Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Pharmacokinetics wikipedia , lookup
MTOR inhibitors wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Pharmacognosy wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Plateau principle wikipedia , lookup
Prescription costs wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Psychopharmacology wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of direct Xa inhibitors wikipedia , lookup
Discovery and development of direct thrombin inhibitors wikipedia , lookup
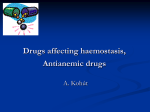
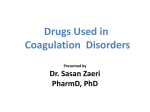
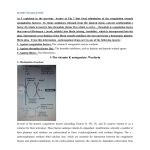
ANTICOAGULANTS Jill Gregory Medicinal Chemistry Dr. Buynak 4.23.09 Overview • Review Blood basics – composition – how blood clots • Note Instances where blood clotting is bad • Discuss Anticoagulants – Heparin – Warfarin – New Drugs • F Xa inhibitors • thrombin inhibitors • Show example Clinical Trial Blood Composition • connective tissue with cells suspended in plasma Plasma (55%) Cellular Elements (45%) water erythrocytes (red blood cells) Ions / electrolytes (K+ Ca++) leukocytes (white blood cells) plasma proteins (Fibrinogen) platelets transported substances How blood clots • Damage to endothelium (vessels) • Platelet plug • Coagulation Factors from – plasma – platelets – and damaged cells interact and activate a cascade that leads to… • Activated Fibrin: fibers woven into a patch http://www.advanced-supplements.com/neprinol.html Coagulation Cascade Intrinsic pathway Extrinsic pathway TF XIIa XII VIIa XIa IXa XI IX VIIIa X Xa Va Common pathway II (prothrombin) Each step requires: • Zymogen (precursor protein) • Activated Protease from step before • Cofactors like Ca++ IIa (thrombin) Fibrinogen Fibrin XIII XIIIa Stabilized Fibrin When would we not want clots to form?? • Clotting is good at sites of injury because it minimizes blood loss and prevents infectious agents from getting into our systems. • Clotting can be bad when occurs inappropriately in normal vessels [called thrombus] …clot can break free [called embolus] and lodge in heart, causing myocardial infarction, or in brain, causing stroke. • Thrombosis is caused by abnormalities in blood composition, vessel wall quality, and/or nature of the blood flow – Different types of thrombosis: • Venous [i.e. VTE = venous thromboembolism; DVT = Deep-vein thrombosis] • Arterial When would we not want clots to form?? • Certain people are at a higher risk for thromboembolism: Virchow triad for the pathophysiology of thrombus formation. http://emedicine.medscape.com/article/959501overview – Cardiovascular disease – Atrial fibrillation – Prosthetic device (i.e. replacement heart valve) – Post-surgery (i.e. hip/knee replacements) Thromboembolism in the U.S. • “Annually, more individuals may die from DVT complications than from the combination of AIDS, breast cancer, and motor vehicle accidents combined” – 900,000 to 2,000,000 VTE cases per year in U.S. – Estimates of death rates per year vary from 50,000 to 300,000 – 700,000 Strokes per year • 15% of strokes are in people with Atrial Fibrillation – 1.2 mil Heart Attacks per year • Help prevent thromboembolism with the antithrombotic drugs: Anticoagulants, Antiplatelets, Thrombolytics Anticoagulants Inhibit clotting factor activation reactions in the blood • CURRENT DRUGS – – – – – – – – • TARGETED FACTOR Unfractionated Heparin______________ Antithrombin (indirectly Xa and IIa) Low Molecular Weight Heparin________ Antithrombin (indirectly Xa and IIa) Lepirudin (DTI)____________________Thrombin (IIa) Bivalirudin (DTI) ___________________ Thrombin (IIa) Argatroban(DTI)____________________ Thrombin (IIa) Danaparoid_______________________ Antithrombin Drotrecogin Alfa____________________ Va, VIIIa Vitamin K antagonists (Warfarin)_______ Prothrombin (II), VII, IX, X NEW/ in DEVELOPMENT DRUGS – – – – – – – – – – – Fondaparinux_____________________Xa Idraparinux_______________________Xa SSR 126517______________________ Xa Rivaroxaban______________________ Xa Apixaban_________________________ Xa LY517717________________________ Xa YM150__________________________Xa DU-176b_________________________ Xa Betrixaban________________________ Xa Ximelagatran*_____________________ Thrombin (IIa) Dabigatran etexilate________________Thrombin (IIa) *taken off the market Italics are Oral Drugs Aside: other Anti-thrombotic drug types • Anti-platelet agents include: – – – – – Aspirin (acetylsalicylic acid) clopidogrel dipyridamole ticlopidine glycoprotein IIb/IIIa inhibitors • Thrombolytic (/fibrinolytic) drugs include: – – – – – – tissue plasminogen activator - t-PA - alteplase (Activase) reteplase (Retavase) tenecteplase (TNKase) anistreplase (Eminase) streptokinase (Kabikinase, Streptase) urokinase (Abbokinase) Heparin And other current Parenteral Anticoagulants Natural anticoagulation mechanisms • Prostacyclin: – • made by the endothelial cells and prevents platelets from collecting and secreting sticky substances Antithrombin, a plasma protein – • stimulated by Heparan sulfate proteoglycans from endothelial cells, inhibits coagulation factors of intrinsic and common pathways Activated plasma zymogen Protein C with cofactor protein S – • degrades certain cofactors and therefore greatly inhibits activation of prothrombin and factor X Tissue Factor Pathway Inhibitor (TFPI) – a lipoprotein that can inhibit tissue factor bound factor Va or VIIa http://en.wikipedia.org/wiki/Coagulation Basics of Heparin • Derived from mucosal tissues of slaughtered meat animals. Also exists in your body and is secreted form mast cells at the site of tissue injury • Increases Antithrombin activity. (Indirect inhibition method of IIa & Xa) • Usually intravenous adminstration • Glycosaminoglycan chains attached to a protein core = proteoglycans (750 kiloDaltons to 1000 kiloDaltons) • Low molecular weight heparin: different composition; more predictable; subcutaneous injection twice daily; use preferred over unfractionated heparin Action of Heparin and similar drugs Dark shaded region is a high-affinity pentasaccharide sequence 2: Unfractionated Heparin 3: Low-molecular weight Heparin 4: Fondaparinux (discussed later) Image from Sterling T. Bennett’s chapter on Monitoring Anticoagulant Therapy Crystal structure of the antithrombin-pentasaccharide complex Essentials of Glycobiology Second Edition Chapter 35, Figure 2 More about Heparin • Fast action intravenously or by injection (not absorbed through the stomach or intestinal wall) • peak after injection 2 - 4 hr • Complex metabolism (long chains broken up) • half life 1 - 5 hr; cleared by the reticuloendothelial system and some excreted in urine. • A few Drug-drug interactions • Toxicities: Bleeding & Heparin-Induced Thrombocytopenia Other Parenteral Anticoagulants • • • • • Lepirudin (DTI) derived from hirudin from leech salivary glands Bivalirudin (DTI) approved for use during heparin-induced thrombocytopenia (HIT) & percutaneous coronary interventions Argatroban (DTI) can be used in patients with risk of (HIT) Danaparoid no longer available in the U.S. Drotrecogin Alfa used in patients with sepsis; recombinant form of activated protein C that inhibits f Va and f VIIIa Dicoumarol Phenprocoumon Warfarin Sodium Vitamin K antagonists: Parent Molecules: 4-Hydroxycoumarin & indan-1,3-dione Oral Anticoagulants Acenocoumarol Anisindione Vitamin K antagonists Mechanism of Action • Some clotting factors need a carboxyl group added to their carboxyl-terminal glutamates after synthesis in the liver in order to be able to bind Ca++ during coagulation activation [these are called Vitamin K dependent clotting factors] • This γ-carboxylation reaction requires reduced Vitamin K, which leaves the reaction as a Vitamin K epoxide. • Vitamin K epoxide is then