Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
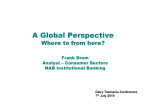
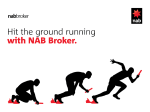
DO EXIST EVIDENCES CONCERNING RELATIONSHIP BETWEEN AN OCCURENCE OF NAbs AND EFFICACY OF INTERFERON´S THERAPY IN MS? Bartko D., Čombor I., Bošelová M. Institute of Medical Sciences, Neurosciences and Military Health, Central Military University Hospital, Faculty of Health Sciences, Ružomberok, Slovak Republic, NAbs occur with all current immunomodulatory therapies BUT it is difficult to compare the influence of NAb on drug effectiveness (Oger, Cantillon 2006) Many analyses showed that NAb to some INFs are transient, e.g. the incidence of NAb to Betaseron peaks until approx 12 - 18 months of treatment AND THEN NAb disappear over time The transient nature of NAb to INF has been reported by many authors, recently by Sorensen et al. (2006), and most recently also by Oger and Cantillon (2007). The median NAb titer peaked at months 18. The highest median titer was 48, which is not considered as high (Oger, Cantillon 2006) Median (Q1–Q3) NAb Titre at Each Timepoint The number of patients tested is given under the x-axis Generally, the recent data on NAb to INF suggest that treatment decision (when NAbs occure) „TO STOP OR TO CONTINUE WITH INF TREATMENT“ should be based on the patient´s CLINICAL COURSE AND NOT on the NAb status Neutralizing antibodies (NAbs) arising during IFN therapy CAN AFFECT bioavailability and production of interferon-induced biological markers. This may impact on clinical and MRI outcomes, although this hypothesis is CONTROVERSIAL. In one long-term evaluation of NAbs in pts treated with INF-beta NAb ferquency was associated with an EARLIER REVERSION to NAb - negative status and DID NOT AFFECT clinical response to treatment (Ricci et al.2006) How can we explain this? It can be explain • by induction or by reflection of increased immunological tolerance (B cell tolerance) or • by induction so-called habituation Three different INF products are registered for the treatment of RRMS. Recently (2004), selective monoclonal antibody adhesion molecule inhibitor was registered for the treatment of MS (Natalizumab) Their efficacy has been proven in many multicenter, controlled trials (IFNb MS Study GROUP 1993, PRISMS 1998 INCOMIN 2002 and others) Recombinant INFs beta are produced by different cell systems, which result in some differences in their aminoacide structure, molecular weight, degree of glycosylation and specific activity Each drug has been registered for use in different doses (30 μg, 22 and 44 μg and 250 and 375 μg) and different administration schedules (IM once a week, SC 3-times a week, SC every other day or IV once a month) Results of pharmaclogical and clinical studies suggest • a dose-response effect for beta interferon • for better effect when the drug is administered several times a week rather than only once a week (Deisenhammer et al.2000) • the effect of treatment on both CLINICAL AND MRI outcomes increased proportionally to the administered weekly doses (OWIMS Study, INCOMIN Study 2002) Effect of NAbs on Disability Mean change in EDSS NAb+ Patients Have Greater Disability Progression 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 NAb+ P=0.01 NAb- 0 6 12 18 24 30 36 42 48 Month NAb+ n= 26 26 26 26 25 26 26 20 14 NAb- n= 732 722 698 670 649 621 605 420 286 Kappos et al. Neurology. 2005;65:40. NAbs occur frequently in pts receiving IFN-beta for MS differently in different IFNs-beta BUT It is unclear whether occurrence of NAbs is PREDICTIVE for the persistence of NAbs during continued IFN-beta therapy. Some authors have shown that NAbs REDUCE the effect on relaps rates and MRI measures of disease activity (Rudick et al., 1998, Sorensen et al., 2003) The another studies have shown that NAbs MAY DISAPPEAR in a large proportion of NAb-positive pts after several months or years of continous therapy with high-dose IFN-beta-1b (Sorensen et al., 2003, Petkau et al., 2004) Reversion to NAb-negative Status or Decrease in NAb titer Over 4 years NAb titer changes (%, n/N) 250μg 375μg p Titer unchanged or 81 (21/26) 29 (2/7) increased Titer decreased or reverted to negative status 19 (5/26) 71 (5/7) 0.02 (Ricci et al., 2006) Reversion to NAb-negativity occurs • 28 NAb –positive pts were studied, • after 2 years, 43 negative, • Characteristics: % were NAb- – NAbs developed earlier, – lower titer of NAbs – more likely to have been treated with IFN-beta-1b than with IFN-beta -1a (Gneiss et al., 2004) In the most recent study (Goodin et al., 2006) it was shown that NAbs to IFN-beta-1b have no impact on clinical response in MS Cumulative probality of remaining NAb-negative. Significantly high proportion of pts treated with IFN-beta- 1b (Betaseron), and IFN-beta -1a (Rebif) and Avonex reverted NAb-negative status to Probability of NAB development (2 consecutive positive titers) •Avonex vs •Rebif and Betaferon: p<0.01 •NEUROLOGY 2005;65: It is