Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
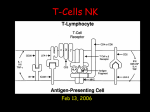
Immunosuppressive medications Mechanisms Usage Side effects Allograft rejection T cell (CD4+) dependent recognize intact MHC class II antigens of the surface of transplanted cells recognize processed antigens on self APCs T cell receptors (TCRs) major TCR a + b heterodimer minor TCR g + d heterodimer constant and variable portions Allograft rejection TCR engages presented alloantigen T cell is activated TCR-CD3 complexes transduce signal 1 TCR-CD3 complexes and CD4 co-receptors are phosphorylated Transcription factors induce expression of new proteins involved in cell division and proliferation Allograft rejection Activated CD4+ cells differentiate into two distinct populations Type 1 T helper cells (Th1 cells) IL-2, IFN-g mediate activation of macrophages, and delayed hypersensitivity Type 2 T helper cells (Th2 cells) IL-4, IL-5, IL-10, IL-13 involved in B cells function Allograft rejection Activated CD4+ cells secrete cytokines which activate CD8+ cytotoxic cells CD8+ cells recognize HLA class I molecules, and, if T helper cytokines (IL-2, IL-4, IL-5) are present differentiate, divide, and destroy cells with the recognized markers. Allograft rejection CD8+ secretory mechanism granzymes (serine esterases) perforins kill by DNA degradations and osmotic lysis CD8+ contact mechanism Fas (CD95) on target meets the Tcell Fas ligand engagement of Fas ligand triggers apoptosis Allograft rejection IL-2 from macrophages induces Th1 cells IL-4 from other cells induces Th2 cells Th2 cells down regulate Th1 cells (yin-yang) All T cell responses require two initiating factors: a TCR-MHC interaction and a “costimulatory” signal Tolerance is related to 1/2 stimulation: TCRMHC but no second “hit” as in absent or blocked CD40, B7 interactions Allograft rejection CD8 knockouts still reject transplants CD4 knockouts do not reject B cell responses are important in the hyperacute rejection and IgG plays a role in chronic rejection Natural killer (NK) cells recognize alloMHC directly and kill MHC negative and alloMHC cells Allograft rejection APCs take up foreign HLA proteins; HLA on a donor APC is recognized directly Ag specific T cells are activated, proliferate, and enter circulation T cells move to tissue in response to selectins or chemoattractants selectins, ICAMs, VCAMs, etc Transplantation: therapy options Avoid need - disease prevention / modificatioin Designer organs Immune tolerance Immunosuppression Immunosuppresion: history Prednisone Azathioprine Total body (lymph node) irradiation Splenectomy Anti lymphocyte globulin ---- OKT3 Cyclosporine, FK506, rapamycin Mycophenolate mofetil Daclizumab, Basiliximab Immunosuppression timeline Prednisone Azathioprine Cyclosporin Mycophenolate Tacrolimus Sirolimus 60’s 80’s 90’s 00’s Immunosuppression: induction Steroids Azathioprine CyA, FK 506 (tacrolimus), and rapamycin OKT3, ALG, ATG Mycophenolate Daclizumab Basiliximab Immunosuppression: rescue Steroids OKT3, ATG, thymoglobulin Mycophenolate ? role of receptor-blockers ? Steroids: phamacokinetics Agent specific Prednisone half life 18 - 36 hours 70% protein bound Actions do not correlate with plasma concentrations Volume of distribution variable Elderly have decreased clearance, as do women. Obesity increases clearance Prednisone: drug interactions P450 inducers increase the rate of steroid metabolism Nephrotic patients have more toxicity at the same dosage and level CyA and FK-506 may interfere Prednisone: mechanisms Glucocorticoids act upon steroid receptors and induce genes which shut off cytokine production AP-1 complexes formed of Jun and Fos