Disease It is used with doxorubicin, vinblastine, and dacarbazine. Testicular Cancer bleomycin, cisplatin, and etoposide . Pleural Effusions It is used by intracavitary injection as a sclerosing agent . bleomycin has been suggested as a suitable alternative to tetracycline . Head and Neck Cancer In a patients receiving bleomycin, cisplatin, methotrexate, and vincristine for head and neck cancer had higher rates of complete response. Cervical Cancer combination chemotherapy regimens : bleomycin, cisplatin, and ifosfamide with mesna. AIDS-related Kaposi’s Sarcoma combination chemotherapy with the drug (e.g., bleomycin, doxorubicin, and a vinca alkaloid Side effect Rash Fever Chills Scarring and stiffening of the lungs causing breathlessness Flushing of the skin due to widening of the small blood vessels Loss of appetite Inflammation of the lining of the mouth Inflammation of the lungs Renal toxicity Precaution & Contraindication Contraindicated in: patients who have a history of hypersensitivity reaction to bleomycin. Use with caution in patients: with compromised pulmonary function & compromised renal function . Carcinogenicity Mutagenicity Fertility Pregnancy: FDA Pregnancy Category D. Breastfeeding Pharmacokinetics Absorption : It is not significantly absorbed from the GI tract and the drug must be administered parenterally. Distribution : The drug is distributed mainly into the skin, lungs, kidneys and peritoneum, Concentrations of the drug in tumor cells of the skin and lungs are higher than those in hematopoietic tissue. Elimination : the terminal half-life of the drug is inversely related to creatinine clearance. In patients with normal renal function, 60–70% of a parenterally administered dose is excreted in the urine as active drug. Drug interaction AGENT cisplatin digoxin phenytoin vincristine EFFECT may increase risk of bleomycin toxicity . may decrease digoxin levels . may decrease phenytoin levels . sequential administration of vincristine given before bleomycin may improve bleomycin efficacy Conclusion Doxorubic in M.O.A Binds to DNA Inhibit DNA & RNA synthesis Dactinomycin Prevent transcription Bleo-mycin Mitomycin Degradate the preformed DNA Bifunctional Alkylating agent & may also Degradate DNA Through Generation of Free radical R.O.A IV infusion Parentrally (IV,IM, intralesional ) Side effect *Cardiac *Myelodamage suppression *Local necrosis *Hair loss *Myleosuppression Parentrally IV *Allergic reaction *Hyperpyrexia *Pulmonary fibrosis *Myelosuppression *Kidney damage Indication * breast carcinoma *Hodgkin's disease * nonHodgkin's lymphoma *Wilms tumor *Hodgkin's disease *Rhabdom *Testicular yosarcoma Cancer *Pleural Effusions *Anal cancer *Bladder cancer References Charles F. Lacy, Lora L. Armstrong, Morton P. Goldman, Leonard L. Lance. Drug Information Handbook International, 12th edition. David S. Fischer, M. Tish Koobf, Henry J. Durivage. The Cancer Chemotherapy Handbook, 5th edition. Joel G. Hardmen, Lee E. Limbird. Consultant editor: Alfred Goodman Gilman.Goodman & Gilman's The Pharmacological Basis of Therapeutics, 10th edition. http://www.nhsdirect.nhs.uk/articles/article.aspx The Pharmacological Basis of Tberapeutics. Goodman and Gilman, tenth edition, 2001. Drug information hand book, 2007. British national formulary, 1989. http://en.wikipedia.org/wiki/Mitomycin http://www.bccancer.bc.ca/HPI/DrugDatabase/DrugIndexPro/Mitomy cin.htm http://www.cancer.org/docroot/CDG/content/CDG_mitomycin.asp MedlinePlus Drug Information Dactinomycin.htm Dactinomycin facts and comparsions at Drugs_com.htm Complete Dactinomycin information from Drugs_com.htm