converted back to its reduced form via the enzyme vitamin K epoxide reductase and NADH • The Vitamin K antagonists inhibit the action of the reductase enzyme http://www.vet.uga.edu/VPP/clerk/Harrell/index.php http://tollefsen.wustl.edu/projects/coagulation/coagulation.html Vitamin K antagonists Effect on Coagulation • Vitamin K dependent clotting factors: Factors II, VII, IX, and X Intrinsic pathway Extrinsic pathway TF XIIa XII VIIa XIa IXa XI IX VIIIa X Xa Va Common pathway II (prothrombin) IIa (thrombin) Fibrinogen Fibrin XIII XIIIa Stabilized Fibrin Vitamin K antagonists History of Warfarin • 1930s: cows hemorrhaging after eating spoiled sweet clover silage • 1939: bishydroxycoumarin (dicoumarol) identified • 1948: potent form as rodenticide – Called Warfarin (Wisconsin Alumni Research Foundation) Anticoagulant in humans? No, too toxic!? • 1951: Army inductee’s failed attempt at suicide with high dose of warfarin rodenticide • Clinical use for over 60 years Vitamin K antagonists Warfarin • Adminstered orally, intravenously, or rectally • Bioavailabily nearly complete; absorption dampered by food • Peak concentration 2 - 8 hr • Binds to albumin 99% of time • Can cross placental barrier • Racemic mixture: S form by CYP2C9; R by CYP1A2, minor pathway CYP2C19, and minor pathway CYP3A4 • half-life: 25 - 60 hr; Excreted in urine and stool • Food-drug & drug-drug interactions: extensive!! • Toxicities: bleeding, fetal bone abnormalities Vitamin K antagonists Problems with Warfarin • Food and drug interactions • Genetic variation in metabolism • narrow therapeutic window dosage adjustments & freq. monitor with INR overlap with parenteral drugs • slow onset of action Newer Anticoagulants Targeting specific factors Factor Xa Inhibitors • Parenteral or Oral • Direct or Indirect mech. of inhibition Intrinsic pathway Extrinsic pathway TF XIIa XII VIIa XIa IXa XI IX VIIIa X Xa Va Common pathway II (prothrombin) IIa (thrombin) Fibrinogen Fibrin XIII XIIIa Stabilized Fibrin Factor Xa Inhibitors Fondaparinux • • • • Parenteral anticoagulant first selective factor Xa inhibitor approved by the FDA (2001) 55% better than enoxaparin (LMWH) at reducing risk of VTE synthetic pentasaccharide: “represents the oligosaccharide consensus sequence of heparin” • Indirect inhibition: binds to antithrombin and increases antithrombin’s affinity for factor Xa by 300-fold http://www.fda.gov/cder/foi/nda/2001/21-345_Arixtra_chemr.pdf Factor Xa Inhibitors Indraparinux & SSR 126517 • Hypermethylated form of fondaparinux = tighter binding to antithrombin • Status: phase III clinical trials • 80 hr half-life = subcutaneous injection once weekly • SSR 126517 is a biotinylated form of indraparinux, prepared to have an antidote (avidin) Factor Xa Inhibitors Oral factor Xa inhibitors • Developed off of success of fondaparinux • Can affect free factor Xa OR Xa bound to prothrombinase complex! • Many different drugs of this type being developed – Rivaroxaban – Apixaban – LY517717, YM150, DU-176b, and betrixaban Factor Xa Inhibitors Rivaroxaban & Apixaban Rivaroxaban Apixaban Company sponsor Bayer, Johnson & Johnson Bristol-Myers Squibb; Pfizer # clinical trials 21 15 Molecular weight 436 460 80% 50% Bioavailability Peak , half-life (hr) 3, 5-9 3, 9-14 metabolism CYP 3A4, CYP2J2, CYP-ind.mech. CYP 3A4, CYP-ind.mech. excretion 66% kidney, rest in feces 25% kidney, rest in feces Factor Xa Inhibitors Two synthesis schemes of rivaroxaban Direct Thrombin Inhibitors Intrinsic pathway Extrinsic pathway TF XIIa XII VIIa XIa IXa XI IX VIIIa X Xa Va Common pathway II (prothrombin) IIa (thrombin) Fibrinogen Fibrin XIII XIIIa Stabilized Fibrin Direct Thrombin Inhibitors Ximelagatran • First target-specific oral anticoagulant in trials • Ximelagatran is the oral prodrug of Melagatran • Hepatatoxicity – Did not receive FDA approval in 2004 – On the market in Europe but pulled in 2006 • ‘proof of