proteins are bound by steroid/GR complex Similar reactions occur with Il-1, Il-3, Il-4, Il-6, IGF-1, TNF, IFN-g, Il-8, RANTES, and MCAF Prednisone: mechanisms Downregulates: collagenases, elastases, plasminogen activator complex Decreases: WBC numbers Upregulates: neural endopeptidase which degrades neuropeptides such as substance P and bradykinin Alters: adhesion molecules (ICAMs) Prednisone: mechanisms Decreases: release of Il-1b, TNF Locally inhibits: arachadonic acid metabolism (blocks PLA-A2) Inhibits: cytokine dependent COX Inhibits: platelet activation factor Prevents: synthesis of inducible NO synthase Prednisone: side effects Immunosuppression Bone and cartilage metabolism Cushing’s syndrome Gastric symptoms Weight gain Diabetes Cataracts Azathioprine Imidazole purine analogue which is the prodrug for 6-mercaptopurine (6MP) Imidazole side group preserves purine structure from degradation Converted by HGPRT to a precursor of thionuclides which inhibits PRPP synthase Inhibits AMP and GMP formation A methylnitroimidazole product may have separate effects on Ag recognition etc. Azathioprine Absorbed in 2 hrs Parent drug bioavailability is about 20% Metabolite availability is >40% Total availablity is > 60% Oxidized by GSSH Xanthine oxidase inhibitors increase toxicity, as do genetic factors in Asians Clonal mutation can lead to resistance Azathioprine Half lives of drug and active metabolite are short (50 min, 75 min) Renal elimination Hepatic disease interferes with metabolism and leads to accumulation of drug Azathioprine Excessive marrow suppression 5 - 10 days to marrow recovery Asians and patients taking allopurinol may become very cytopenic Liver disease: cholestatic disease and VOD Interstitial pneumonitis Increased malignancies Cyclosporines Norwegian soil fungus product Monstrous macrolide antibiotic ? Calcineurin inhibitor ? (E)-14,17,26,32-tetrabutyl-5-ethyl-8-(1hydroxy-2-methylhex-4-enyl) 1,3,9,12,15,18,20,23,27-nonamethyl-11,29dipropyl-1,3,6,9,12,15,18,21,24,27,30undecaazacyclodotriacontan2,4,7,10,13,16,19,22,25,28,31-undecaone Cyclosporine A: mechanisms Disrupts the calcium dependent cascade of events which follows binding of antigen to the T cell receptors and leads to activation and proliferation. Interferes with secondary messengers in cell Suppresses genes for c-myc, Il-2, Il-3, Il4, Il-5, IFN-g, and Il-2 receptors Cyclosporine CyA/Cyp inhibits calcineurin This prevents the phosphorylation of nuclear factor (NF-Atc) of activated T cells The NF-ATc cannot enter nucleus to activate its nuclear (DNA) subnunit Prevents promotion of: Il-2 gene and thus Il-2, Il-3, Il-4, IFN-g, TNF, also: AP-1, AP-3, OAP, Oct-1 and NF-kb Cyclosporine Prodrug: only active after it binds to intracellular ligands Immunophilins are small proteins which comprise 0.2 - 0.4% of cellular proteins Cyclophilins A, B, C, and D Complexes bind to calcineurin catalytic subunit and render complex inactive Inihibition stops activation of T cells Cyclosporine May upregulate TGF-b TGF- b increases endothelin 1, and extracellular matrix production Cyclosporine Inhibits B cells CyA inhibits CD40 ligand expression by inhibiting NF-ATC phosphorylation The CD40 ligand is involved in T cell, B cell interactions Alters TNF a production by macrophages Complex effects on bone marrow Cyclosporine: Side effects Nephrotoxicity related to trough levels patchy, striped, interstitial fibrosis Hypertension Cholesterol metabolism Neurotoxicity peripheral neuropathy Lethality > 1500 Cyclosporine: drug interactions Far too many to recall Interference by drugs which are metabolized by the P450 Interactions at the P-glycoprotein pump Cyclosporine-drugs : useful