Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of proton pump inhibitors wikipedia , lookup
Orphan drug wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Psychopharmacology wikipedia , lookup
Compounding wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Plateau principle wikipedia , lookup
Prescription costs wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
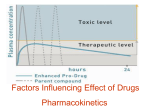
Pharmacokinetics Ed Bilsky, Ph.D. Department of Pharmacology University of New England Pharmacokinetics vs. Pharmacodynamics • Pharmacokinetics describes the movement of the drug (and its metabolites) through the body during the processes of absorption, distribution and elimination – Relates the dose of the drug administered to the concentration that is achieved at the site of action – “The actions of the body on the drug” • Pharmacodynamics describes the relationship between the concentration of the drug at the site of action with the observed effect – “The actions of the drug on the body” Pharmacokinetics • Pharmacokinetics processes of absorption, distribution and elimination will determine how rapidly, in what concentration, and for how long, the drug will appear at the target site • “Standardized” doses may have to be adjusted in individual patients in response to various factors – Physiology (age, sex, ethnicity) – Pathology (diseases of the liver, kidney, etc.) • For a particular drug, the parameters of clearance and volume of distribution are especially sensitive to changes in these factors Pharmacokinetics Pharmacokinetic properties of selected drugs: Drug Oral availability % Urinary excretion % Plasma Binding Half-life (hours) Acetaminophen 88 3 0 2 Diazepam 100 1 99 43 Digitoxin 90 32 97 161 Lithium 100 95 0 22 Morphine 24 4 35 1.9 0 79 25 1.1 Vancomycin Pharmacokinetics Administration Absorption Routes: topi cal enteral parenteral Central Compartment Plasma free drug Protei n bound drug Metaboli sm (li ver, etc.) Figure 1. An overview of drug disposition Eli mination (ki dney, GI tract) Distribution Site of action Ti ssue reservoi rs Enteral Absorption Administration of the drug into the alimentary tract: 1. Oral – most common route of administration – important considerations • • • • state of consciousness nausea and vomiting stomach contents and acid environment affect pharmacokinetics first pass effect 2. Rectal – decreased first pass effect – absorption can be variable 3. Sublingual Oral administration Sublingual administration Buccal cavity Venous return from buccal cavity Hepatic vein Stomach Portal vein Intestine LIVER Bile duct Rectum Venous return from rectum Rectal administration Vena cava Parenteral Absorption Injection of the drug into the skin, muscle or blood: 1. Subcutaneous (under the skin) – small drug volumes and slow absorption 2. Intramuscular (into the muscle) – larger drug volumes and faster absorption 3. Intravenous (into the vein) – quickest delivery route, easier to maintain steady drug concentrations Miscellaneous Routes 1. Inhalation/Pulmonary – typical rapid onset, no first pass effect, targeted delivery 2. Topical – Transdermal • requires the drug to be absorbed across the dermis • usually a very slow absorption and a prolonged duration of action (fentanyl patch) • no first pass effect – Mucous membranes – Eye drops Drug Formulation Drug formulations can modify the pharmacokinetics of drug delivery • sustained release products – controlled-release theophylline for asthma • protective coating – enteric coated aspirin • selective tissue targeting – ointments Drug Formulation Plasma Gastrointestinal Tract Solid dose forms Oral suspension Release Dissolution Oral solution Absorption Arthrotec Rate of Absorption for Various Preparations • Liquids • Suspension solutions Fastest • Powders • Capsules • Tablets • Coated Tablets • Enteric-coated tablets Slowest Factors Affecting Drug Absorption • Chemical properties – – – – chemical structure – solubility (structure) molecular weight (lithium to tPA) solubility partition coefficient (lipid solubility– charge Or no charge) QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture. • Physiological variables – gastric motility – empty vs full stomach – pH at absorption site – pH at tissue can affect pharmacokinetics/ dynamics – affects ability to get into cell (eg local anesthetics) – surface area at absorption site – more readily absorbed – blood flow – presence or absence of food (affects transit in intestine, what you eat can affect drugs (chelating) Factors Affecting Drug Absorption Process Outside Passive diffusion Drug (D) Inside Membrane D Facilitated diffusion D Active transport D ATP/Gradient Diffusion • The spontaneous movement of molecules or other particles in solution to reach a uniform concentration throughout the solvent – based on random thermal motion of the particles – does not require the input of external energy Initial Conditions A B Equilibrium A B Diffusion Fick’s Law of Diffusion: DC x A x Perm. Coefficient Flux = (molecules/unit time) Thickness • In the case of diffusion across membranes, the lipid solubility of the compound is a major determinant of mobility of the drug Drug pKa • Most drugs are either weak acids, weak bases or are amphoteric (both –side groups with both properties) • A drug’s pKa value represents the pH at which 50% of the molecules in solution are ionized • Drugs will tend to exist in the ionized form when exposed to their pH-opposite environment – acids are increasingly ionized in a basic environment – bases are increasingly ionized in an acid environment Henderson-Hasselbalch Equation pH = pKa - log log [Protonated] [Unprotonated] [Protonated] [Unprotonated] = pKa -pH pKa and Drug Diffusion • Aspirin is a weak acid (pKa=3.0) – in the stomach, aspirin is roughly in equilibrium between its ionized and unionized forms – aspirin is absorbed across the lining of the stomach stomach environment (pH ~ 2-3) COO - COOH OCOCH Unionized 3 OCOCH Ionized 3 + H+ Drug Ionization as a Function of pH 100 100 Weak Acids: Aspirin Phenobarbital Morphine Diazepam 75 % Ionized % Ionized 75 50 50 25 25 0 Weak Bases: 0 3 6 pH of Solution 9 12 0 0 3 6 pH of Solution 9 12 pKa and Drug Diffusion • Differences in the pH of body fluids can lead to drug “trapping” in certain compartments – lead to changes in absorption and/or elimination Body fluid Range of pH Stomach 1.9-2.6 Intestine 6.4-7.6 Urine 5.0-8.0 Breast milk 6.4-7.6 Drug Persistence in the Blood Once the drug has been absorbed into the blood, a number of factors can affect bioavailability 1. Drug metabolism by enzymes in the blood – cholinesterases (succinylcholine duration of action < 8 minutes – mimics Ach/muscle blocker) 2. Binding to blood proteins – albumin (acidic drugs) – Alpha-1 acid glycoprotein (basic drugs) Lipid Solubility • Affects diffusion and distribution of the drug – passage across the blood-brain barrier (heroin versus morphine) • Highly lipid soluble drugs tend to accumulate in body fat – diminishes the effect the drug has on the CNS – slowly released from the fat over a long period of time Blood Brain Barrier capillary in the supraoptic nucleus capillary in the subfornical organ Drug Metabolism • Biotransformation – modifies the chemical structures of compounds – liver >> kidney > other selected tissues – in general, makes the compounds more water soluble to enhance renal excretion – typically inactivates compounds (important exceptions) Biotransformation • Biological transformation of a drug into: – a more water soluble compound – an inactive metabolite – an active metabolite Phase I Phase II Oxidation Reduction Hydrolysis Chemical reactions that change the molecule Conjugation Addition of another molecule (e.g., glucuronidation) Biotransformation % Drugs Metabolized by Each Cytochrome Isozyme 100 75 50 25 0 CYP3A4 CYP2D6 CYP2C9/10 CYP2C19 CYP2E1 CYP1A2 Cytochrome P450 Isozyme Biotransformation Formation of Active Metabolites Drug Active metabolite diazepam desmethyldiazepam imipramine desmethylimipramine Prodrug Active metabolite codeine morphine sulindac sulindac sulfide Factors Affecting Drug Metabolism • Induction of Enzyme Systems – alcohol and phenobarbital • Inhibition of Enzyme Systems – disulfiram and alcohol • Sex – levels and distribution of alcohol dehydrogenase Metabolic Pathway for Alcohol Ethanol CH3CH2OH alcohol dehydrogenase CH3CHO Acetaldehyde aldehyde dehydrogenase Acetyl Coenzyme A energy CO2 citric acid cycle H2O Metabolic Pathway for Alcohol CH3CH2OH alcohol dehydrogenase disulfiram (Antabuse) CH3CHO aldehyde dehydrogenase Acetyl Coenzyme A energy CO2 citric acid cycle H2O Enzyme Inducers and Inhibitors Inhibitors ethanol phenobarbital omeprazole smoking Inducers cimetidine erythromycin quinidine grapefruit juice First-Pass Metabolism after Oral Administration of a Drug, as Exemplified by Felodipine and Its Interaction with Grapefruit Juice Wilkinson, G. R. N Engl J Med 2005;352:2211-2221 First-Pass Metabolism after Oral Administration of a Drug, as Exemplified by Felodipine and Its Interaction with Grapefruit Juice QuickTime™ and a decompressor are needed to see this picture. Wilkinson, G. R. N Engl J Med 2005;352:2211-2221 QuickTime™ and a decompressor are needed to see this picture. Drug Excretion • Many drugs are excreted via the urine – blood concentration of the drug determines how much drug gets filtered by the kidneys --> how much drug is eliminated (important for first order kinetics) – some drugs are excreted unchanged in the urine • Other sites of excretion – feces – lungs – sweat Drug Excretion • Urine pH can alter the excretion rate of some drugs – varies between 5.0 and 8.0 • Weak acids are excreted more readily in alkaline urine and more slowly in acidic urine • Weak bases are excreted more readily in acidic urine and more slowly in alkaline urine Phenobarbital (weak acid, pKa 7.2) nonionized ionized Urine pH = 7.2 Urine pH = 8.2 Reabsorption alkalinize the urine (sodium bicarbonate) Bladder Bladder Clinical Pharmacology • A relationship exists between the concentration of a drug at the site of action and the beneficial and/or toxic effects produced by that drug • Application of pharmacokinetic knowledge helps the clinician to achieve a desired beneficial effect with minimal adverse effects • In practice, these applications are most critical when the therapeutic index of a drug is very low, or when there is a large variation in response of different patients to a given dose of a drug Volume of Distribution • Relates the amount of drug in the body to the concentration of the drug in blood or plasma Vd = Amount of drug in body Concentration of drug • Examples: – warfarin = 9.8 L/70 kg – fluoxetine = 2500 L/70 kg blood Clearance • The factor that predicts the rate of elimination in relation to the drug concentration CL = Rate of elimination Concentration of drug • May be defined with respect to blood, plasma or unbound drug in the plasma water Clearance • Elimination of a drug from the body is the sum of all routes of elimination CL systemic = CL renal + CL liver + CL • Examples – Digitoxin, CL = 0.234 L/h/70 kg, t1/2 = 161 – Atenolol, CL = 10.2 L/h/70 kg, t1/2 = 6.1 – Acetaminophen, CL = 21 L/h/70 kg, t1/2 = 2 other Downloaded from: StudentConsult (on 30 January 2006 03:27 AM) © 2005 Elsevier Volume of Distribution and Clearance Katzung, 3-2 Rate of Elimination • For most drugs, clearance is constant over the plasma or blood concentration range encountered in clinical settings – elimination is not saturable • This is referred to as first-order elimination Rate of elimination = CL x Concentration Clinical Example • Determine rate of elimination for acetaminophen • Calculate a typical dose for acetaminophen – oral bioavailability and plasma protein binding • Determine total body water and concentration after a typical dose • Compare calculated concentration with toxic concentration – What is the therapeutic index for acetaminophen? Capacity-Limited Elimination • Some drugs exhibit capacity-limited elimination – phenytoin, alcohol, aspirin CL = Vmax x C Km + C • When C >> Km, the elimination rate becomes nearly independent of drug concentrations – zero-order kinetics Clinical Example J.B., a 25 year old medical student, ingests typical dosages of acetaminophen, diazepam and ethanol on three consecutive weekends. He weighs 100 kg and has a body-fat content of less than 10% • What are the approximate concentrations attained in the body for each of these compounds? • For the ethanol example, what does this come out to on a molar basis? • What if a middle-age professor (100 kg, bodyfat >40%) drank the same amount of alcohol, what would his blood alcohol level be at? Flow-Limited Elimination • Some drugs are cleared very readily by the organ of elimination (e.g., morphine) – most