Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Radiographic Anatomy
Digestive System
Educational Objectives
By the end of this lecture you should be able to:
• Identify the anatomical parts of the digestive system on
diagrams and radiographs.
• Identify the relations between the different parts of the GIT
• Explain how to hang GIT radiographs on the view box
•
State and locate the surface land marks associated with the
abdomen.
References
1. Text book of radiographic positioning and related anatomy; by
Kenneth L.Bontrager,6th edition.
2. Introduction to Human Anatomy and Physiology: by Eldra
Pearl Solomon:W.B.Saunders Company
3. Handbook of Anatomy and physiology for Students of Medical
Radiation Technology: Mallett.M:Jaspar
Websites
http://www6.district125.k12.il.us/science/anatomy/
http://www.innerbody.com/htm/body.html
http://www.e-radiography.net/
http://www.getbodysmart.com/index.htm
4
Digestive System
(gastrointestinal; GI tract)
–
Stomach
A. Fundus
(fluid level seen in erect position)
A. Body
B. Pyloric Antrum
–
Small intestines (small bowel)
A. Duodenum ("c" shape; bulb)
B. jejunum
C. ileum
Digestive System
(gastrointestinal; GI tract)
Large intestine (colon)
A.
B.
C.
D.
E.
F.
G.
H.
Caecum (valve; appendix)
Ascending colon
Hepatic flexure
Transverse colon
Splenic flexure
Descending colon
Sigmoid colon (flexure)
Rectum and anal canal
Accessory GI tract organs
A.
B.
C.
Salivary glands
Liver &Gall bladder
Pancreas
Quadrants & Regions of the abdomen
• Abdomen divisions
4 Quadrants (clinically)
9 Regions (anatomically)
Quadrants & Regions of the abdomen
MSP: mid-sagittal plane
TUP: transumblical plane (L4/5)
RLL: right lateral plane
LLL : left lateral plane
TPP: transpyloric plane (L 1)
TTP: transtubercular plane (L 5)
Regions of the abdomen
Digestive System
(I): Alimentary canal:
– 9 m length
– Extend from mouth to anus
►Oral cavity
►Pharynx
►Esophagus
►Stomach
►Intestine (small & large)
(II): Accessory organs:
– Salivary glands
– Pancreas
– Liver and biliary system
Pharynx
◙ Levels : from skull base to level of C-6 (13 cm).
◙ 3 parts:
(I): Nasopharynx:
•
•
•
•
•
Skull base to the level of soft palate
Anterior: nasal cavity (posterior nares)
Inferior: nasopharyngeal isthmus
Lateral wall: opening of auditory tube
Roof: adenoid
(II): Oropharynx:
• Level of soft palate to tip of epiglottis
• Anterior: oropharyngeal isthmus
(III): Laryngopharynx:
• Tip of epiglottis to level of C-6
• Pyriform fossa
Esophagus
◙ Levels : from C-6 to T-11 (25 cm).
Normal points of narrowness: (1) Level of cricoid cartilage; (2) Level of left main bronchus;(3)
Passing through the diaphragm. Venous drainage of the lower oesophagus form a point of
communication between portal and systemic veins; any obstruction of the portal venous system
may lead to oseophageal varices.
◙ Relations: (3 areas)
(I): In the neck:
• Anterior: trachea, thyroid
• Posterior: cervical vertebrae
• Lateral: common carotid artery
(II): In the thorax:
• Anterior: trachea, Lt. main bronchus, Lt. atrium
• Posterior: thoracic vertebrae, thoracic duct, descending aorta
• Lateral:
– Right side: azygous vein, right lung
– Left side:
• Superior med.: Lt. subclavian artery, aortic arch, Lt. lung
• Inferior med.: descending aorta, Lt. lung
(III): In the abdomen: 1-3 cm ; the phrenic ampulla lies just above the
cardia and may simulate hiatus hernia. The abdominal part is called
(submerged segment) and help to prevent reflux from the stomach.