principle’ – “efficacious” as warfarin – Wider therapeutic index – Little dosage adjustment/ no monitoring Direct Thrombin Inhibitors Dabigatran etexilate • Prodrug converted to Dabigatran (471 mw) by esterases in blood after absorbed in stomach in microenvironment from tartaric acid capsule • Peak 2hr; Half life 14 – 17 hr • Not metabolized by cytochrome system = no anticipated drug interactions • Farthest along in trials • History: – early 1990s: German scientists at Boehringer-Ingleheim began research – 1996 Synthesized novel drug – 1999 Phase I trials – 2001-3 Phase II trials – 2004-present Phase III trials – 2008 announced to be entering European market soon as Pradaxa® – RE-LY trial results in 2009 • Promising; improvement in liver safety Direct Thrombin Inhibitors Dabigatran etexilate clinical trial example “RELY: Randomized Evaluation of Long term anticoagulant therapy (RE-LY) comparing the efficacy and safety of two blinded doses of dabigatran etexilate with open label warfarin for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation Study Design: Prospective, multi-centre, randomized, open label, controlled parallel group, non-inferiority trial. Study Objective: Demonstrate that the efficacy and safety of two blinded doses of dabigatran etexilate in patients with non-valvular atrial fibrillation are non-inferior to warfarin treatment for the prevention of stroke and systemic embolism. Scope: A total of 15, 000 patients will be randomized from approximately 1,000 clinical sites within 44 countries. Patients will be randomized over a 2-year period with a minimum 1 year follow-up, maximum of 3 years and mean of 1.5 years of follow-up.” https://www.rely-trial.com/RelyWeb/resources/jsp/emergency/dabigatran_bg.jsp Summary Slide Intrinsic pathway Extrinsic pathway TF XIIa XII VIIa XIa IXa XI IX VIIIa X Xa Va Common pathway II (prothrombin) Vitamin K antagonists Heparin derivatives Factor Xa inhibitors Thrombin inhibitors IIa (thrombin) Fibrinogen Fibrin XIII XIIIa Stabilized Fibrin Future of Anticoagulants • Clinical trials of novel anticoagulants will continue • New drugs to be on the market soon but cost will determine how wide spread the use will be • Parallel development of f Xa inhibitors and direct thrombin inhibitors • Drugs with other targets (f VIIa - TF, f Va - VIIIa, f IXa) will go to trials • Utilize crystal structures/docking algorithms References • http://tollefsen.wustl.edu/projects/coagulation/coagulation.html (Great on blood coagulation) • http://www.accessdata.fda.gov/scripts/cder/drugsatfda/ (approved drugs) • • • • • • • • • • http://clinicaltrials.gov/ct2/search (searchable database for clinical trials) http://en.wikipedia.org/wiki/Coagulation http://my.clevelandclinic.org/drugs/antiplatelet_drugs/hic_antiplatelet_drugs.aspx http://www.vet.uga.edu/VPP/clerk/Harrell/index.php http://en.wikipedia.org/wiki/Thrombolytic_drug http://www.americanheart.org/presenter.jhtml?identifier=4451 http://www.natfonline.org/frequency_te.php http://emedicine.medscape.com/article/959501-overview https://www.rely-trial.com/RelyWeb/resources/jsp/emergency/dabigatran_bg.jsp Brunton, Lazo, Parker. Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 11th ed. Chapter 54: Blood Coagulation and Anticoagulant, Thrombolytic, and Antiplatelet Drugs” by Philip W. Majerus and Douglas M. Tollefsen.1467-1488. Bauer, Kenneth A. “New Anticoagulants.” Current Opinion in Hematology 2008, 15:509-515. Turpie, Alexander. “New oral anticoagulants in atrial fibrillation.” European Society of Cardiology, European Heart Journal 2007, 29:155-165. Esko, Jeffrey D and Robert J. Linhart. “Proteins that bind Sulfated Glycosaminoglycans.” accessed online from Essentials of Glycobiology 2nd edition. CSH Press 2009. <http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=glyco2&part=ch35> “Rivaroxaban.” Prous Science. Drugs of the Future 2006, 31 (6): 484-493. • • • •