things Erythromycin - itraconazole - ketoconazole inhibit p450 and reduce CyA dosage (save money) reduce infections Diltiazem - verapamil (p-glycoprotein) Interfere with metabolism, other effects Nifedipine (p-glycoprotein) effect on transplant independent of CyA FK-450, Tacrolimus (Prograf) Japanese fungus product Giant macrolide molecule Not structurally related to CyA Works much like CyA * * * * * * * * * * * * * * 3S-[3R [E(1S ,3S ,4S )],4S ,5R ,8S ,9E,12R ,14R ,15S ,16R ,18S ,19S ,26aR ]] -5,6,8,11,12,13,14,15,16,17,18,19,24,25,26,26a -hexadecahydro-5, 19-dihydroxy -3-[2-(4-hydroxy-3-methoxycyclohexyl) -1-methylethenyl]-14,16-dimethoxy -4,10,12,18-tetramethyl-8-(2-propenyl) -15,19-epoxy-3H-pyrido[2,1-c] [1,4] oxaazacyclotricosine-1,7,20,21(4H,23H) -tetrone, monohydrate Tacrolimus Well absorbed Food slows absorption Peak 0.5 to 8 hours post dose Protein bound, variable volume of distribution Hepatic metabolism by P-450-3A4 Monitoring less critical than with CyA Tacrolimus: mechanisms Prodrug which binds to an immunophilin FK-BP (high affinity receptor) FK-BP not related to cyclophilins Inhibits rotamase activity of FK-BP only Does bind to rapamycin BP Complex (FK-506/FK-BP) binds to and inhibits a calcium/calmodulin-dependent serine-threonine phosphatase Tacrolimus: mechanism Inhibition of the phosphatase prevents the enzyme from dephosphorylating the transcription factors for NF-AT, AP-3, Oct-1 and others which inhibits gene turn on The result is less Il-2, Il-3, Il-4, TNF-a, IFN-g Also affects a rapamycin inhibitable system which is not calcium dependent Tacrolimus Clinically, tacrolimus is very close to CyA in terms of effects, though the binding proteins and the precise mechanisms differ Pharmacologically, the drug is 50 times more active wt for wt Blood levels are said to be much more stable Tacrolimus: toxicity Nephrotoxicity Similar to CyA Mechanism of toxicity is unknown Inhibits the P-glycoprotein multidrug transporter Tacrolimus: drug interactions Pharmacological antagonist for CyA Similar profile of drug interactions Rapamycin Yet another macrolide Not nephrotoxic ? Acts at a point beyond tacrolimus and CyA Acts on the same binding protein as tacrolimus, but the mechanisms differ Some protocols use in combination with CyA (3S,6R,7E,9R,10R,12R,14S,15E,17E,19E,21S,23S, 26R,27R,34aS)9,10,12,13,14,21,22,23,24,25,26, 27,32,33,34,34a-hexadecahydro-9,27-dihydroxy-3[(1R)-2-[(1S,3R,4R)-4-hydroxy-3-methoxycyclohexyl]- 1-methylethyl]-10,21-dimethoxy6,8,12,14,20,26- hexamethyl-23,27-epoxy-3H-pyrido[2,1-c][1,4]oxaazacyclohentriacontine-1,5,11,28,29 (4H,6H,31H)-pentone Rapamycin Binds to TOR (target of rapamycin) Inhibits signal transduction downstream from growth factor receptors (IL-2) Blocks progression from G1 to S phase of cell cycle Antagonist of tacrolimus Cooperative with cyclosporine A Mycophenolate mofetil: Inhibts inosine monophosphate dehydrogenase (IMPDH) Mycophenolate is the morpholino-ethyl ester of mycophenolic acid (a penicillium product) Non-competitive inhibitor of IMPDH Mycophenolate: mechanism Inhibits IMPDH IMPDH is a key enzyme in purine nucleoside synthesis IMPDH inhibition lowers GMP levels which occupy a key step in T cell response TCR /CD3 complex activity may need GMP Thus cell activation is inhibited Mycophenolate: mechanism Lymphocytes do not have purine salvage pathway enzymes Lymphocytes depend on IMPDH for purines Lymphocyte proliferation is blocked by MPA effect on purines Most other cells have purine salvage and are not affected Mycophenolate: mechanisms Effects can be reversed by administration of guanosine nucleotide Guanosine does not reverse AZA effects IMDPH acts if given up to 24 hours