Other factors: Acute gastro-oesophageal angle,pressure of right crus
of the diaphragm and intrinsic muscles sphincter.
Stomach
◙ Shape: J-shaped, but may varies (volume, position, resp., build)
◙ 2 Orifices:
1.
2.
Cardiac
Pyloric
◙ 2 Curvatures:
1.
2.
Lesser
Greater
◙ 3 Parts:
1.
Fundus (air bubble)
2.
3.
Body
Antrum
◙ Mucosa: gastric rugae
- Longitudinal: on lesser curvature
- Random (mosaic): elsewhere
◙ Muscles:
1.
2.
3.
Outer: longitudinal
Inner: circular
Innermost: oblique
Relations of the Stomach
◙ Anterior:
–
–
–
–
Diaphragm
Left lobe of the liver
Left costal cartilage
Anterior abdominal wall
◙ Posterior (stomach bed):
–
–
–
–
–
–
Diaphragm
Left suprarenal gland
Left kidney
Pancreas
Spleen and splenic artery
Transverse colon and Splenic Flexure.
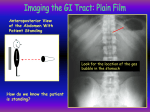
◙ Stomach lie: The fundus of the stomach is located posterioly while the pyloric
antrum is very near to the anterior abdominal wall; so with barium studies(1) In the
erect position: Air fluid level seen.(2) Supine: barium fill the fundus while pyloric
region is seen in double contrast.(3) Prone: barium fill the pylorus while the fundus is
seen in double contrast.
◙ Incisura: is that part of the stomach where there is sudden change in the plan of the
stomach from the vertical to the horizontal; it help to show whether the stomach is
eutonic, hypertonic or hypotonic according to its level in comparison with the 1st part
Small intestine
◙ Extension:
From pyloric orifice of stomach to ilio-caecal valve
◙ Length:
6 meters (range, 3-10)
◙ 3 Parts:
1.
Duodenum
2.
Jejunum
3.
Ileum
◙ Movements:
1.
Rhythmic
2.
Pendular
3.
Peristaltic
Duodenum
◙ C-shaped around the head of pancreas
◙ The shortest
◙ The widest
◙ 4 parts:
1.
Duodenal bulb: 2 inches, level of L-1, conical shape
2.
Descending: 3 inches, level of L-2
3.
Transverse: 4 inches, level of L-3
4.
Ascending: one inch, level of L-2
NB: 1. Duodenal bulb (Cap): is a common site of ulcers. It likely seen better in the right
anterior oblique.
2. Descending part: forms a curve around the head of the pancreas; the common bile
duct and the pancreatic duct open by a common opening (ampulla of Vater) =
{duodenal papilla} : through it. The opening is surrounded by sphincter of Oddi.
3. During contrast examination; barium reach the duodenal cap after 5minutes, delay
emptying more than 15 minutes may be due to obstruction.
Relations of the Duodenum
1.
Duodenal bulb:
–
Superior and anterior: liver and
gall bladder
–
Inferior: head of pancreas
–
Posterior: common bile duct,
portal vein
2.
Descending:
–
Posterior: right kidney
–
Medial: head of pancreas
–
Lateral: colon (HF)
3.
Transverse:
–
posteriorly crosses (Rt. Psoas
muscle, IVC, aorta)
4.
Ascending:
–
Posterior: lt. Psoas, lt. renal
vein, inferior mesenteric vein)
–
Anterior: transverse colon
Small intestine: 6-7 m surrounded by the
peritoneum ,so it is freely mobile
Large intestine
◙ Length:
• 1.5 m
• Extend from ileum to anus
• Characteristic shape:
Haustrated appearance
caused by the longitudinal
Muscle fibers being shorter
Than the circular muscle
Fibers; they run usually in
Three bonds called:
taenia coli.