of the drug is eliminated from the blood during the first pass of the drug through the organ • Elimination of these drugs will depend primarily on the rate of drug delivery to the organ – rate of elimination will be affected by disease processes that affect blood flow and the organs capacity to biotransform the drug Half-Life • Half-life (t1/2) is the time required to change the amount of drug in the body by one-half during elimination – simplify by assuming the body is a single compartment t1/2 = 0.7 x Vd CL • Disease states can affect both the volume of distribution and clearance Katzung, 3-3 Bioavailability • Defined as the fraction of unchanged drug reaching the systemic circulation following administration Concentration, g/ml 40 To determine Foral: i.v. AUC = [drug] x time = mg•hr•ml-1 30 oral 20 1. Measure AUCi.v. 2. Measure AUCoral 10 AUCoral Foral = AUCi.v. 0 0 2 4 6 Hours 8 10 For drug given i.v., F = 1.0 For other routes, F < 1.0 Bioavailability • Extent of absorption – gut metabolism – too lipophilic or too hydrophilic – effects of P-glycoprotein • First-pass elimination – portal blood delivers the drug to the liver prior to distribution to the systemic circulation • metabolism • excretion into the bile Extraction • The effect of first-pass hepatic elimination on bioavailability is expressed as the extraction ratio ER = CLliver Q Q = hepatic blood flow • The systemic bioavailability of the drug (F) can be predicted by the extent of absorption (f) and the extraction ration F = f x (1 - ER) Katzung, 3-3 Delayed Drug Effects • Changes in drug plasma levels are not always an accurate estimate of changes in drug effect • Some drug effects are delayed due to the time lag between the rise in plasma concentrations and the time needed for the drug to distribute to the site of action • Other drug effects require changes in gene expression and protein synthesis to occur before becoming manifest • Another example is the effects of warfarin on blood clotting-decreased synthesis of clotting factors occurs immediately but existing factors are somewhat stable Dosing Intervals QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture. Figure 3-6, Katzung Katzung, 3-3 Dosing Intervals • Significant differences can occur between continuous versus intermittent dosing regimens even though the average steady state levels of the drug are the same • Renal toxicity of gentamicin is greater with continuous infusion versus intermittent dosing Katzung, 3-3 Target Concentrations • For most drugs, there are specific target concentration ranges that will provide a desired therapeutic effect • The goal of the dosing regimen is to keep drug levels in the target range for the entire interval between doses • At steady state, the dosing rate must equal the rate of elimination Dosing rate = Rate of elimination = CL x TC Katzung, 3-3 Maintenance Dose • If bioavailability is less than 100%, then this must be taken into account Dosing rateoral = Dosing rate/Foral • When giving intermittent doses, the maintenance dose is calculated as: MD = Dosing rate x Dosing interval Katzung, 3-3 Theophylline Example • A 18 year old female presents to the ER with an acute asthma attack. The physician wants to administer theophylline intravenously. • What are the clearance and target concentration values for theophylline? • Dosing rate = CL x TC = 2.8 L/h/70kg x 10 mg/L = 28 mg/h Katzung, 3-3 Theophylline Example • The intervention is successful and the physician now wants to initiate oral therapy and maintain the target concentration. How would this be accomplished? • What is the oral bioavailability of theophylline? • What is the desired dosing interval? • Maintenance dose = (Dosing Rate/F) x Dosing Interval • (28 mg/h ÷ 0.96) x 12 hrs = 350 mg Katzung, 3-3 Loading Dose • From Figure 3-6, when using maintenance dosings, it takes 4-5 half-lives to reach steady state regardless of if it is through intermittent dosing or continual infusion • A faster rate of onset of drug effect may be required, especially in the case of drugs with long half-lives Loading Dose = Vd x TC • The rate of distribution into different compartments may need to be considered to avoid excessive drug concentrations and toxicity --> slower infusion rate Katzung, 3-3