after T cell stimulation Does not act on early response genes and Ils Arrests lymphocytes in G1 phase Mycophenolate: toxicity Leukopenia Anemia GI toxicity Note: despite the “targeting” of the drug to cells without a salvage pathway, the toxicity tends to indicate all high turnover cells are at risk…….. ? a rate issue ? Antibodies ALG going ATG going MM AB gone OKT3 only option OKT3 Murine IgG2a directed against e chain of CD3 molecule Cells may be activated and then release cytokines which cause acute toxic responses Block recognition site by internalization Cells are then opsonized and sequestered by macrophages OKT3 Given IV only, 5mg a day for up to 14 days First 2 to 3 doses may trigger severe reactions which result in flu-like symptoms, acute pulmonary edema, and chemical meningitis Wt must be within 3% of dry Profound lymphopenia results OKT3 Very high risk for viral infections Use immune globulin for CMV If dose excessive, high risk for lymphoproliferative malignancy Don’t exceed 70 mg Antibodies may develop Test for Ab titer before second dose IL-2 receptor antibodies IL-2 is a major factor in the proliferation of activated Tcells in response to grafts CyA, tacrolimus inhibit IL-2 production by interfering with secondary messages which lead to stimulation of the IL-2 promoter Rapamycin inhibits secondary messenger responses (by Tyr Kinase pathways) to IL-2 stimulation Activation of T cells APC T cell Presentation of Ag to Tcell Ag receptor Proliferation/differentiation signal Activation of T cells APC T cell IL-2 rejection IL-2 and tolerance Since IL-2 stimulates Tcells in recursive manner, it would seem that IL-2 inhibition should block rejection and memory But, IL-2 knockout mice reject heart transplants Anti IL-2 treatment slows but does not prevent later rejection IL-2 neutralizing antibodies reduce tolerance IL-2 causes apoptosis of activated T cells (clonal deletion role) IL-2 effects Activation of T cells Induction of “memory cells” Induction of T cell apoptosis T cells and tolerance T cell activation is required for tolerance to develop Complete suppression of T cell response (total blockade of IL-2, for example) leads to ignorance, and the host remains primed to recognize and reject Tolerance is preferable to ignorance IL-2 inhibits the maintenance of memory cells Memory cells Naïve cells Memory cells Survival Long (years) Very long (life) Homing Circulate to secondary lymph sites Slow (high threshold) Circulate to lymphatic and non lymph tissue * Fast (low threshold) Response *Memory cells do not require secondary lymphatic structures to react T cell responses Delete (die – apoptosis) T cell Suppress ( T regulatory) Deviate Anergy Ignore -- tolerance (Th2) Memory expand clone die off memory tolerance exposure to foreign antigen time IL-2 receptor antibodies Rather than inhibit the secondary messages which lead to IL-2 production or the response to IL-2, directly attack the major element -- IL-2 IL-2 blockers are clinically available IL-2 R antibodies Daclimuzab (Zenapax) is a “humanized” antiT cell a chain IL-2 receptor antibody Basilixamb (Simulect) is a chimeric mouse anti-CD 25 monoclonal antibody with affinity for the alpha chain of the IL-2 R IL-2 receptor antibodies Vicente et al (NEJM 98): Induction protocol which included CyA and daclimizab (IL-2 receptor antibodies) Results of the study indicated there was an increase in transplant survival (95 vs 90%), and decreased rejection episodes in cadaver kidney recipients IL-2 receptor antibody Nashan et al used basiliximab as induction protocol (Lancet 350:1193-1198, 1999) They reported a reduction in biopsy proven rejection (30% vs 44%) European trial