Large intestine
Parts
◙ Caecum:
◙ Colon:
◙ Rectum:
◙ Anal canal:
Caecum & Colon
◙ Caecum:
– 6 cm long,
– The widest (7.5-9 cm)
– Ilio-caecal valve (ICV):
posteromedial aspect
Appendix :
– 12-24 cm length,
retrocaecal (75%)
Caecum & Colon
◙ Colon:
Ascending:
– 15 cm length, HF ?
Transverse:
– 50 cm length, SF,
transverse mesocolon
Descending:
– 25 cm length, pelvic brim
Sigmoid colon:
– 40 cm length, S-shaped
– Most movable ; may be
Too long
Rectum & Anal canal
◙ Rectum:
– Level of 3rd sacral V. (2 cm ant. to tip of coccyx)
– 12 cm length
– S-shaped (upper, middle and lower thirds), valve of Houston
– Lower third: no peritoneal cover, dilated (rectal ampulla)
– Pre-sacral space: it is the space between the rectum and the sacrum(0.61.2cm)
◙
Examined by the lateral view during barium enema studies to detect tumors ,
crohn’s disease and ulcerative colitis.
Anal canal:
– Right angle with rectum
– Sphincters: internal (involuntary), external (voluntary)
– NB: The lower part of the rectum and the anal canal form two antero-posterior
curves (S-shape) this fact must be remembered when a rectal tube or enema is
inserted to avoid serious injury. This area also have rich supply with vagus nerve;
so sever stretch or extreme temperature may lead to shock.
Rectum & Anal canal
Biliary System
◙ Gall
Bladder:
◙ Biliary
Ducts:
Gall Bladder
◙ Pear-shaped sac
◙ Capacity: 50 cc (store conc. Bile secreted by the liver.
◙ Site: inferior surface, right lobe of the liver ; there is a wide range of variation of the gall
bladder position from the 1st lumber vertebra to the level of the 5th lumber vertebra ;
due to this position ; gall bladder stones overlaps the same area of right renal stones .
Right lateral view may help to differentiate since gall bladder stones will be thrown
anteriorly. NB: 15% only from gall bladder stones are radio-opaque.
Mechanism of bile secretion: Gall bladder contracts and secrete bile under the effect of
cholecystokinin enzyme stimulated by the presence of fats in the stomach.
◙ Size: 10 cm length, 3 cm width
◙ Parts:
1.
2.
3.
Fundus: anterior abdominal wall, 9th costal cartilage
Body: upward, backward and to the left
Neck:
•
Upward and forward, then sharply downwards
•
S-shaped,
•
Cystic duct (3 cm length),
•
Mucosa: spiral valve
Biliary Ducts
◙ Hepatic ducts: right and left
◙ Common hepatic duct: 3 cm length
◙ Common bile duct:
– Common hepatic + cystic duct
– 7 cm length
– Relations:
• Supra-duodenal part: in front
of portal vein
• Retro-duodenal: first part of
duodenum
• Retro-pancreatic:
– Unites with pancreatic duct:
enter 2nd part of duodenum
Pancreas
• 5" long / 1" thick
• Head close to curve in
•
•
C-shaped duodenum
pancreatic duct joins
common bile duct from
liver
Opens 4" below
pyloric sphincter
Regions:
Head, body, tail
AP ABDOMEN
STOMACH
COLON
SM. BOWEL
Normal abdominal gas pattern with air in the stomach and
scattered non-distended loops of large and small bowel.
Barium swallow, esophagus.
Oblique view
The normal impressions made by :
(A) aortic arch,
(B) left mainstem bronchus, and
(LA) left atrium on the esophagus.
Barium Meal
FUNDUS
DUODENUM
ANTRUM
BODY
JEJUNUM
C-LOOP
NORMAL
GASTRIC
ANATOMY
SPLENIC
FLEXURE
HEPATIC
FLEXURE
Barium Enema
DESENDING COLON
TERMINAL ILEUM
CECUM
NORMAL
COLON
CT abdomen
CT abdomen