important to stress that pts who have remained NAb - negative during the first 6 - 24 months of IFN-beta therapy only rarely develop NAbs (Soelberg Sorensen et al., 2005) The prevalence of NABs seems to vary widely among present three products and between studies On the contrary, the majority of pts, who had been NAb - positive from 12 through 30 months after start therapy, remaind NAb - positive THEREFORE NAbs should be measured in all pts treated with IFN-beta at least during the first 24 months of therapy If pts have been persistently NAb-negative for 24 months, measurments can be discontinued. Risk of becoming NAB-positive is negligible WHY SUCH CONTROVERSIAL RESULTS CAN BE FOUND? Because data from previous trials cannot be compared. The antibody titers were achieved with different assays and therefore the definitions of NAb-positive were different (PRISMS1998, PRISMS 2001) There is no internationally agreed standard method to test for NABs. Neutralizing assay are cell-based bioassays with inherent variability and THEREFORE assay interpretations are variable among different laboratories Of the available methods the antiviral cytopathic effect (CPE) is widely used and is recommended by the WHO BUT this method is time-consuming and relatively complicated The myxovirus resistance protein A (MxA) induction assay is an alternative method which is less time-consuming Three months ago very interesting data were published (Sominand at al 2007). The authors differentiate between * prevalence of NAb, and * immunogenicity of Nab * titer Duration of therapy 40 months PREVALENCE * Avonex: 13% * Betaferon: 43% * Rebif 22ug: 39 % * Rebif 44ug: 30% Austrian NAB project Preparation Patients tested for NAb NAb positive N (%) High titer N (%) IFNb-1b 239 74 (31 %) 43 (18 %) IFNb-1a i. m. 202 11 (5 %) 9 (4 %) IFNb-1a s. c. 405 118 (29 %) 83 (20 %) Total 846 203 (24 %) 135 (16 %) c2: p < 0.0001 Multiple Sclerosis 2006; 12: 731 - 737 IMMUNOGENICITY * Avonex * Betaferon induced LOW NAb titers * Rebif induced the highest titers i.e. it showed HIGHEST IMMUNOGENICITY (Sominanda et al., 2007) POSITIVITY was only moderatly increased in those showing WORSENING in comparison with other pts (without worsening). NAb TITER is less studied, despite it is MORE IMPORTANT marker than NAb prevalence From this point of view, I would like to stress that many of us have tendency to remain in –not always confirmed-DOGMAS, e.g. • • • • LP in MS can worsen the disease pregnancy can lead to worsening of MS MS belongs to demyelinizing disease at present: demyelinization axon and oligodendrocytes are involved intensive infammation etc. In 1980 in „Foreword“ of one monograph I have written: „It is dedicated to everyone who is looking for what is unexpected, to everyone who doesn’t suffer from common belief that whatever exists is all right, and to everyone who respects facts and mistrusts dogmas.” (Bartko, 1980) I have no reason to change this philosophy. Disbelief into dogmas is the basis of progress, belief into dogmas is the basis of stagnation CONCLUSIONS EFNS-AAN guidelines agreement 1. EFNS + AAN: Treatment of MS with IFNb is associated with the production of NAbs to the IFN molecule (Level A). 2. NAbs are not necessarilly the same. „NAbs differ“, 3. AAN: It is probable that the presence of NAbs, especially in persistently high titers, is associated with a reduction in the radiographic and clinical effectiveness of IFN treatment (Level B). 4. Controversy: for some IFN pts NAbs do not impact on clinical outcomes 5. If pts on IFN do get NAbs, they are transient 6. AAN: .......it seems clear that IFN-1a (as it is currently formulated for IM injection) is less immunogenic than the current IFN preparations 7. EFNS: There is general agreement that the IFN-b-1a (Avonex) is the least immunogenic. EFNS-AAN guidelines disagreement 8. AAN: insufficient information on NAb testing regarding * when to test, * which test to use, * how many tests are necessary, * and which cutoff titer to apply. EFNS-AAN guidelines 9. The answers (by EFNS): * when to test? 12 - 24 month! * which test to use? bioassay! * how many tests are necessary? at least two * and which cutoff titer to apply? minimum >20, for prognosis >100 10. The induction of NAbs against IFNs could be only relevant if they affect patient outcome 11. In almost 7000 pts across three continents, it was not found correlation between NAb status at any prevalence and treatment outcome (Real world data 2006) 12. In the majority of pts (92 %) who were not doing well on treatment, NAbs were not primary cause of treatment failure (Hurwitz, Pulmon, Real world data, 2006) 13. Therefore, the treatment decision should be based on clinical course and not on NAb status 14. No question about the negative effects of NAB is generally accepted 15. The immunogenicity is still the most important issue and needs to be considered when chosing a IFNb preparation To all my friends and participants: I am grateful...